
Abstract

Sirs: Five percent imiquimod cream is a topically active immunomodulatory agent proven to be effective in the treatment of genital warts, but rarely used to treat cervical condylomata acuminata (CA). Here we report five women aged 21–40 years suffering from recurrent and refractory cervical CA. They had received previous treatment of CO2 laser or electrocautery 2–4 times during the past 1–6 months. After physical examination and the acetic acid test, we found pale or pink plaques on the cervix uteri, which were grossly cauliflower-like or asperous, and acetowhitening lesions. We diagnosed these patients clinically as having recurrent CA on the cervix uteri. After the patients signed informed consents in the first visit, a piece of the lesion was clamped out for biopsy, and then high-frequency electrocautery therapy was given (Figure 1a and b). As soon as the ulcers healed one to two weeks later, and we had made sure of the diagnosis of cervical CA by the biopsy and immunochemical staining for human papillomavirus antigen (HPV-Ag), we applied 5% imiquimod cream to the cervix uteri (Figure 1c). Firstly, we wiped out cervical secretions by cotton balls in order to bring the cream into enough contact with the cervix uteri and also to avoid dilution of the cream with the secretions. Then we applied 250 mg imiquimod cream on the cervix uteri and kept the patients lying for 10 minutes. Finally, the patients were instructed to wash off the cream after 6–8 hours by vaginal douche to avoid excessive exposure. One week later, the patients returned for the next treatment and the entire course consisted of 12 applications. During the course of treatment, we asked the patients to maintain sexual abstinence and delay the treatment until after menstruation. All patients remained wart free in the 6–9 months follow-up period (Figure 1d). Furthermore, we found that the cervicitis of three patients was cured, and the mucous membranes of all the patients were smooth and elastic. Our patients had mild and endurable local adverse reactions. In the second week, one patient was noted to have moderate cervical erosion; hence we delayed the treatment until the next week. Two patients had mild erosions and the other two only had cervical hyperaemia, but these patients all decided to continue the treatment and went on to complete the entire course.
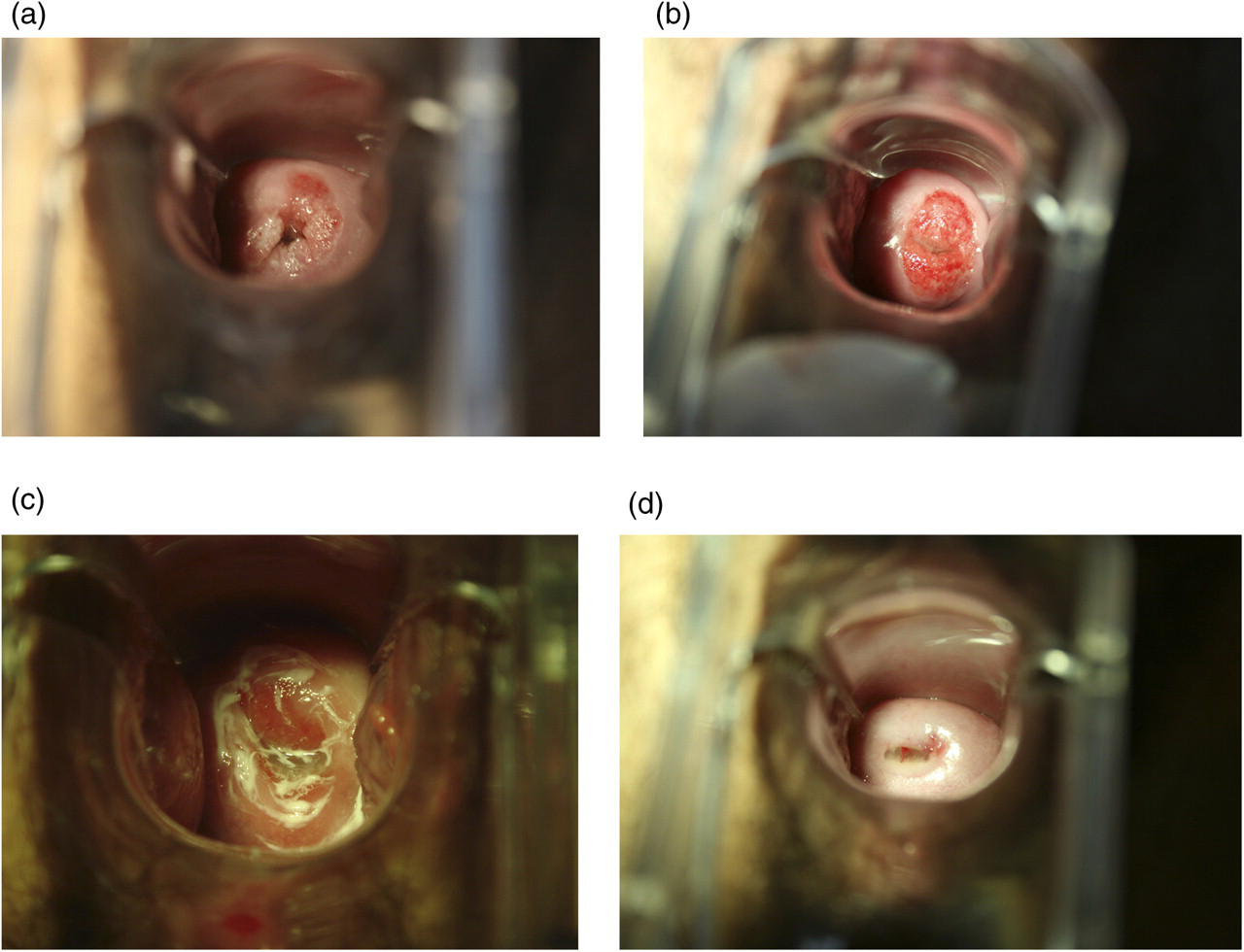
(a) In the first visit, there was a pink plaque on the cervix uteri. (b) The lesion healed after high-frequency electrocautery, before application of 5% imiquimod cream. (c) Application of 5% imiquimod cream. (d) In the return visit six months later, the cervix uteri seemed smooth and elastic
Most current therapies depend on physical destruction of the lesions rather than direct antiviral activity against the causative agent, HPV. Imiquimod, an immune-response modifying agent, can indirectly activate cytokines to eradicate the lesions. 1 Although there is no licence for use against CA on cervix uteri, data suggest 5% imiquimod cream as an effective therapy against cervical intraepithelial neoplasia. 2 Perhaps the cytokines and sexual abstinence contributed to the unexpected smooth and elastic cervix uteri.
As a treatment for genital warts that is specifically antiviral and non-destructive, imiquimod could offer a significant advantage over current treatment modalities for HPV-related disease. Thus we think 5% imiquimod cream may be a potential therapy for treating and preventing the recurrence of cervical CA.