
Abstract
Summary
The aim of the study was to test for relationships between state-level sex educational policies and sexually transmitted disease (STD) rates. We analysed US case reports of gonorrhoea and chlamydial infection for 2001–2005 against state policies for abstinence coverage in sexuality education, using the proportion of the population per state who identified as black (aged 15–24 years) as a covariate. We also tested for effects on 15–19 year olds versus 35–39 year olds and tuberculosis rates (the latter to ensure findings applied only to STD). States with no mandates for abstinence had the lowest mean rates of infection among the overall population and among adolescents. States with mandates emphasizing abstinence had the highest rates; states with mandates to cover (but not emphasize) abstinence fell in between. Rates in some states covering abstinence changed faster than in others, as reflected in sharper declines (gonorrhoea) or slower increases (chlamydial infection). These effects were not shown for tuberculosis or 35–39 year olds. Having no abstinence education policy has no apparent effect on STD rates for adolescents. For states with elevated rates, policies mandating coverage may be useful, although policies emphasizing abstinence show no benefit.
Keywords
Introduction
Abstinence promotion as public policy has received considerable attention. Section 510 of the 1998 Social Security Act presents the teaching of abstinence from sexual activity outside of marriage as ‘expected standard’ for school-age children and asserts several negative consequences of sex outside marriage, for example, ‘harmful psychological and physical effects’, within the framework of that law. 1 National data, in fact, suggest 83% of men received abstinence education in 2002 (up from 74% in 1995), while instruction about birth control methods decreased for men (from 81% to 66%) and women (from 87% to 70%) over the same time period. 2
A 2007 report outlining results from randomized, controlled trials of four programmes implementing Section 510-based educational programmes showed no differences by exposure to the education, with 49% of participants reporting lifetime abstinence in the intervention and control arms and 55% (intervention) versus 56% (control) reporting abstinence over the previous 12 months. 3 One recent cohort study comparing those receiving comprehensive sexuality education to those receiving none and those receiving abstinence-only education found significant benefits only for those in the first category. 4
Other researchers have had success showing that exposure to abstinence education can delay sexual debut,5,6 albeit not necessarily the negative outcomes of sex. 7 Moreover, delayed debut may not be specific to abstinence education, as similar results have been shown for formal and more comprehensive sex education in general. 8 Researchers have even tested across the domain of possible outcomes for potential deleterious effects of abstinence, with cohort data showing not only the oft-demonstrated link between early sexual debut (compared with peers) and outcomes such as high-risk partners and erectile problems, but also weaker links between erectile problems and late sexual debut. 9
The relationship between the two endpoints of any abstinence promotion health model, based around the reduction of harm, is less closely addressed. Specifically, do abstinence policies (the first step) have any demonstrable impact upon sexually transmitted disease (STD) rates (the harmful outcome)? Thus, testing effects of abstinence promotion policy on STD outcomes is an important public health analysis. The most widely developed abstinence policies for states generally fall within the purview of secondary education. In the current analyses, we focused upon abstinence content in education and operationalized abstinence policy as abstinence education policies by state.
The relevant research question pertains to whether abstinence education policies are associated with reduced STD rates, increased STD rates or not associated at all. The data are observational, and opposing hypotheses for the same outcomes are possible: for example, abstinence education may be associated with high rates because such education is unhelpful to STD prevention or because states with high rates turn to abstinence education. In order to mitigate these issues, we examined effects over time: states with high STD rates may turn to abstinence education as a policy, but, if that policy is effective, STD rates should drop over time. In this paper, we attempt to answer the question: To what extent do STD rates in US states rise or fall over time according to state abstinence education policies?
Methods
Data sources
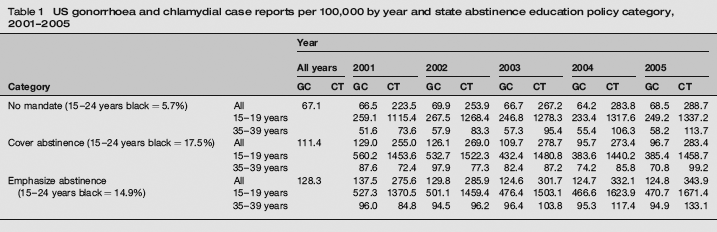
US gonorrhoea and chlamydial case reports per 100,000 by year and state abstinence education policy category, 2001–2005
We had also drawn data on policies toward coverage of contraception in sex education from the Guttmacher reports. No states required an emphasis on contraception, so there were only two levels of this variable. Initial analyses showed that there was no association between policy on contraception and STD rates. Further analyses showed that contraceptive policy (no mandate versus coverage) was evenly distributed across the coverage and emphasis levels of abstinence policy. As contraception policy had neither independent effect on results nor a role as a covariate, we have excluded it from the analyses in this paper.
