
Abstract
This is the guideline for genital herpes simplex virus (HSV) management for the IUSTI/WHO Europe, 2010. They describe the epidemiology, diagnosis, clinical features, treatment and prevention of genital HSV infection. They include details on the management of HSV in pregnancy, those who are immunocompromised and the clinical investigation and management of suspected HSV-resistant disease.
Keywords
SEARCH STRATEGY
Evidence for this guideline was provided by review of the Medline/Pubmed, Embase, Google, Cochrane Library and relevant guidelines up to September 2008. A Medline/Pubmed and Embase search was carried out from January 1981 to September 2008, looking for the following terms in the title or abstract: ‘herpes simplex virus (HSV)/herpes’, ‘genital ulcers’, ‘HSV/herpes pregnancy’, ‘neonatal HSV/herpes’ and ‘HSV/herpes drugs’. For some specific recommendations, additional Medline/Pubmed search was performed when necessary. Google search was performed in September 2007 with the search term ‘HSV guideline(s)’ and all relevant documents of the first 150 search results were reviewed. A search of the Cochrane Library included Cochrane Database of Systematic Reviews, Database of Abstracts of Reviews of Effects and Cochrane Central Register of Controlled Trials. The 2001 European guideline for the management of genital herpes was the main source for the present guideline. In addition, the following guidelines were reviewed in detail: 2006 US Centers for Disease Control and Prevention (CDC) sexually transmitted disease guidelines and 2007 British Association for Sexual Health and HIV (BASHH) national guideline for the management of genital herpes.
INTRODUCTION
First infection with either herpes simplex virus type 1 (HSV-1) or type 2 (HSV-2) is termed primary infection and results in either symptomatic disease at the site of viral entry (i.e. on the face or genital area) or asymptomatic, and thus unrecognized, infection. In addition, there may be systemic symptoms, as with other acute viral illnesses. Following infection, the virus becomes latent in the local sensory ganglion, periodically reactivating to cause symptomatic lesions, or undergo asymptomatic, but nonetheless infectious, viral shedding. Genital herpes can be caused by either HSV-1 – the usual cause of oro-labial herpes – or by HSV-2. Infection with either virus can cause an identical initial illness; however, the actual clinical presentation may depend upon previous HSV-1 or HSV-2 infection, and previous sites of infection. Subsequent recurrence frequency is greater for HSV-2 than for HSV-1 disease when infection involves the genital area.
Transmission risk
Risk of transmission appears to be greatest during lesional recurrences or prodrome, and patients should be advised to abstain from sexual contact during this time. Transmission can occur in the absence of lesional recurrence as a result of subclinical viral shedding. Efficacy of condoms to prevent sexual transmission has not been formally assessed; however, indirect evidence from failed vaccine trials provides strong support for their consistent usage (IIb, B). 1,2
DIAGNOSIS
Clinical diagnosis
Although classical genital herpes can be recognized by the presence of typical papular lesions progressing to vesicle and ulcer formation, associated with local adenitis and in recurrent cases preceded by prodromal symptoms, the features in many patients can be highly variable. The majority of patients will suffer from atypical lesions where signs may be easily confused with other genital dermatoses. In atypical cases, relying upon clinical diagnosis alone should be avoided whenever possible.
Laboratory diagnosis
Virus detection (see Table 1)
Laboratory confirmation is recommended in all patients with suspected genital herpes, using methods that directly demonstrate the virus in genital specimens, typically swabs taken from the base of the lesion (vesicles should be unroofed with a needle or scalpel blade) and placed in viral transport medium (Ib, A); 3
HSV typing into HSV-1 and HSV-2 is recommended in all patients with first-episode genital herpes to guide counselling and management (III, B); 1
As HSV shedding is intermittent, testing swabs from asymptomatic patients is not recommended for routine diagnosis since it is unlikely to yield confirmation of carrier status (Ib, A); 1
Virus isolation in cell culture has long been regarded as the diagnostic gold standard. Advantages include high specificity and recovery of virus isolates that can be typed into HSV-1 and HSV-2 and tested for antiviral susceptibility. However, virus culture is slow (7–10 days for a negative result), labour-intensive and poorly sensitive. 4 Levels of virus shedding (e.g. in first versus recurrent episodes and in early versus late presentations) significantly influence sensitivity. Delayed sample processing and lack of refrigeration after collection significantly reduce diagnostic yield; 5,6
HSV DNA detection by realtime polymerase chain reaction (PCR) increases HSV detection rates in muco-cutaneous swabs by 11–71% compared with virus culture and is recommended as the preferred diagnostic method (Ib, A). 3,7,8 Realtime PCR can tolerate less stringent conditions for sample storage and transport than virus culture, and allows the rapid detection and typing of HSV with a lower risk of contamination than traditional PCR assays;
Viral antigen can be detected by direct immunofluorescence assay using fluorescein-labelled monoclonal antibodies on smears, or by enzyme immunoassay (EIA) on swabs. These assays are 10–100-fold less sensitive than virus culture and are not generally recommended (Ib, A). 9–11 As EIA performs satisfactorily in symptomatic patients, it may offer a rapid diagnostic alternative in settings with limited laboratory facilities. EIA may not differentiate between HSV types;
Cytological examination (Tzanck and Papanicolaou smears) has modest specificity and sensitivity and is not recommended for diagnosis (Ib, A).
