
Abstract
The aim of this study was to assess prevalence and risk factors for sexually transmitted infections (STIs) among fishermen along Lake Victoria, Kenya. This cross-sectional study surveyed 250 fishermen from beaches in Kisumu District using proportional-to-size sampling based on the number of registered boats per beach. Participants provided demographic and sexual behaviour information, blood for HIV-1 herpes simplex virus type 2 (HSV-2) and syphilis serological tests urine for transcription-mediated amplification assays for Neisseria gonorrhoeae and Chlamydia trachomatis and penile and scrotal swabs for human papillomavirus (HPV) DNA assay. Consistent condom use with the three most recent sexual partners was reported by 30%; 38% reported concurrent sexual partnerships and 65% reported ever having transactional sex. HIV seroprevalence was 26%, HSV-2 seroprevalence by Western blot assay was 58% and 9.5% were rapid plasma reagin and Treponema pallidum particle agglutination assay positive. Genital HPV DNA of any type was detected in 57.2% with 74% of these having two or more HPV types. C. trachomatis and N. gonorrhoeae were detected in 3.2% and 1.2% respectively. Risk factors for syphilis seropositivity included working on multiple beaches during the past year (adjusted odds ratio [AOR] 3.81; 95% confidence interval [CI] 1.29–11.28). HPV infection was associated with owning a radio which is a marker for higher socioeconomic status (AOR 6.33; 95% CI 2.94–7.14) and reporting transactional sex with the most recent sexual partner (AOR 3.03; 95% CI 1.23–7.69). In conclusion, 90% of fishermen had evidence of one or more STIs. This exceptionally high-risk occupational group represents a high priority for preventive interventions.
INTRODUCTION
The prevalence of sexually transmitted infections (STIs), including HIV infection, has been high among mobile occupation groups such as truck drivers, migrant workers and fishermen including those in East Africa 1–6 and elsewhere. 7–9 The gendered dynamics of fishing communities in contexts of poverty bring together several key contextual factors such as gender inequality, poverty, migratory processes and highly differentiated occupational sex segregation that shape HIV/AIDS risks. 10
Fishing communities, which include both fishermen and others who process or trade in fish, are among the groups with highest HIV/STI prevalence. 11–14 Their vulnerability stems in part from the specific dynamics of the occupation and social interactions that arise out of the fishing industry. 15 The fishing communities attract young, highly migratory men who spend long periods away from their families and local communities so that the social structures and hierarchies that guide sexual norms are not maintained. 16 On the fishing beaches, social ties are based on economic relationships and occupational peer group interactions, providing unrestricted opportunities to determine sexual and behavioural norms. 13
The fishing industry in Kenya and specifically in Kisumu District where data for this study were collected plays an important role in the national and regional economy. For instance, the industry contributed 0.5% to gross domestic product (GDP) in the year 2006 with Lake Victoria contributing over 90% of the total nominal fish production annually. 17 The district is largely occupied by people of Luo ethnicity who traditionally do not practice male circumcision. HIV seroprevalence in the general population is 15.4% compared with the Kenyan national average of 7.4%. 18,19 Kisumu, the capital of Kisumu District and Nyanza Province, is the leading commercial, trading, industrial, communication and administrative centre in the Lake Victoria basin. It has an estimated population of 0.5 million people with 53% living below the poverty line (on less than 1 US$ per person per day). 20 The highly migratory fishermen, who are key players in this important industry in the district, are thought to engage in high-risk sexual behaviour that predispose them to the risk for acquiring and transmitting STIs, including HIV. This cross-sectional survey sought to provide a comprehensive assessment of sexual risk behaviours and related STIs among fishermen along Lake Victoria in Kisumu District, Kenya.
METHODS
Design and study population
We conducted a cross-sectional survey along Lake Victoria, Kenya between August and December 2005, recruiting fishermen from fishing boats selected from 18 of the 32 beaches in the Kisumu District, using a proportional-to-size sampling method based on the number of registered boats per beach.
For each beach, we prepared a primary and a secondary list of boats, randomly selected from the registered boats at these beaches. The participants were mainly selected from boats on the primary list. We only selected participants from boats in the secondary list if: a boat on the primary list was no longer in operation; a boat on the primary list had less than four crew members; or, when potential participants selected from boats on the primary list declined to participate or failed to meet inclusion criteria. The list of registered boats we used was so current that only 4.8% (3/63) of the boats on our sample list were not in operation at the time of data collection. For boats that had less than four crew or those from which some of the crew declined to participate or did not meet the inclusion criteria, we went ahead and recruited all the crew who consented for participation and met the inclusion criteria, the balance (4 − X) were recruited from the next boat on secondary list. For boats with more than four fishermen, we selected the first four available crew members, and continued sequentially down the list of boats until we reached our sample size of 250 fishermen.