Analyses
Data were not available from two states, so the framework for analyses comprised 48 states by five years of data for each STD. The principal analysis was a mixed model multivariate analysis of variance with three between-groups levels for policy and five levels of the repeated measure (yearly STD rates). This analysis controls for the non-independence in the repeated measure and yields effects for policy collapsed across year and for year collapsed across policy. The third and most salient result is the effect for the year by policy interaction, which speaks to differential changes in rates across time by group. Each test is represented by F, the ratio of explained to unexplained variance, and an accompanying P value to indicate whether F > 0. Although group sizes were unequal (between 7 and 23 states per group), equality of covariance matrices was maintained, and P values were accurate. 10
Our initial analysis was with the population gonococcal and chlamydial rates in each state. To improve the validity of the model, we added further variables. First, because research into health disparities has repeatedly shown a large disparity by race,11,12 we ran analyses using the percentage of blacks aged 15–24 years in state populations as a covariate. Second, because the effects of education should attenuate with age, we also ran analyses for 15–19 year olds and 35–39 year olds separately. Finally, because tuberculosis (TB) rates are correlated with many STD rates, but should not be affected by abstinence education, we ran analyses with 2001–2005 TB rates as outcomes. These three steps allow for a likely confounding variable to be incorporated and also for model results for the theoretically most affected populations and outcomes to be distinguished from others.
Results
Gonorrhoea rates dropped between 2001 and 2005, and states differed in gonorrhoea rates according to the nature of their abstinence education policies. Specifically, states with no policies mandating abstinence had the lowest mean rates across time (M = 67.1 cases per 100,000) and those which had policies mandating an emphasis upon abstinence had the highest rates (M = 128.3) (Table 1). Gonorrhoea rates across states in each of these two groups changed little between 2001 and 2005. States that had policies mandating abstinence coverage, but not emphasis (M = 111.4), however, saw their rates fall consistently, although not to the level of states without any mandated coverage. Table 2 (model 1) shows that the average rates between 2001 and 2005 differed significantly across the three groups. The interaction term in Table 2 (model 1) and an examination of the means in Table 1 demonstrated that states that had policies mandating only coverage had drops in gonorrhoea rates that were significantly greater than those in the other two groups (Figure 1).
Gonorrhoea rates in states by sexuality education policy, 2001–2005. (a) Ages 15–19 years, (b) All ages Analysis of variance and covariance model tests: gonorrhoea DF, degrees of freedom Note: For main effects: ‘year’ tests whether gonorrhoea rates differ across year, collapsed across category; ‘abstinence category’ tests whether gonorrhoea rates differed by category (‘no mandate’, ‘cover abstinence’ and ‘emphasize abstinence’) collapsed across year; % black tests whether gonorrhoea rates differ according to the proportion of blacks aged 15–24 years in a state. For interactions: category × year tests whether changes in gonorrhoea rates over time differ by abstinence category. % Black × year tests whether the association between % Black and gonorrhoea rates differs across time
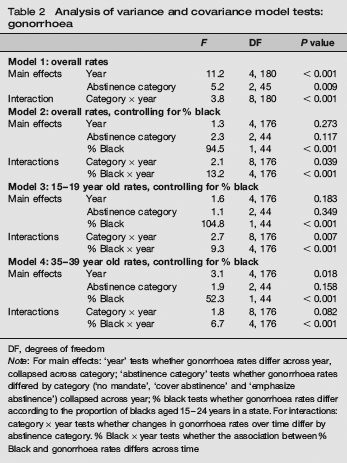
The percentage of the population who were black, aged 15–24 years, differed significantly by category, F(2, 45) = 5.6, P = 0.006. The percentages ranged from 5.7% in states with no mandate at all to 17.5% in states with a mandate to cover abstinence and 14.9% in states with a mandate to emphasize abstinence (Table 1). When controlling for the percentage of the population who were black, aged 15–24 years, we found states with higher percentages of black, aged 15–24 year olds, had higher rates of gonorrhoea, while rates by year and abstinence category were attenuated below significance (Table 2, model 2) (contrast tests show states with no mandate still had lower rates than states emphasizing abstinence). However, the interaction of category and time in model 2 remained statistically significant. These results illustrate the large disparity in gonorrhoea rates by race, but also indicate the diminishing of this disparity in recent years, which is shown by the interaction between year and % black.
With 15–19 year olds as the data source, we found no detectable overall drop in rates between 2001 and 2005 for this age range (Table 2, model 3). The effect of % black remained, with the reduction in the inferred disparity over time also remaining clear via the interaction with year. As with the overall population, rates dropped only in those states mandating, but not emphasizing, coverage (i.e. not detectably in the other two groups). For 35–39 year olds (Table 2, model 4), gonorrhoea rates dropped between 2001 and 2005, with abstinence education policies no longer a significant correlate, neither as a main effect nor as an interaction with year.
For each year, we found that gonorrhoea and TB rates were correlated; between 2001 and 2005, the lowest correlation was r = 0.39 (2002), and the highest was r = 0.48 (2003), both P < 0.01. When we selected TB rates as the outcome variable, we found an effect for time, with TB rates diminishing from 4.33 cases per 100,000 in 2001 to 3.61 cases per 100,000 in 2005, F(4,176) = 7.9, P < 0.001. There was also a main effect for abstinence category, F(2, 44) = 4.5, P < 0.05, but not for the time by category interaction, F(8, 176) = 1.5, NS. The main effect for time is not relevant to the current study, and the effect for abstinence category reflects the correlated gonorrhoea and TB rates. The absence of an interaction effect distinguishes the gonorrhoea model from the TB model.
