
Abstract
A patient with newly-diagnosed HIV infection and biopsy-proven cerebral toxoplasmosis was treated with sulphadiazine and pyrimethamine. Despite adequate hydration and daily examination of urine for sulphadiazine crystals obstructive uropathy due to bilateral ureteric stones with hydronephrosis occurred, resulting in rapid onset renal failure. Sulphadiazine was discontinued and clindamycin was substituted. With intravenous fluid hydration and bilateral nephrostomies the urolithiasis resolved. This case serves to remind clinicians of the need for vigilance when treating cerebral toxoplasmosis with sulphadiazine, in order to avoid this potentially serious complication of treatment.
INTRODUCTION
Early in the HIV pandemic, a new role emerged for sulpha drugs in the treatment of common opportunistic infections, such as toxoplasmosis, and clinicians became familiar with management of sulphonamide-induced nephrotoxicity. These side-effects had initially been recognized with widespread use of sulpha drugs during the 1940s and 1950s 1–3 after which their popularity declined in favour of ‘safer’ antibiotics. 4 First-line therapy for cerebral toxoplasmosis remains sulphadiazine and pyrimethamine, given for a minimum of six to eight weeks and for longer if clinical and radiological response is slow. 5 A reduction in the prevalence of HIV-related opportunistic infections resulting from the introduction of highly active antiretroviral therapy (HAART) 6 and the goal of providing patient-friendly acute care in the community setting make it imperative that clinicians are familiar with use of sulpha drugs and their side-effects.
We describe a patient with newly-diagnosed HIV infection and biopsy-proven cerebral toxoplasmosis treated with sulphadiazine. Despite adequate hydration, obstructive uropathy with rapid onset renal failure occurred. With discontinuation of sulphadiazine, intravenous fluid hydration and bilateral nephrostomies the urolithiasis resolved.
CASE REPORT
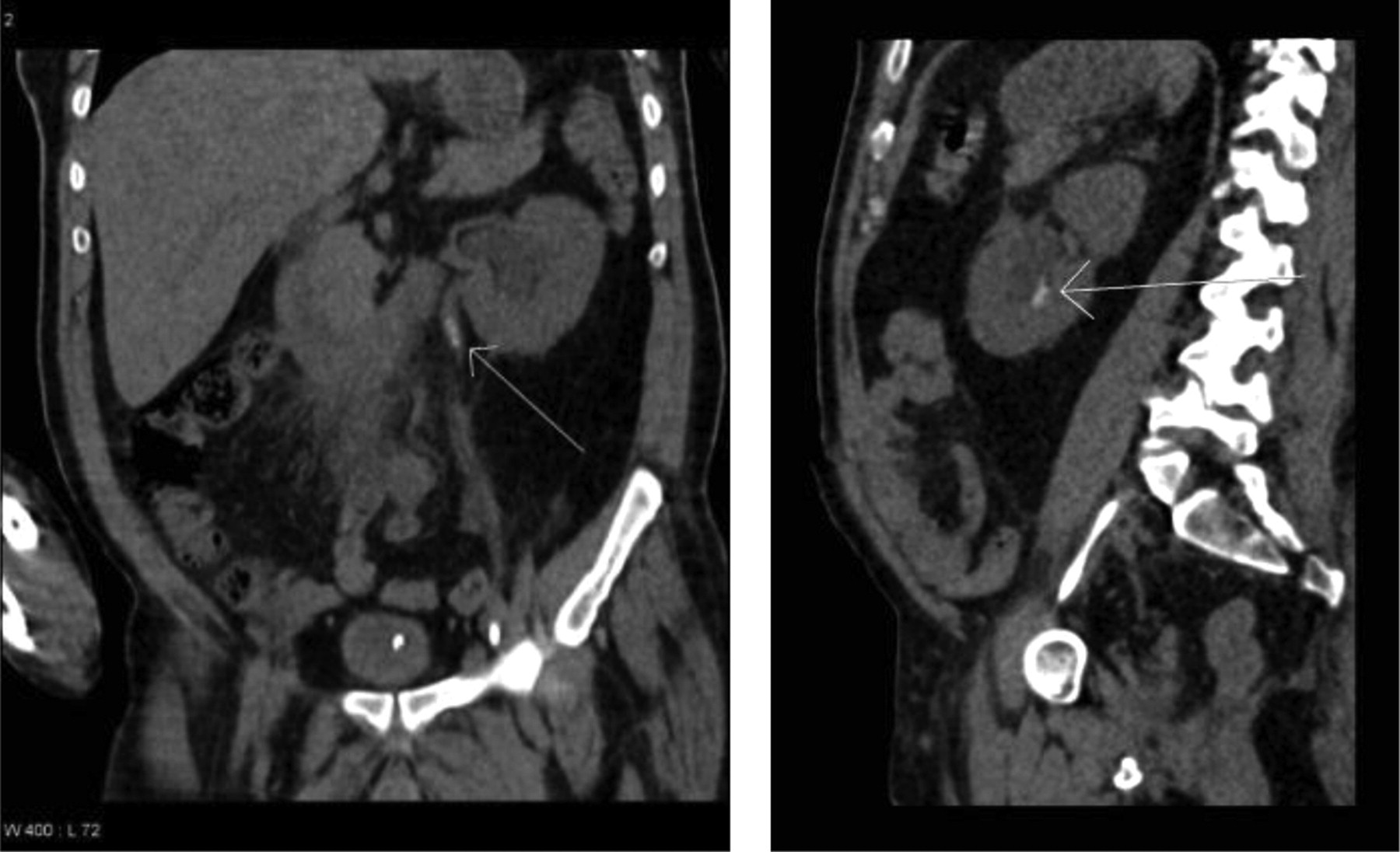
A 55-year-old cigarette smoker with longstanding hypertension and type II diabetes mellitus presented with left-sided weakness and facial palsy following a grand mal fit. Initial blood biochemistry (C-reactive protein, renal and liver function tests) and haematology (full blood count, erythrocyte sedimentation rate) were unremarkable but cranial computed tomography (CT) imaging showed a heterogeneously enhancing right fronto-parietal lesion, with surrounding oedema and mid-line shift. The appearances were thought to represent a metastasis. A CT scan of the chest, abdomen and pelvis (to identify a primary lesion) was normal (Figure 1). Tumour markers (carcino-embryonic antigen, cancer antigen [CA] 19–9 and CA 125, alphafetoprotein, human chorionic gonadotrophin) were negative. Cranial magnetic resonance imaging (MRI) showed left frontal and temporal lobe lesions in addition to the right fronto-parietal lesion seen on CT scanning. Histology of a stereotactic brain biopsy of the right fronto-parietal lesion showed cerebral toxoplasmosis and treatment (sulphadiazine 2 g six-hourly with pyrimethamine 50 mg once daily) was started. An HIV test was positive; CD4 count = 20 cells/μL, viral load = 270,000 copies/mL.

Coronal (left) and sagittal (right) reformatted images of a post-contrast computed tomography scan of abdomen and pelvis showing no renal calculi. The high density in the renal collecting system is iodinated contrast