We had regular meetings with fishermen during their weekly assemblies and during our study mobilization campaigns where we interacted with their fishermen, sometimes in question and answer sessions, to inform the fishermen about the study and gain their confidence in us. Further, when the selected fishermen came to be recruited into the study, the study staff and, particularly, the social scientist who conducted the face-to-face interviews, prioritized making the fishermen comfortable and creating a rapport and a sense of mutual trust. All the interviews happened in the morning when the fishermen were sober to enhance recall. For fishermen who were not sober at the time they came to be recruited, they were asked to come the following day when sober. This study was approved for implementation by both Kenya Medical Research Institute/National Ethical Review Committee and University of Washington Human Subjects Review Committee.
Measurements
Survey questionnaire and specimen collection
Participants provided written informed consent and underwent a standardized structured interview conducted in private by a social scientist who gathered socioeconomic and demographic details (covering age, religion, marital status, income and material assets, number of children and education), and information on each of the last three sexual partnerships with respect to condom use, concurrent relationships, extramarital sex and transactional sex, i.e. exchange of gifts including fish for sex. We provided pre- and post-test counselling for HIV and obtained blood samples for serological testing for infection with HIV, herpes simplex virus type 2 (HSV-2) and syphilis; urine for Neisseria gonorrhoeae and Chlamydia trachomatis testing; and penile and scrotal specimens collected with saline-wetted swabs for detection of human papillomavirus (HPV) DNA. Appropriate treatment and/or referral were given for those diagnosed with HIV, gonococcal or chlamydial infection or syphilis seropositivity.
Laboratory assays
Serum was divided for three sets of tests: HIV-1 serology was carried out according to Kenyan Ministry of Health guidelines, first using Determine HIV-1/2 (Abbott Laboratories, Abbott Park, IL, USA) and Uni-Gold™ HIV (Trinity Biotech PLC, Bray, Ireland), using the p24 ELISA Vironostika kit, (Organo Technika, Boxtel, Oss, The Netherlands) to resolve any discrepancies between the first two assays. Syphilis serological testing employed the Macro-Vue Rapid Plasma Reagin test (Benex Limited, Shannon, Ireland) confirmed by Treponema pallidum particle agglutination (TPPA). HSV-2 serological testing first employed the HerpeSelect HSV-2 ELISA (Focus Diagnostics, Cypress, CA, USA), defining an optical density index value of >1.1 as positive, with positive results then confirmed at the University of Washington by Western blot assays 21 as described elsewhere. 22 C. trachomatis and N. gonorrhoeae testing employed the APTIMA Combo 2 assay (Gen-Probe Inc, San Diego, CA, USA). HPV DNA was detected first by polymerase chain reaction amplification using HPV L1 consensus primers MY09/MY11/HMB01 and β-globin primers PC04/GH20, followed by dot blot hybridization with generic HPV and β-globin probes. 23,24 All assay procedures and interpretations of results followed the manufacturers' instructions.
Data analysis
Data were collected on Teleform-created case report forms and scanned into the Teleform software (Cardiff™, Vista, San Diego, CA, USA) before exporting into SPSS (Version 15.0; SPSS Inc, Chicago, IL, USA). Depending on the type of variable, appropriate descriptive statistics, including means and standard deviation for normally distributed continuous variables and frequency counts and relative frequencies for categorical factors, were computed. To assess the association between various STIs and other variables, we fitted a logistic regression model for the odds of disease. Given the observational nature of the study, multivariate logistic models were fitted to control for potential confounders and other variables that may not be balanced between groups. As a measure of association, odds ratios (ORs) from the logistic models along with their confidence intervals (CIs) are reported.
RESULTS
Socioeconomic and demographic characteristics
The 250 participants had median age 27 years (range 18–65 years); 73% had at least eight years of basic education, and 70% were married, of whom 14% were polygamous; 24% lived in a house with single room. All were from the Luo ethnic group and 11% had been circumcised. Fishing was the main source of income for almost all (97%) participants. The main occupation for the other three percent was either fish trading or boat making/repairing. Their median monthly income was Kshs. 5500 (80 US$) (Table 1).