Laboratory methods for HSV detection
HSV = herpes simplex virus; EIA = enzyme immunoassay; PCR = polymerase chain reaction
*New methods to identify aciclovir-resistance in HSV using genotyping have been developed and published, and are likely to supplant phenotypic testing in the next few years. However, such methods are currently unavailable in clinical practice
HSV type-specific serology
Serological testing is not routinely recommended in asymptomatic patients (IV, C), but is indicated in the following groups:
1,12–17
History of recurrent or atypical genital disease when direct virus detection methods have been negative (III, B). HSV-2 antibodies are supportive of a diagnosis of genital herpes; HSV-1 antibodies do not differentiate between genital and oropharyngeal infection. Counselling of HSV-2 IgG-negative, HSV-1 IgG-positive patients should take into account that HSV-1 is an uncommon cause of recurrent genital disease;
1
First-episode genital herpes, where differentiating between primary and established infection, guides counselling and management (III, B). At the onset of symptoms, the absence of HSV IgG against the virus type detected in the genital lesion is consistent with a primary infection.
1
Seroconversion should be demonstrated at follow-up; Sexual partners of patients with genital herpes, where concerns are raised about transmission. Serodiscordant couples can be counselled about strategies to reduce the risk of infection and disease (Ib, A);
Testing of asymptomatic pregnant women is not routinely recommended, but is indicated when there is a history of genital herpes in the partner (IIb, B). 18–20 HSV-1 and/or HSV-2 seronegative women should be counselled about strategies to prevent a new infection with either virus type during pregnancy;
HSV-2 carriers who engage in high-risk sexual behaviour should be counselled about the increased risk for HIV acquisition (Ia, A); 21
Testing of HIV-infected patients is not routinely recommended (IV, C). Although HSV-2 seropositivity increases the risk of HIV transmission and frequent HSV recurrences augment HIV replication, there is limited evidence to inform the management of HSV-2 co-infection in HIV-infected patients without symptoms of genital herpes; 19,22,23
Limited data suggest an increased risk of perinatal HIV transmission among HSV-2 seropositive HIV-infected women. 24,25 As evidence is not consistent, testing of HIV-positive pregnant women is not routinely recommended (IV, C); 26
HSV serological assays should be used that detect antibodies against the antigenically unique glycoproteins gG1 and gG2.
11,27
Non-type-specific HSV antibody assays are of no value in the management of genital herpes:
Western blot is the diagnostic gold standard. It is >97% sensitive and >98% specific, but is labour-intensive and not commercially available;
28,29
Several commercial (e.g. Focus HerpeSelect ELISA and Immunoblot; Kalon HSV-2 assay) and in-house assays are available, with reported sensitivities >95% and generally high specificities. Specificity, however, can vary significantly in different populations (ranging from as low as 40% to >96%).
30–39
False-negative results are more likely to occur in early infection and can be resolved by repeat testing. False-positive results have been observed in populations with low prevalence and in some African cohorts.
40
Rapid point-of-care tests are available (e.g. Biokit HSV-2 assay, previously POCkit™HSV-2, with sensitivity and specificity >92%) and new assays are being developed;
41
HSV seroprevalence rates, presence of risk factors for genital herpes and clinical history influence the positive predictive value of HSV type-specific serology and should guide testing and result interpretation (III, B).
