
Abstract
Although vaccination with Bacille Calmette-Guérin (BCG) is considered safe, adverse regional (BCG-itis) and disseminated (BCG-osis) diseases preferentially occur in the immunocompromised host. The infection with human immunodeficiency virus (HIV) by mother-to-child transmission leads to impaired cellular immune responses, a situation that poses a great challenge regarding the universal use of BCG vaccine. World Health Organization recommends that children who are known to be HIV-infected, even if asymptomatic, should no longer be immunized with BCG. Many of the complications of BCG vaccination occur in severely immunosuppressed HIV-infected children and are related to late institution of antiretroviral and antimycobacterial therapy. We report two cases of BCG-itis in HIV-infected infants, who fulfilled clinical criteria of immune reconstitution inflammatory syndrome: axillary adenitis, one with suppuration, and both temporally associated with precocious restoration of immunity elicited by the use of antiretroviral therapy. Isoniazid (10 mg/kg/day) was offered until regression of adenopathies, and lesions were not handled.
INTRODUCTION
Bacille Calmette-Guérin (BCG) vaccination is considered safe. However, a worrisome risk scenario has emerged from various reports of BCG-related disease, particularly BCG-osis, in HIV-infected children. 1 Despite difficulties in comparing the relevant studies, mainly due to the differences in methodologies used and the frequent lack of characterization of Mycobacterium bovis, the World Health Organization (WHO) recommends that children who are known to be HIV-infected, even if asymptomatic, should no longer be immunized with BCG. 2
Professionals working with HIV-infected infants confront BCG adverse events related to severe immunosuppression or to immune dysfunction elicited by introduction of highly active antiretroviral therapy (HAART). Many of the complications of BCG vaccine occur in severely immunosuppressed HIV-infected children and are related to late institution of antiretroviral and antimycobacterial therapies. 3 BCG adverse events may also be outcomes of immune reconstitution inflammatory syndrome (IRIS) following HAART. IRIS is an immunopathological condition known to cause disease, 4,5 and it can be either precocious or late. 6 The first manifests during the first three months of therapy, and reflects an immune response against an active (often quiescent) infection by opportunistic pathogens. The second is an immune response against the antigens of non-viable pathogens. Here, we report two cases of BCG-itis related to precocious IRIS.
FIRST CASE PRESENTATION
Patient 1 was a female infant, delivered by Caesarean section, weighting 3.280 g at birth and was breastfed from birth until five months of age, when she presented with respiratory failure and pneumonia. In addition to antimicrobial therapy, she received intravenous trimethoprim-sulphamethoxazole and glucocorticoid due to the suspicion of Pneumocystis jirovecii infection. Her initial plasma HIV-1 RNA was 5.1 log10 copies/mL and the blood CD4% was 13.3%. Two weeks after recovery, she was treated with zidovudine, lamivudine, lopinavir/ritonavir and secondary prophylaxis for Pneumocystis. Forty-one days later, she returned with ulceration of 2 cm of diameter ipsilateral to her BCG vaccination scar and extensive suppurative axillary lymphadenitis (Figure 1). BCG-itis was associated with IRIS was diagnosed due to the undetectable RNA HIV-1 level and the increase of CD4 T-cell count to 22%. Isoniazid (10 mg/kg/day) was administered for four months, with complete regression of the manifestations. The lesion was not handled.
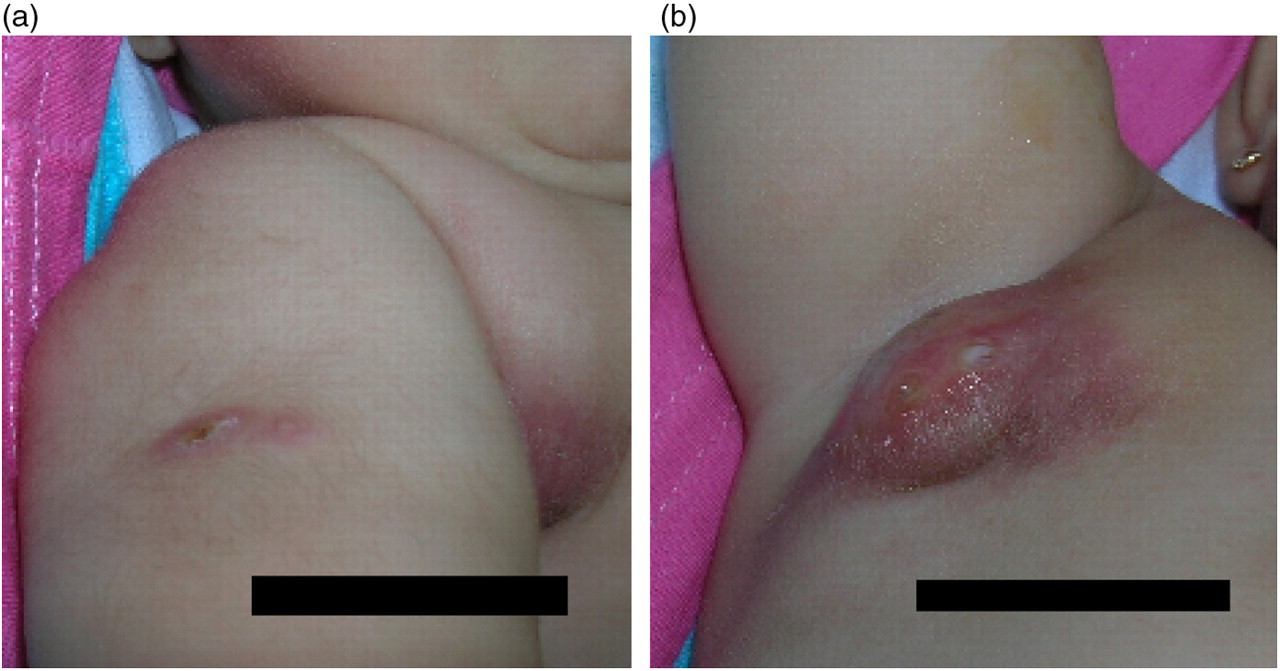
BCG vaccine-induced complication presenting 41 days after starting HAART: (a) Ulceration at BCG vaccination site (right deltoid); (b) ipsilateral suppurative axillary lymphadenitis. BCG, Bacille Calmette-Guérin; HAART, highly active antiretroviral therapy