Demographic characteristics and sexual behaviours among 250 fishermen on the beaches of Lake Victoria, Kisumu, Kenya
HSV = herpes simplex virus; HPV = human papillomavirus; STI = sexually transmitted infection
*n (denominator) is a subset of the total n, i.e. those staying at their ancestral home
Sexual behaviours
Only 30% of fishermen reported always using condoms with their three most recent sex partners (Table 1). Of 174 who were married, 170 (98%) had extramarital partners and 25% of these consistently used condoms with all of their three most recent sexual partners; consistent condom use with all three most recent partners was reported by 26% of fishermen who suspected their partners to be involved in romantic relationships with other fishermen and 27% who suspected their partners to have an STI. Of 100 fishermen who provided dates of sexual intercourse, 38% reported concurrent (temporally overlapping) sexual partnerships, with 15% having more than one concurrent sex partner. Of those reporting concurrent partnerships, fewer than one-fifth (18%) used condoms with all of their three most recent sex partners. About 88% of the fishermen's most recent sexual partners were wives while only 20% and 5% of their second most recent and third most recent sexual partnerships were with their wives, respectively.
Two-thirds of the fishermen were involved in transactional sex and 14% reported transactional sex with all of their three most recent sexual partners. This involved not only exchange of money for sex (62% of fishermen) but also allowing women to buy fish from their catch and the provision of shoes and clothes (38%). Of 175 fishermen involved in transactional sex, only 28% used condoms with all of their three most recent sex partners (Table 1).
Prevalence of STI infection
Of the 250 fishermen, 26% were HIV seropositive, 58% were HSV-2 seropositive by Western blot and 9.5% were rapid plasma reagin seropositive, confirmed by TPPA. Genital HPV infection was detected in 57%. These included the following oncogenic HPV types: HPV-16 (12%), HPV-35 and HPV-52 (10%), and HPV-18 (7%); as well as non-oncogenic types HPV-62 (11%), HPV-6 (10%) and HPV-70 (8%). C. trachomatis and N. gonorrhoeae were detected in 3.2% and 1.2%, respectively (Table 1). Overall, 90% of the 250 men had serological or nucleic acid amplification test evidence of one or more of these STIs.
Risk factors for STI infections
In univariate analysis, being young (18–24 years old) (OR 0.37; 95% CI 0.18–0.73), single (OR 0.27; 95% CI 0.14–0.50) and with no children (OR 0.27; 95% CI 0.15–0.50) were associated with lower risk of HSV-2. For HIV, having no children (OR 0.42; 95% CI 0.21–0.84) and having an ongoing sexual relationship with the third most recent sexual partner (OR 0.28; 95% CI 0.08–0.97) were associated with lower risk. Only factors that were significant at univariate level were included in the multivariate analysis and when this was done, none of the factors associated with HSV-2 and HIV at univariate level remained significantly associated with lower risk of infection in multivariate analysis. The risk factors significantly associated with each of the STIs tested at univariate level are summarized in Table 2. However, we excluded from the table factors such as education, income, type of house, owning a television, owning a phone, engaging in multiple concurrent partnerships, condom and self-perceived HIV as these were not significantly associated with any of the STIs tested.
Risk factors for sexually transmitted infections by univariate logistic regression analysis
HSV = herpes simplex virus; HPV = human papillomavirus; OR = odds ratio; CI = confidence interval
*Only factors significantly associated with any of the STIs tested are listed in this table. Figures that were not significant have been excluded
†Variable is significantly associated with odds of disease
As shown in Table 3, risk factors for syphilis seropositivity at multivariate level included working on more than one beach during the year preceding the study (adjusted odds ratio [AOR] 3.81; 95% CI 1.29–11.28), while suspecting the second most recent sexual partner of having sexual relationships with other fishermen was protective (AOR 0.35; 95% CI 0.12–0.99). Genital HPV infection was associated with radio ownership (a sign of higher socioeconomic status) (AOR 6.33; 95% CI 2.94–7.14) and having transactional sex with the most recent sexual partner (AOR 3.03; 95% CI 1.23–7.69). Catholics or Protestants were more likely to be infected with HPV than those who were members of independent evangelical churches or other religious denominations (AOR 2.10; 95% CI 1.08–4.07). As shown in Figure 1, seroprevalence of HSV-2 increased with age; seroprevalences of HIV infection and syphilis increased with age until the ages 31–40 years, whereby it then fell. Prevalences of gonorrhoea or chlamydial infection fell with increasing age.