13,25–34
Various enzyme-linked immunosorbent assay (ELISA) interpretation algorithms are being evaluated. Currently, when using the Focus HSV-2 ELISA in a low-risk or heterogeneous setting, the index value for interpreting positivity should be raised from >1.1 to ≥3.5 (IIa, B), taking into account that this reduces sensitivity for both early and established infection.
29,30,33
Samples with values between 1.1 and 3.5 should undergo confirmation by an alternative method (e.g. Biokit HSV-2 or Kalon ELISA) (IIa, B). The specificity of the Kalon assay improves by raising the cut-off to 1.5 (IIa, B). The assay has performed comparatively or better than the Focus ELISA in comparative studies.
32,34
Concordance between the Focus ELISA and the Kalon assay is 99% using a Focus assay cut-off of 3.5;
33
Type-specific HSV IgG becomes detectable two weeks to three months after the onset of symptoms and is commonly negative in early presentations.
25
Where clinically indicated, follow-up samples should be taken to demonstrate seroconversion (IIa, B). HSV IgM testing substantially increased the ability to detect early infection in patients who lack detectable IgG (IIb, B).
42
HSV IgM testing, however, has limited availability in routine diagnostic settings. In addition, IgM testing can also be positive during reactivation of disease and negative during primary disease, and is not viral-type specific. Because of these limitations, the test cannot be recommended in routine clinical practice.
MANAGEMENT
First-episode genital herpes
Indications for therapy
First episodes of genital herpes are frequently associated with a prolonged disease course. Untreated, many patients suffer general and local complications. Therapy can be highly effective and should be instigated at the earliest opportunity and on clinical suspicion alone.
Antivirals
Patients presenting within five days of the start of the episode, or while new lesions are still forming, should be given oral antiviral drugs. Aciclovir, valaciclovir and famciclovir are all effective in reducing the severity and duration of episode (Ib, A). 43,44 No therapy alters the natural course of genital herpes infection.
Topical agents are not only less effective than oral agents, but also the use of topical aciclovir has been associated with aciclovir-resistant strains. 45 Hence they cannot be recommended (IV, C).
The only indication for the use of intravenous therapy is when the patient is unable to swallow or tolerate oral medication because of vomiting.
The recommended regimens – all for five days – are as follows:
Aciclovir 200 mg five times a day; Aciclovir 400 mg three times a day; Famciclovir 250 mg three times a day; or Valaciclovir 500 mg two times a day.
Choice should be made by individual clinicians, taking cost of therapy and likely compliance into account. A number of patients will have extended episodes beyond five days. Patients with sustained systemic symptoms, new lesion development and complicated disease should continue therapy beyond five days.
Supportive measures
Saline bathing and the use of appropriate analgesia are recommended. Although the potential for sensitization exists in the use of topical anaesthetic agents, lignocaine is a rare sensitizer and can be used safely in genital herpes in the form of gel or ointment. 46 Benzocaine, however, is a potent sensitizer and should not be used (IV, C).
Counselling
It is important to be frank about transmission risks including subclinical shedding and the limited impact of condoms and antivirals. Advice on disclosure should be practical and tailored to the patient's personal situation. The low physical morbidity and high population prevalence should be stressed. Clear information about pregnancy is important both to men and women. High distress at diagnosis is common, often persists with recurrences and may be reduced by antivirals (Ib, A). 47–49 Most patients require one or two sessions but adjustment is difficult to predict and careful follow-up is important with more intensive input for those who do not adjust within three to six months.
Management of complications
Hospitalization may be required for urinary retention, meningism, severe constitutional symptoms or adverse social circumstances. If catheterization is required, consideration should be given as to whether a suprapubic approach offers better symptom control to the individual patient.
Superinfection of lesions is rare, but may occur during the second week. This is characterized by the recrudescence of local symptoms. Candida is most often implicated and is easily diagnosed and treated.
Special situations – HIV-positive patients with first-episode genital herpes
There are no controlled trials on duration and dose of treatment. Some clinicians advocate a 10-day course of treatment at twice the standard dose of any of the usual agents (IV, C).
Information for patients
The following information should be discussed when counselling patients with first-episode genital herpes:
The course of infection, including subclinical shedding; Treatment options; The risk of transmission, and interventions that may limit or reduce the risk of transmission; The risk of transmission to the infant at birth. The patient should be counselled to inform the obstetrician or midwife; The possibility of partner notification and the possible source of infection.
