
Abstract
Partner notification is essential for the control of chlamydia infection, which is on the rise. The aim of this study was to assess the performance of partner notification for chlamydia infection in the genitourinary medicine clinic at the University Hospital of Hartlepool, UK from 2004 to 2008. Overall 1.37 partners were declared per index patient, with male patients declaring 1.59 partners and female patients declaring 1.19 partners. For each chlamydia index patient 0.52 partners were screened (38 per cent of declared partners). Fifty-seven percent of the screened patients were positive for chlamydia and this increased from 33% in 2004 to 66% in 2008. The number of index cases needed to interview to get a new positive chlamydia was 3.37 over the study period and varied from 6.74 in 2004 to 2.74 in 2008. This audit highlights the need to improve partner notification for chlamydia infection.
INTRODUCTION
Partner notification is a process whereby the sexual partners of people with a diagnosis of sexually transmitted infections (STIs) are informed of their exposure to infection. Partner notification can be either patient referral (where the service user informs their sexual partner(s) of the need for testing and treatment) or provider referral (in which the service provider contacts sexual partner(s) on behalf of the service user, to advise on the need for testing and treatment). 1
Chlamydia is recognized as the most prevalent treatable STI in the United Kingdom, 2 with approximately 70% of individuals being either asymptomatic or experiencing transient symptoms. The past 10 years have seen a dramatic increase of nearly 112% in rates of infection. 3 Infected individuals having unprotected sexual intercourse with new partners is thought to be a major contributing factor to this rising trend in infections. An important tool in the prevention of chlamydia infection and transmission is partner notification. However, there are difficulties associated with contacting and treating sexual partners of chlamydia index patients. The Society of Sexual Health Advisers (SSHA) and The British Association of Sexual Health and HIV (BASHH) offer National Guidelines and advice on partner notification and management. 1,2
AIMS
The aim of this study was to evaluate the performance of partner notification against auditable outcomes set by National Guidelines. According to targets set by the SSHA, for each index case of chlamydia, at least 0.6 sexual partners outside London and 0.5 sexual partners in London should attend for screening and treatment within 90 days of the health adviser's first interview. 1 BASHH guidelines have stated 0.43 contacts per index case for larger city clinics or 0.64 contacts per index case for other clinics. 2 A review article has proposed that 0.6 sexual contacts for each index patient with chlamydia should be screened. 4 BASHH furthermore recommends notification of all sexual partners of symptomatic patients over a four-week period prior to onset of symptoms, and for asymptomatic patients notification of all partners over the previous six months or the most recent sexual partner if outside this period. 2
METHOD
This was a retrospective analysis of chlamydia infection information obtained from the Lillie database system of the genitourinary medicine clinic at the University Hospital of Hartlepool, UK. Each patient's sexual orientation, contacts declared, contacts seen and contacts diagnosed with chlamydia were recorded. The health adviser carried out partner notification when details of sexual partners were available.
The health adviser noted the number of partners declared by the patient, the number of partners in the previous three months, the number of partners in the past 12 months and condom use. The index patient discussed sexual partner(s) in as much detail as possible with the health adviser. The health adviser entered details of partner's full name, address, telephone number and date of birth in the patients' notes. The index patients were given the option of patient referral or provider referral. 1 Partner notification was considered complete when named partners had attended for screening and treatment. The data were analysed for the number of partners seen per index patient as per the National Guidelines. 1,2
RESULTS
A total of 1045 index patients (469 men and 576 women) declared 1434 sexual partners (747 men and 687 women) and 545 (38%) of declared partners attended for screening and treatment. The number of partners declared per index patient was 1.37. When analysed by sex, this number was 1.59 for male and 1.19 for female index patients. The number of partners seen per index patient was 0.52. Of the 545 partners evaluated, 308 (57%) tested positive for chlamydia and this increased from 33% in 2004 to 66% in 2008 (Table 1 and Figure 1). The number of positives per index patient is reported as the number of index cases needed to interview (NNTI) to get a new positive. The NNTI was calculated by using the formula: number of index patients/(number of screened partners × proportion of screened tested positive). The NNTI statistic for 2004 = 109/(49 × 0.33) = 6.74. This was 3.37 over the study period and varied from 6.74 in 2004 to 2.74 in 2008 (Table 1).