Postoperatively the patient was drowsy and required naso-gastric feeding and intravenous fluids. Despite careful fluid management and daily visual examination of urine for crystals, his renal function deteriorated suddenly after 13 days of sulphadiazine therapy; urea = 8.9 (normal = 1.7–8.3) mmol/L and creatinine = 259 (normal = 49–92) μmol/L), peaking at 22.1 mmol/L and 610 µmol/L, respectively, on day 16.
CT imaging of kidney, ureters and bladder (interval = 22 days after the first CT scan) showed bilateral ureteric stones (largest = 7 mm) and dilatation, with hydronephrosis and multiple small stones in the lower pole of the left kidney with a prominent collecting system (Figure 2).
Reformatted images of a non-contrast computed tomography scan of the kidney, ureters and bladder. Coronal image (left) showing a proximal ureteric stone (arrow) causing hydronephrosis. Sagittal image (right) showing a left lower pole intra-renal stone (arrow) with some hydronephrosis
Sulphadiazine was stopped and replaced with clindamycin (600 mg six-hourly); pyrimethamine was continued. With insertion of bilateral percutaneous nephrostomies and increased intravenous fluids, renal function normalized over the next 14 days. Ultrasound imaging on day 45 showed complete resolution of urolithiasis.
HAART (zidovudine/lamivudine and boosted lopinavir) was started 76 days after starting treatment of cerebral toxoplasmosis, once there was sustained improvement in the patient's condition and MRI. Nine months following initial presentation the patient is alive; current CD4 count = 170 cells/μL, viral load = undetectable and renal function remains normal.
DISCUSSION
Before the introduction of HAART, cerebral toxoplasmosis was a common first presentation of HIV infection. 7 Clinicians today are less likely to encounter and manage such opportunistic infections and treatment-associated complications. 5,8–13
Sulphadiazine and its hepatic metabolite acetylsulphadiazine are excreted via the renal tract; they are poorly soluble in urine and may potentially precipitate in the acid environment, producing crystalluria and stones. Crystalluria is common, may occur in up to 28% of patients taking sulphadiazine 3 and is potentially nephrotoxic via both direct chemical irritation of the tubular epithelium and tubular obstruction due to urolithiasis. 2 Dehydration and hypoalbuminaemia are regarded as potential risk factors for development of sulphadiazine crystalluria and stone formation. 13 Sulphadiazine-induced urolithiasis should be suspected if acute renal failure develops in patients receiving this drug, even in the absence of demonstrable crystalluria. The diagnosis is confirmed by demonstration of stones by ultrasound, CT or MRI. 8,10
Outpatient antibiotic therapy is gaining popularity for a variety of medical conditions. 14–16 Given the long duration of acute treatment for toxoplasmosis use of outpatient treatment will be popular with patients and additionally will help to reduce inpatient length of stay. This case serves to remind clinicians who may be unfamiliar with use of sulphadiazine that rapid onset renal failure due to urolithiasis can occur despite good hydration and close monitoring. We suggest that if outpatient treatment of toxoplasmosis is contemplated, careful attention to fluid balance, daily checking of urine for the presence of crystalluria, and frequent monitoring of biochemical renal function (3 times a week) are required in order to avoid this potentially serious complication of treatment.