Follow-up
Patients are followed-up until the episode has resolved and counselling is considered complete. Further follow-up may be required to exclude other causes of genital ulceration that may be co-existent. Patients should be invited to reattend should recurrences be problematic.
Recurrent genital herpes
Indications for therapy
Genital herpes recurrences are self-limiting and generally cause minor symptoms. Decisions about how best to manage clinical recurrences should be made in partnership with the patient. Management strategies include supportive therapy only, episodic antiviral treatments and suppressive antiviral therapy. The most appropriate strategy for managing an individual patient may vary over time according to recurrence frequency, symptom severity and relationship status. For most patients, management will need to be supportive only, with simple local measures such as saline bathing or topical petroleum jelly being adequate.
Episodic antiviral treatment
Oral aciclovir, valaciclovir and famciclovir are effective at reducing the duration and severity of recurrent genital herpes. The reduction in duration is a median of 1–2 days (Ib, A). 50–52 Head-to-head studies of their effects show no advantage of one therapy over another, or the advantage of extended five-day treatment over ultra-short therapy. Prodrugs offer simplified twice-a-day dosing. It is likely that patient-initiated treatment started within 24 hours is most likely to be effective. Aborted lesions have been documented in up to one-third of patients with early treatment. 53 To ensure prompt treatment, patients should be advised to carry a small quantity of drugs at all times.
The recommended regimens – all for five days – are as follows:
Aciclovir 200 mg five times daily; Aciclovir 400 mg three times daily for 3–5 days; Valaciclovir 500 mg twice daily; or Famciclovir 125 mg twice daily.
Short-course therapies are as follows:
Suppressive therapy
The majority of early trials of suppressive therapy were done in patients with a recurrence rate equivalent to ≥6 recurrences/annum. More recently, studies have been completed in patients with milder disease including those with only serological evidence of infection. These indicate that patients across all spectrums of disease will benefit from a reduced rate of recurrence with treatment. The frequency of recurrence at which it is worth starting suppressive therapy is a subjective issue and needs to balance the frequency of recurrence and the impact of disease on the individual against the cost and inconvenience of treatment.
All patients are highly likely to experience a substantial reduction in recurrence frequency on suppressive antiviral therapy. However, the majority of patients on such a regimen will still experience an occasional symptomatic recurrence.
Experience with suppressive antiviral therapy is most extensive with aciclovir (Ib, A). 61 Safety and resistance data on patients on long-term therapy now extends to over 18 years of continuous surveillance. Although not essential, it may be prudent to regularly assess the need for continuing therapy, since patient circumstances may alter significantly. However, even after prolonged periods of suppression, many patients do not find a significant alteration in disease frequency or severity upon discontinuation and reassessment.
Recommended regimens
The optimal total daily dose of suppressive aciclovir therapy is 800 mg. The only published clinical dose-ranging study concluded that 200 mg four times a day was marginally superior to 400 mg twice daily (P < 0.02) (IIb, B). 62 However, ability to comply with a four times a day dosing regimen should determine prescribing decisions for individual patients.
Twice-daily valaciclovir (250 mg twice daily) has been shown to be as effective as twice-daily aciclovir (400 mg twice daily). Once-daily aciclovir does not suppress genital herpes recurrences. There is some debate as to whether once-daily therapy is as effective as twice-daily therapy with valaciclovir. For those patients experiencing <10 recurrences per annum, a dose of 500 mg daily valaciclovir will be adequate; for those patients experiencing >10 recurrences per annum, 250 mg twice daily or 1 g once a day is required. 63
No major clinically significant differences between suppressive therapy with valaciclovir (500 mg daily) and famciclovir (250 mg twice daily) have been documented (IV, C). 64 In patients with an insufficient clinical response, the daily suppressive dose of valaciclovir or famciclovir may have to be doubled (IV, C). Routine blood monitoring of standard dose therapy is not required. Occasionally, a mild headache or nausea may occur with valaciclovir.
The decision to continue suppressive therapy should be reviewed at least annually. Discontinuation of therapy at this time, if the patient is willing, will allow a reassessment of recurrence frequency.
A small number of patients will experience a reduction in recurrence frequency compared with presuppression symptomatic levels. The minimum period of assessment should include two recurrences to allow a view to be taken both on the frequency and severity. It is safe and reasonable to restart treatment in patients who continue to have significant disease (IV, C).
Short courses of suppressive therapy to prevent clinical symptoms may be helpful for some patients (e.g. for holidays, exams, etc.). Clinicians need to note that full suppressive effect is usually only obtained five days into treatment.