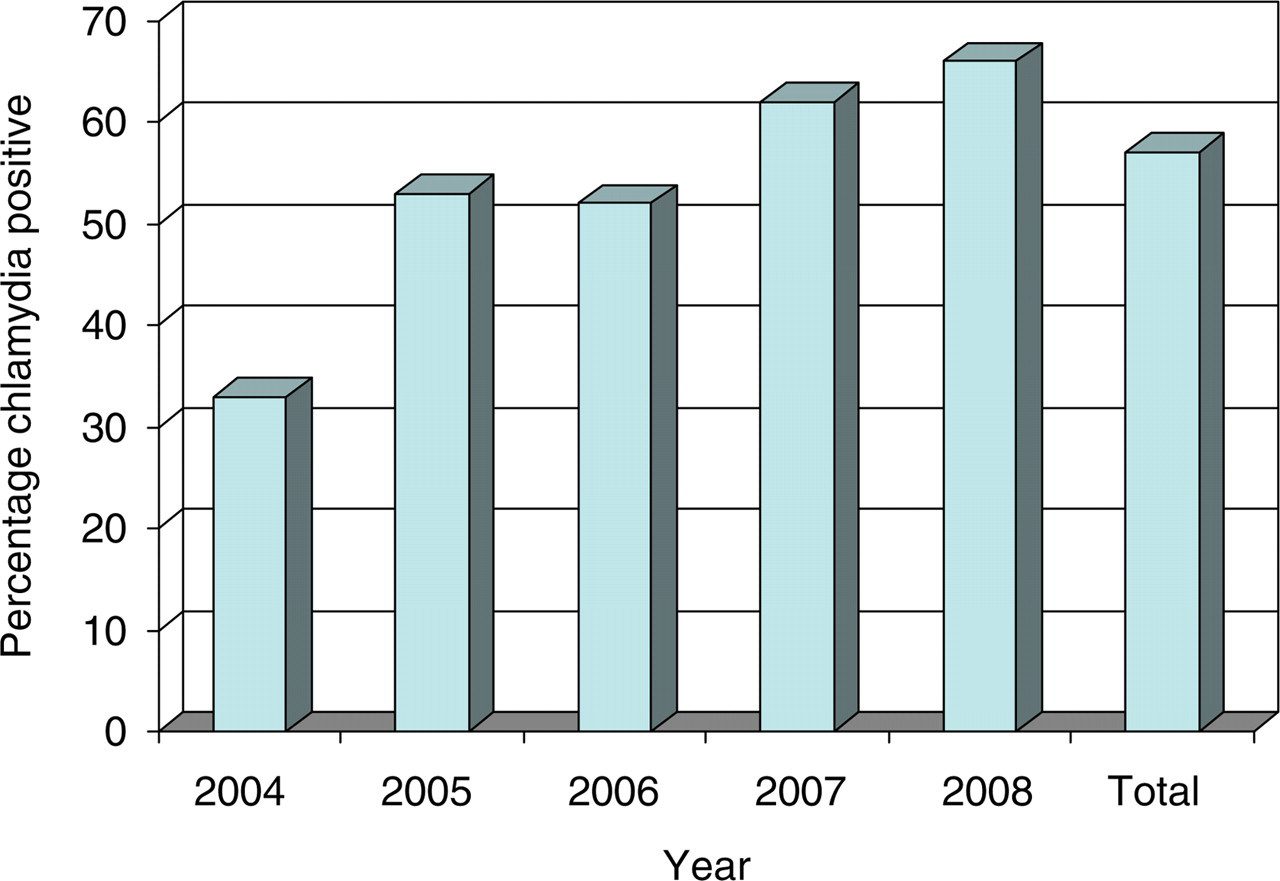
Proportion of named contacts screened that tested positive for chlamydia by year of diagnosis
Numbers of patients declared and seen per positive chlamydia index case
NNTI = number of index cases needed to interview
*Target: 0.5–0.6 partners for each index patient should be screened
The number of men who have sex with men (MSM) was 17 (3.2%) of the index male patients (Table 2). There were no lesbians identified in the index female patients.
Analysis by sexual orientation of male patients of numbers of patients declared and seen per positive chlamydia index case
NNTI = number of index cases needed to interview; hetero = heterosexual male patient; MSM = men who have sex with men
*Target: 0.5–0.6 partners for each index patient should be screened
DISCUSSION
The number of sexual partners who attended per index patient was 0.52 over the five-year period – this is lower than the national target. This may be due to some partners being identified as having attended alternative locations for screening and treatment. This audit has highlighted an important issue in the management of partner notification in compliance with the national protocol. The national target for partner notification of 0.6 per index case outside London may not be achievable because of multiple casual sexual partners. 5
Notifying sexual partners of their potential exposure to STIs has been a mainstay of disease control and prevention since 1943. 6 In today's climate, partner notification would appear to be a simple task; new and innovative means of communication such as text messages, voicemail and Internet messaging should enable individuals to notify known contacts quickly. 7
Interestingly, the data demonstrate that despite increasing numbers of index patients since 2004, the NNTI to identify a new chlamydia case has decreased from 6.74 in 2004 to 2.74 in 2008. This trend may be due to increasing prevalence of chlamydia infection in the population. The number of index MSM has remained low over the study period and therefore has no impact on the NNTI trend in the present audit. Although the audit produced figures comparable with the National Guidelines, we still found 62% of partners who remained inaccessible and potentially infected. Perhaps the greatest challenge posed is detecting those individuals who are infected asymptomatically and who unknowingly transmit infection through unprotected sex. These individuals may also develop complications of their infection. Currently, there is a growing public health concern over the rising numbers of STIs and this underpins the importance of effective partner notification and management of index patients. However, it should be noted that some inaccessible sexual partners may have attended other local health services for chlamydia screening and treatment. Although this information was not available for analysis in our data, attempts to verify this attendance is recommended because index patients' reports may be unreliable. 8
Online notification may be an effective strategy to increase partner notification and a number of index patients and partners have preferred this method. 9 However, a new Australian study reported some quite hostile responses to text messages as a method of notification. 10 The study further highlighted that email and short message service might be appropriate and useful in some circumstances. Therefore, availability of tailored resources may assist in improving partner notification for chlamydia. 11 Improvement in partner notification may require increased resources for health advisers and better communication between clinics for verification of attendance of sexual partners. 12 The relative success achieved in managing chlamydia infection based on National Guidelines should be complimented by public awareness campaigns, education and empowerment of patients if we are to achieve higher targets of partner notification.