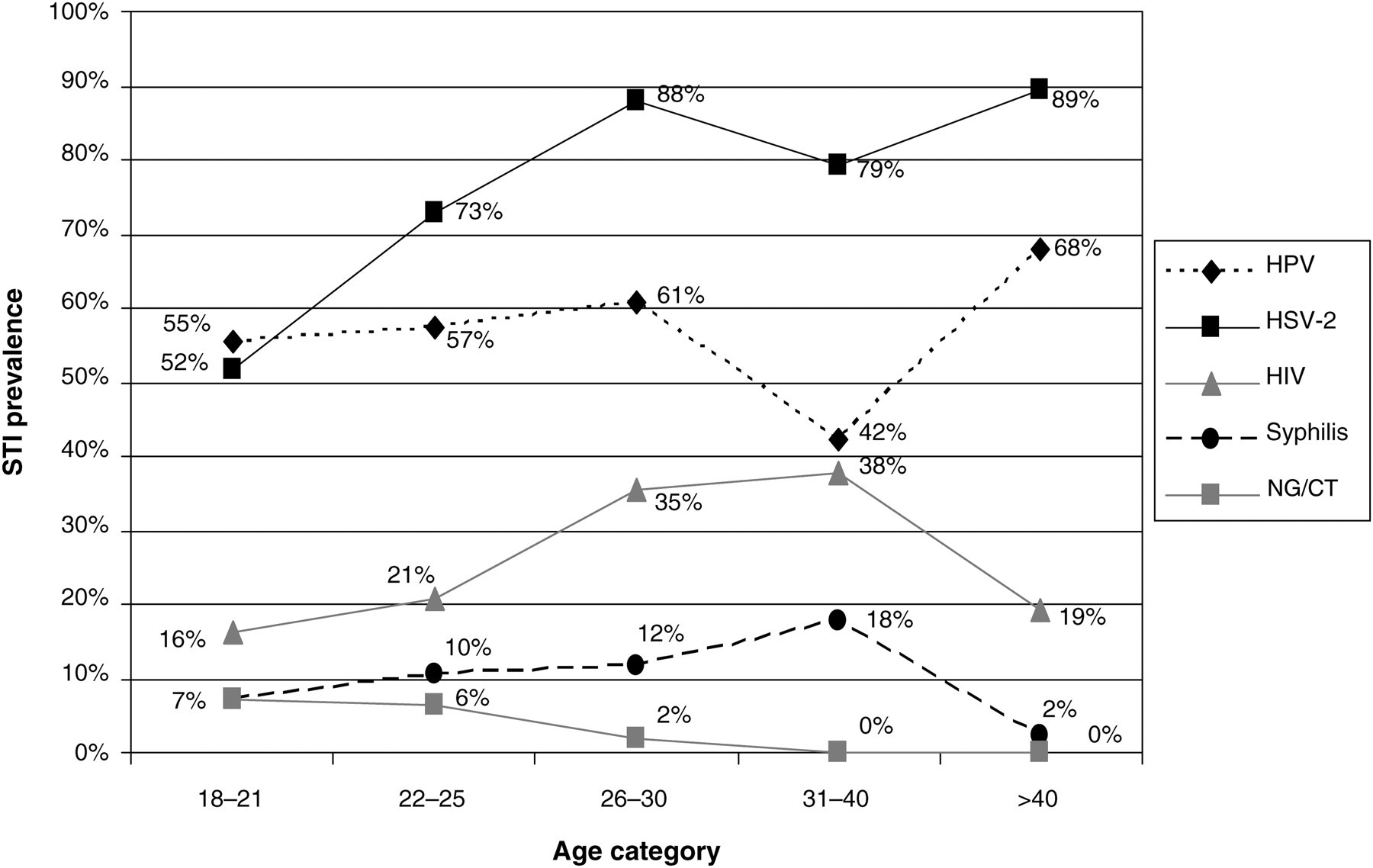
STI prevalence by age group. STI = sexually transmitted infection; HSV = herpes simplex virus; HPV = human papilloma virus; NG = Neisseria gonorrhoeae; CT = Chlamydia trachomatis
Risk factors for HPV and syphilis infections by multivariate logistic regression analysis
AOR = adjusted odds ratio; CI = confidence interval; HPV = human papilloma virus
Non-significant figures omitted
DISCUSSION
This survey examined sexual risk behaviours, prevalence of STIs and the risk factors associated with STI infections among fishermen along Lake Victoria in Kisumu. High-risk sexual behaviours were frequent and prevalences of STIs were exceptionally high in this population. Risk factors for various STIs tested are not well defined in this population with high STI/HIV prevalences.