Viral shedding and transmission on suppressive therapy
Subclinical shedding of infectious virus occurs in most individuals with genital HSV-1 and/or HSV-2. Viral shedding is more likely to occur in patients with genital HSV-2, in the first year after infection, or in individuals with frequent symptomatic recurrences. Aciclovir, valaciclovir and famciclovir all suppress symptomatic and asymptomatic viral shedding.
Even if it seems biologically plausible, partial suppression of viral shedding does not necessarily equate to reduce transmission. However, suppressive therapy with valaciclovir 500 mg a day (in those with 10 or fewer recurrent episodes per year) significantly reduced transmission – by nearly 50% – in serodiscordant couples (Ib, A). 65 Hence, suppressive valaciclovir therapy may be considered in addition to the use of condoms and selective sexual abstinence.
SPECIAL SITUATIONS
Management of HSV in the immunocompromised and HIV-positive patient
Management of initial episode HSV
There are no trial data for any antiviral in initial episode genital HSV in HIV-infected patients.
The vast majority of adults with HIV have serological evidence of established HSV-1 and 2 infections making acquisition trials extremely difficult to perform. Case studies report that acquisition of genital HSV may be associated with a prolonged and uncertain clinical course. Systemic symptoms may predominate and chronic lesions may become established if immunological clearance of the skin does not occur. In the absence of data, most authorities advise that multiples of the standard levels of treatment for first-episode HSV be used in the immunocompromised. However, for those with HIV these may not always be required particularly for those with normal CD4 counts.
In patients with advanced HIV, double the standard dose of antiviral should be considered and if new lesions continue to form at days 3–5 a higher dose should be considered. In addition, if fulminant disease ensues that intravenous aciclovir be substituted. Recommended initial doses are as follows:
Aciclovir 200–400 mg five times daily, 400 mg–800 mg three times daily (IV, C); Valaciclovir 500 mg–1 g twice daily (IV, C); Famciclovir 250–500 mg three times daily (IV, C).
Treatment should be given for 5–10 days or at least until all lesions have re-epithelialized – this will often exceed the usual 10-day duration of treatment that is given to HIV-negative patients.
Management of recurrent disease
A number of trials of antiviral therapy in the immunocompromised have been reported.
Duration of therapy
It is likely that five days of therapy will be adequate for most patients. It should be noted that with advanced HIV 13–17% of patients have been reported to have new lesions developing at the end of a seven-day course of treatment. 66 Shorter courses of therapy may be adequate in those with good CD4 counts (>500) although only one trial with famciclovir has reported this effect (1b,B). 54
Dosage of antivirals
Standard doses of antivirals should suffice in those with no evidence of immune failure (1b, A). In those with advanced disease, it may be necessary to double the standard dose and to continue therapy beyond five days (1b, B). Caution should be exercised in using ultrashort courses of episodic therapy since these have not been evaluated fully in the immunocompromised.
Suppressive therapy
Suppressive antiviral therapy for HSV is effective and well tolerated. All three agents have been trialled. Standard suppressive doses of aciclovir are effective. Valaciclovir is more effective when given twice daily (500 mg twice a day) compared with once-daily dosing (1000 mg). 67 The valaciclovir 500 mg once-daily dose has not been evaluated in the HIV-positive patient. Trial data for the efficacy of high-dose famciclovir are only available over much shorter durations. 68 There is a considerable body of data on the safety of oral antivirals in the HIV-positive immunocompromised host. Two studies in the pre-highly active antiretroviral therapy (HAART) era looked at high-dose aciclovir (400 mg four times daily) and more recently at standard dose regimens. 66,69,70 For valaciclovir a number of studies looked at the value of valaciclovir for the suppression of recurrent genital herpes. 66 High-dose valaciclovir (2 g four times daily) has been studied and reported in HIV-positive people, and those immunosuppressed and recovering from bone marrow transplants. Most recently, a large number of studies looking at the efficacy of aciclovir and valaciclovir suppression and its impact on HIV transmission from co-infected patients have reported. These trials indicate that use of oral aciclovir at standard dose and valaciclovir at 1 g once daily and 500 mg twice daily is associated with little or no adverse effect or toxicity as compared with the non-HIV positives. High-dose valaciclovir (8 g daily) has been associated with microangiopathic haemolytic uraemic syndrome. 71
Dosage
The best evidence to achieve suppression exists for valaciclovir 500 mg twice daily and aciclovir 400 mg twice daily (1b, A). If a lack of suppression on these standard doses is noted, the first option should be to double the dose of the agent; if this is not successful at controlling disease then famciclovir 500 mg twice daily could be tried (IIa, B).