Chlamydial infection
Analysis of variance and covariance model tests: chlamydial infection

DF, degrees of freedom
Note: For main effects: ‘year’ tests whether chlamydia rates differ across year, collapsed across category; ‘abstinence category’ tests whether chlamydia rates differed by category (‘no mandate’, ‘cover abstinence’ and ‘emphasize abstinence’) collapsed across year; % black tests whether chlamydia rates differ according to the proportion of blacks aged 15–24 in a state. For interactions: category × year tests whether changes in chlamydia rates over time differ by abstinence category. % Black × year tests whether the association between % black and chlamydia rates differs across time
We replicated the above analyses for 15–19 year olds and 35–39 year olds. We found no group differences in rates across year for 15–19 year olds, nor any differences in year across groups (Table 3, model 3). However, there was an interaction between policy and year, with states having mandates to cover abstinence having essentially flat rates, while rates at the other two levels of abstinence policy increased. We also observed a large disparity by race among 15–19 year olds, indicated by the effect for percentage of blacks aged 15–24 years in model 3. As with gonorrhoea, among 25–39 year olds, the interaction for abstinence education category by year was not statistically significant (Table 3, model 4).
Discussion
We found that states with no mandate had the lowest rates of both STDs, while states that emphasized abstinence had the highest. In both categories, gonorrhoea rates were quite stable, while chlamydial rates rose. Although states that had a mandate to cover abstinence had higher rates than states with no mandate at all, coverage was also associated with (a) declining rates of gonorrhoea over time and (b) slower increases in chlamydial infection. This year by category effect was retained for adolescents, but not adults; for STD, but not TB; and while controlling for a major racial disparity.
Once again the racial disparities in gonorrhoea and chlamydial infection are evident, although results suggest these disparities are declining. However, adolescent gonorrhoea case reports do not appear to be declining overall, while adolescent chlamydial case reports are increasing. As for what abstinence education policies do to affect those rates, as we suggested in the introduction, states with low rates may have seen little need to mandate abstinence education.
Looking at states with relatively elevated rates (as per the 2001 means shown in Table 1), the next step for research is to look more closely at how policy is enacted in various states. Ideally, one would examine all 50 states, but, if constrained, a comparison of the seven states in which declines were seen against a selection of states in which abstinence was emphasized, but no declines were seen, would be useful. Such a study would be a policy-level analogue of an epidemiological case-control study with a view to identifying more precisely which variables in policies may actually influence STD rates, and possibly prospective comparative effectiveness studies to follow.
Until such data are collected, we can only generate hypotheses. It may be that emphasis is correlated with the amount of time spent on discussing it in curricula. If so, the solution may simply require teachers to spend less time on the tactic: some time helps reduce rates, lots of time does not. Alternatively, abstinence emphasis may be correlated with content designed to arouse fear, while coverage without emphasis is correlated with presentation as a ‘reasonable choice’ or as a ‘suitable option.’ If so, we have yet more evidence that resorting to fear arousal is generally ineffective. Experimental evidence to this point in health intervention dates back at least several decades,13,14 but many parents, physicians and school boards remain unconvinced. Perhaps a less fear-inducing approach permits students to think through the strategy more clearly. We can say that coverage versus emphasis is not a marker for abstinence-only versus abstinence plus other options: approximately half the states had a contraception policy in each of the coverage and emphasis groups.
Our study has limitations. First, there are constraints on interpretation inherent in ecological data; second, there may be some disruption between state policy and actual educational practice at the school district (or similar) level. With ecological analyses, we cannot show that those who were infected with gonorrhoea were more or less likely to be exposed to whatever sex education exists in each state. Moreover, in many states, local districts exercise control over educational policies; therefore, state mandates may or may not be closely reflected in classrooms. 15 In fact, recent data show states vary widely in the proportion of schools in which HIV prevention topics are taught (36–99%). 16 However, these limitations bias data toward the null, and our results exist in spite of any such bias, not due to it. In sum, although not experimentally generated, our findings discriminate among groups in a logical manner, and the findings have substantial construct validity. 17
In conclusion, our analysis of the relationship between abstinence education policy and STD rates at the state level suggests that lack of any abstinence education policy has no apparent harmful effect on STD rates among United States adolescents. In states with elevated STD rates, policies mandating coverage of abstinence among other approaches may have a beneficial impact on STD rates. Conversely, there is no evidence of a beneficial effect resulting from policies that emphasize abstinence. Future research should focus on the content of different abstinence policies, how they are operationalized into programmes and comparative effectiveness studies of alternating sex education policies and other programme-relevant questions.
Footnotes
Acknowledgements
The authors wish to thank Ms Rachel Gold for her assistance locating classifications of state educational policies and Ms Bridget Wynn for her logistical assistance with this paper.