The fishermen in this community reported high-risk sexual behaviours similar to those observed among fishermen in other settings. 25–28 Individuals involved in unprotected extramarital and concurrent sexual partnerships act as efficient bridges for carrying STIs across different sexual networks with huge public health impact. Our findings support the call by Kissling et al. 29 to include fishing communities among the high-risk subgroups, who, like migrant workers and truck drivers, need to be targeted for special attention and treatment with an endpoint of disrupting the otherwise efficient bridge for carrying STIs across networks.
The HIV and HSV-2 prevalence rates found in this study are among the highest reported in men in Kenya with HIV almost double the prevalence rate of 15.4% 19,30 in the general population and more than double the HSV-2 prevalence more than double the rate of 28% 31 seen in uncircumcised youth in Kisumu. These large differences in prevalences between our study and the aforementioned studies may be partially explained by differences in sampling methods and the age of participants across the studies, with the Mattson and Mehta samples restricted to young men aged 18–24 years, compared with men aged 18–65 years in our study. However, this comparison also underscores the heightened risk of infection among the mobile occupational group of fishermen, as observed in other regions of the world. In a subsequent study of 168 Lake Victoria fishermen screened for a phase I trial of 62% ethanol in emollient gel, we found a 24.5% (41/167) prevalence of HIV infection (Bukusi Elizabeth, 2009, personal communication), suggesting that this pretrial survey was representative of those who were later screened and enrolled in the trial.
The STI/HIV epidemic in the beaches along Lake Victoria in Kisumu District seems to be driven largely by the high demand for fish. Fish-centred sex similar to this documented among fishermen in Kisumu has been reported in many other fishing communities around the world. 29 This practice is attributed to gender segregation of fishing activities, with men largely involved in fish-catching with the women's role as agents for the fishermen and fish consumers. Desperation due to economic hardships make women vulnerable to the fishermen's demands in order to access fish as also reported in the Kafue Flats in Zambia. 26 Structural interventions such as those which help women economically could help women to reduce their HIV/AIDS risks. 32–34 While the economic reasons for the fishmongers' involvement in high-risk sexual behaviours are understandable, the reasons for fishermen's risky choices are not clear. Seeley and Allison 16 postulated a link between working in potentially dangerous occupations such as mining and fishing and social risk-taking behaviour to explain fishermen's risky sexual choices.
Limitations of this study include the use of face-to-face interviews for assessing some sensitive issues that may be subject to social desirability bias. Asking questions about past behaviours may also be subject to recall bias. Data on sexual behaviours with the last three sex partners would be most relevant for associations with recently acquired STIs such as HPV, gonococcal and chlamydial infection in this study, but since the timing of acquisition of HIV, HSV-2 and syphilis seropositivity is uncertain, recent behaviours can best be viewed as potential surrogates of past behaviours. The cross-sectional nature of our survey allows us to infer but not establish causal relationships. Although boats were randomly chosen, individual participants within boats having more than four crew members were selected consecutively as they volunteered, potentially introducing selection bias. Despite these limitations, this study contributes immensely to the understanding STI prevalence rates and associated factors among this occupational group. In conclusion, we can say that the high-risk sexual behaviour and high STI prevalences indicate that fishermen on the beaches along Lake Victoria represent an occupational group at exceptionally high risk for STIs and therefore a high priority for preventive interventions, including circumcision and other preventive modalities. 35
Footnotes
ACKNOWLEDGEMENTS
We acknowledge the Director, Kenya Medical Research (Nairobi) and the Director, Center for Microbiology Research (Nairobi); Beach Management Units; participating fishermen; all the staff of the University of Washington Center for AIDS and STD, particularly Tammy Wilson; staff of the Fishermen Study, the Couple's Intervention Study and the Family AIDS Care and Educational Services in Kisumu, Kenya; the STI laboratory in Kisumu, Kenya; and the University of Washington Virology Laboratory in Seattle, USA. The study was funded by NIH Grant No. U19-AI031448-16.