Management of recalcitrant herpes in immunocompromised individuals
Although rare in immunocompetent individuals, clinically refractory lesions due to genital HSV are a major problem in patients with severe immunodeficiency, including late-stage HIV diseases and patients with immune reconstitution inflammatory syndrome following combination antiretroviral therapy. Algorithms for treatment in such situations are shown in Figure 1.
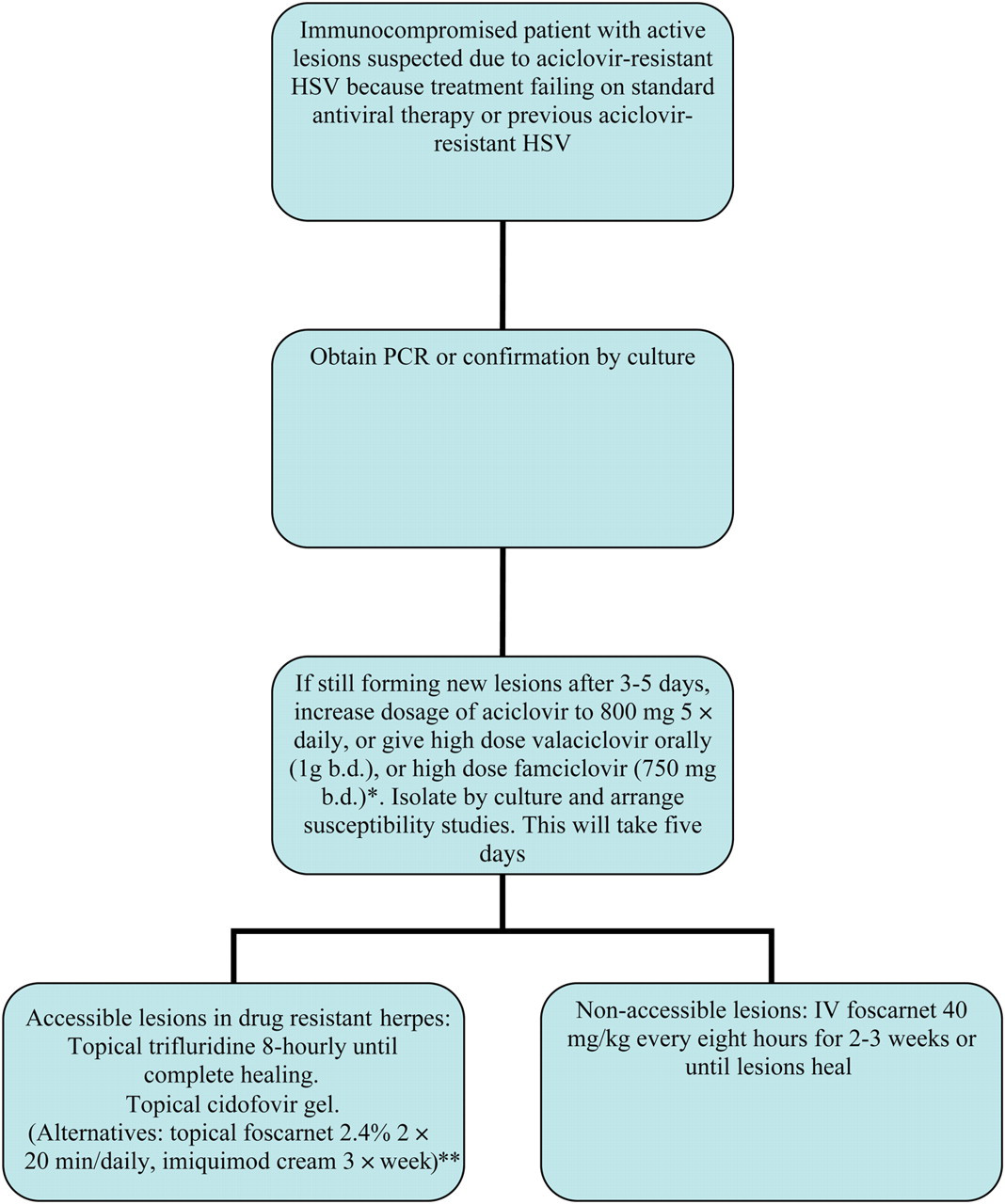
Algorithm for the treatment of herpes in immunocompromised individuals. HSV= herpes simplex virus; PCR= polymerase chain reaction; b.d.= twice daily. *All HSV strains resistant to aciclovir are also resistant to valaciclovir. **Some of these products might have to be made up in-house
HSV suppression to limit HIV progression
Suppressive antiviral therapy with aciclovir or valaciclovir has been shown to decrease the levels of HIV viraemia in those patients with detectable HIV viral loads through a mechanism not yet fully elucidated. 72 Such a strategy will impact on HIV progression, particularly for those individuals not on HAART. A large randomized controlled trial in early HIV (those individuals not on HAART and with CD4 counts above 250) has shown that standard doses of suppressive antiviral therapy (aciclovir 400 mg twice daily) will sustain CD4 counts above accepted treatment levels and this effect reduced the need for HAART at two years by 16% in the treatment group. 73
Management of partners
There is no evidence on which to base recommendations for partner notification. On an individual basis, it may be appropriate to offer to see partners to help with the counselling process. Partner notification in relation to pregnancy is discussed below.