SECOND CASE PRESENTATION
Patient 2, a 2.545 g female infant, was born to a known HIV-positive woman who did not adhere to antiretrovirals during pregnancy and had suffered reactivation of Toxoplasma infection resulting in vertical transmission. At age five days, therapy with oral pyrimethamine, sulphadiazine, plus supplemental folinic acid was started, and she was treated for 12 months. Trimethoprim–sulphamethoxazole for Pneumocystis pneumonia prophylaxis was not prescribed because of the potential for increased toxicity. Zidovudine was prescribed for six weeks to prevent vertical transmission of HIV. At two months of age, infection by HIV was confirmed: viral load was 1.2 log10 copies/mL and the CD4 was 27.2% (1.378 cells/mm3). At six months of age, stavudine, lamivudine and lopinavir/ritonavir were started due to failure to thrive and multiple infections. Eighteen days later she presented with regional axillary adenitis, ipsilateral to her BCG vaccination scar (not shown). At the time, HIV viral load was 11400 copies/mL and CD4 was 30%. The lesion was not handled, and isoniazid (10 mg/kg/day) was prescribed for three months. Her recovery was complete.
DISCUSSION AND CONCLUSION
Both cases of BCG-itis resulted from precocious IRIS, with adenopathies occurring 41 and 18 days after commencement of HAART, respectively. They occurred in a cohort of 78 HIV-infected children, 77 of whom were BCG-Moureau vaccinated in their first month of life, performed in our service.
Both cases fulfilled two major established criteria for diagnosis of IRIS: localized disease (lymph nodes) with exaggerated inflammatory reaction without another likely cause, and associated decrease in plasma HIV RNA level by >1 log 10 copies/mL. 6,7 They also complied with a third, yet considered minor, diagnostic criterion for IRIS: increased blood CD4 T-cell counts after HAART.
The prognosis in both cases was excellent, resulting in cure, with the use of isoniazid until regression of the adenopathies, following recommendation by the Brazilian Ministry of Health on adverse reactions to BCG. Caution is advised about the risk of pre-existing isoniazid resistance, and the potential development of drug resistance. 8 Spontaneous resolution is common in BCG-itis, even without active treatment. 7
Although confirmation of the clinical diagnosis of IRIS should include viral load and CD4 counts, genotyping and/or culture of M. bovis from an aspirate of the ipsilateral axillary adenitis/abscess to confirm the microbial diagnosis in our setting of investigative time. We guided management by the response to HIV treatment and reconstitution of immunity, without genotyping and/or culture of M. bovis.
Currently, WHO recommends BCG vaccination deferral in HIV-exposed infants and contraindicates BCG vaccine in HIV-infected infants. 2 We believe that depriving children exposed to HIV infection of the benefit of BCG vaccination is not the best solution. In settings where HIV prevalence is high and BCG is routinely given at birth, prevention programmes of mother-to-child transmission of HIV allow effective follow-up and precocious treatment, decreasing the number of cases of severe immunosuppression, and consequently of BCG-related IRIS.
Footnotes
Acknowledgements
The authors would like to thank the children and their families who consented to this report. The authors are grateful to the members of the Specialized Assistance Service for HIV/AIDS, the Voluntary Counselling and Testing Centre for HIV and AIDS of the Municipal Program for the Surveillance of STD and AIDS of the city of Campos of Goytacazes for their support. This study was financed by the Municipal Health Department of the city of Campos dos Goytacazes, the National Program for STD/AIDS and by a grant from the Ministry of Ministry of Health/UNESCO to E.M-A.