It is worth considering the following points when counselling patients:
The use of condoms is advisable also in case of suppressive antiviral treatment;
16
Asymptomatic shedding plays a major role in the transmission of HSV infection; Partner notification is an effective way of detecting uninfected or asymptomatic individuals when combined with type-specific antibody testing; Up to 50% of asymptomatic HSV-2 seropositive women can be taught to recognize genital herpes recurrences after counselling. It may be possible to reduce the risks of transmission by educating patients to recognise symptomatic recurrences; Virus transmission can be reduced either with suppressive antiviral treatment or by using condoms.
Management of pregnant women with first-episode genital herpes
First and second trimester acquisition
Management of the woman should be in line with her clinical condition and will often involve the use of either oral or intravenous aciclovir in standard doses;
Providing that delivery does not ensue, the pregnancy should be managed expectantly and vaginal delivery anticipated (IV, C);
Daily suppressive aciclovir 400 mg three times daily from 36 weeks gestation may prevent HSV lesions at term and hence the need for delivery by Caesarean section (Ib, B). 74–79
Third trimester acquisition (IV, C)
Caesarean section should be considered for all women, particularly those developing symptoms within six weeks of delivery, as the risk of viral shedding in labour is very high (Ib, B);
Daily suppressive aciclovir 400 mg three times daily from 36 weeks gestation may prevent HSV lesions at term;
If vaginal delivery is unavoidable, prolonged rupture of membranes and invasive procedures, including the use of scalp electrodes, should be avoided. Intrapartum intravenous aciclovir given to the mother and subsequently to the baby may be considered and the paediatrician should be informed. 80
Management of pregnant women with recurrent genital herpes (III, B)
Women with recurrent genital herpes should be informed that the risk of neonatal herpes is low.
Symptomatic recurrences of genital herpes during the third trimester will be brief; vaginal delivery is appropriate if no lesions are present at delivery; For women with a history of recurrent genital herpes who would opt for Caesarean section if they had HSV lesions at the onset of labour, daily suppressive aciclovir 400 mg three times daily from 36 weeks gestation may prevent HSV lesions at term and hence the need for delivery by Caesarean section (Ia, A);
81
If there are no genital lesions at delivery, there is no indication for Caesarean section to prevent neonatal herpes; Sequential cultures or PCR during late gestation to predict viral shedding at term are not indicated;
82
The utility of taking cultures or PCR at delivery, in order to identify women who are asymptomatically shedding HSV, is unproven.
Management of recurrent HSV in early pregnancy
Although the safety of aciclovir in early pregnancy is not fully established, judicious use of this agent for suspected acquisition episodes is widely advocated. The same cannot be said for recurrent disease. Continuous or episodic therapy is not recommended in early pregnancy and should be avoided. Clinicians are on occasion obliged to use therapy for severe and complicated disease and a case-by-case assessment should be made. Newer antivirals should be avoided and the dose of aciclovir titrated down to the minimum effective level.
Management of HIV-positive women with recurrent HSV infection (IV, C)
There is some evidence that HIV antibody positive women with genital HSV ulceration in pregnancy are more likely to transmit HIV infection independent of other factors.
83,84
However, this is not a consistent finding across all studies.
85
Women who are HIV antibody positive and have a history of genital herpes should be offered daily suppressive aciclovir 400 mg three times daily from 32 weeks gestation to reduce the risk of transmission of HIV-1 infection especially in women where a vaginal delivery is planned. Starting therapy at an earlier gestation than usual should be considered in view of the increased possibility of preterm labour (IV, C); There is currently no evidence to recommend daily suppressive treatment for HIV-1 antibody positive women who are HSV-1 or -2 seropositive but have no history of genital herpes.
86
Management of women with genital lesions at the onset of labour
Caesarean section may be considered for women with recurrent genital herpes lesions at the onset of labour, but the risk of neonatal herpes following vaginal delivery is small and must be set against risks to the mother of Caesarean section. Evidence from the Netherlands shows that a conservative approach, allowing vaginal delivery in the presence of an anogenital lesion, has not been associated with a rise in numbers of neonatal HSV cases (III, B). 87 However, this approach can only be adopted if fully supported by obstetricians and neonatologists, and if consistent with local medicolegal advice;
Clinical diagnosis of genital herpes at the time of labour correlates relatively poorly with HSV detection from genital sites by either culture or PCR and fails to identify women with asymptomatic HSV shedding.
Note: None of the antiviral drugs is licensed for use in pregnancy, but the use of aciclovir in pregnancy has not been associated with any consistent pregnancy or fetal/neonatal adverse effects, 87 other than transient neutropenia. 88 Safety data for aciclovir may be extrapolated to valaciclovir in late pregnancy, as it is the valine ester, but there is less experience with use of valaciclovir. 89 Famciclovir should currently be avoided.
Prevention of acquisition of infection (IV, C)
Maternal risk of HSV acquisition in pregnancy varies geographically and local epidemiological surveillance should guide strategy for prevention. Any strategy for prevention of neonatal herpes needs to involve both parents.
All women should be asked at their first antenatal visit if they or their partner have had genital herpes; Female partners of men with genital herpes, but without a personal history of genital herpes should be advised about reducing their risk of acquiring herpes in pregnancy and of subsequent transmission to their baby. Strategies include conscientious use of condoms during pregnancy especially in the last trimester of pregnancy, abstaining from sex at the time of lesional recurrences and in the last six weeks of pregnancy; Daily suppressive treatment has been shown to significantly reduce the risk of transmission of HSV to a seronegative partner; however, the effectiveness of suppressive treatment of the male partner to reduce transmission to a pregnant woman has not been evaluated so can currently only be recommended with caveats; Pregnant women should be advised of the risk of acquiring HSV-1 as a result of receptive orogenital contact especially in the last trimester of pregnancy; Identifying susceptible women by means of type-specific antibody testing has not been shown to be cost-effective and is not indicated in Europe; All women, not just those with a history of genital herpes, should undergo careful vulval inspection at the onset of labour to look for clinical signs of herpes infection; Mothers, staff and other relatives/friends with active oral HSV lesions or herpetic whitlow should be advised to avoid direct contact between lesions and the neonate.
Management of the neonate
Babies born to mothers with first-episode genital herpes at the onset of labour
The paediatrician should be informed;
HSV PCR of urine and stool, from the oropharynx, eyes and surface sites, should be taken to allow early identification of infected babies;
The potential benefits and risks of starting intravenous aciclovir without waiting for the results of these cultures should be discussed;
If aciclovir is not started immediately the neonate should be closely monitored for signs of lethargy, fever, poor feeding or lesions.
Babies born to mothers with recurrent genital herpes at the onset of labour
Although some clinicians feel that taking a set of specimens for viral culture collected after delivery may help with early identification of infection, there is no evidence to support this practice. However, health-care workers and parents should be advised to consider HSV in the differential diagnosis if the baby shows any signs of infection or develops skin, eye or mucous membrane lesions, particularly in the first two weeks of life.
Footnotes
ACKNOWLEDGEMENTS
Simon Barton, George Kinghorn, Helen Lotery, Anna Wald are acknowledged.
IUSTI/WHO European STD guidelines Editorial Board: Keith Radcliffe (Editor-in-Chief), Marita van de Laar, Michel Janier, Jorgen Skov Jensen, Martino Neumann, Raj Patel, Jonathan Ross, Willem van der Meijden, Pieter van Voorst Vader, Harald Moi.