
Abstract
Being lost to follow-up (LTFU) is a major problem in caring for persons with HIV infection. We describe the proportions and characteristics of LTFU in a Belgian outpatient HIV clinic. All patients treated with highly active antiretroviral therapy (HAART) who attended at least two consultations were included. Patients not returning within the following year were considered LTFU. Multivariate analysis using logistic regression was performed. The LTFU rate was 5.5% on average and remained stable over the years. Patients LTFU were more often intravenous drug users (odds ratio [OR] = 3.48), not covered by health insurance (OR = 6.69), living outside the province (OR = 1.49) and treated with a complex initial HAART regimen (OR = 5.80). Increased age was also associated with a higher risk of LTFU. Patients at risk for LTFU after starting HAART should be the targeted for reinforced counselling and HIV treatment centres should establish systems to trace patients LTFU.
INTRODUCTION
Key for the success of the treatment of patients with HIV/AIDS is retention in follow-up and perfect adherence to the treatment regimen. 1,2 Retention in care is keeping patients in follow-up (meaning regular medical visits). Poor retention in care has a negative impact on survival. 3
Lost to follow-up (LFTU) refers to all patients out of care. LTFU is a problem for the care of all patients with chronic diseases, in the developed as well as in the developing world. 4–6 Reported annual LTFU rates for persons with HIV infection vary between 5% and 44%, 7–9 and different risk factors have been linked to LTFU. 2 Most guidelines recommend follow-up visits every three to four months for HIV-infected patients treated with highly active antiretroviral therapy (HAART). 10 The purpose of these visits is to monitor the efficacy and possible side-effects of the treatment.
This study describes the LTFU rates and factors associated with LTFU in a cohort of HIV-infected patients treated with HAART and followed up at the outpatient clinic of the Institute of Tropical Medicine (ITM) in Antwerp, Belgium. This clinic is an AIDS reference centre for the province of Antwerp.
METHODS
Study population
HIV-positive patients, attending the ITM outpatient clinic between 30 June 1999 and 30 June 2009, over 18 years of age and treated with HAART were included in the analysis. HAART was defined as a treatment regimen with at least three drugs from two ARV drug classes as well as the co-formulation zidovudine/lamivudine/abacavir. Patients were included only if they had been seen twice at the ITM clinic within one year; this was to avoid inclusion of patients who came only once for a second opinion or HIV-status testing.
Definition of lost to follow-up
We considered someone LTFU if he/she did not return for a follow-up visit the year (365 calendar days) after the last recorded visit. One person could be LTFU on several occasions during the study period. Only the first episode of LTFU was taken into account during analysis. We considered the year of LTFU, the year of the last recorded visit or the year before the interruption in follow-up. LTFU rate was defined as the proportion of LTFU at the end of each calendar year, and was calculated using the number of LTFU events at the end of each calendar year divided by the number of patients under follow-up at the start of each year. Patients known to have died or to have been transferred out were not considered as LTFU.
Statistical analyses
LTFU rates were calculated for each calendar year, and confidence intervals around these estimates were calculated using the Wilson's score method. We examined both categorical and continuous baseline data as possible factors associated with LTFU. The categorical variables were: language spoken (Dutch, French, English or other), gender, age group (18–29, 30–39, 40–49, 50+ years old), HIV transmission risk (homosexual contact, heterosexual contact, intravenous drug use or mother-to-child transmission), sexual preference (homosexual or heterosexual), origin (Belgium, sub-Saharan Africa, other), health insurance, chronic hepatitis B or C (defined as hepatitis B surface antigen and hepatitis C antibody positive, respectively). We also included the type of first HAART regimen: NRTI (nucleoside reverse transcriptase inhibitors) only, NRTI + PI (protease inhibitor), NRTI + NNRTI (non-nucleoside reverse transcriptase inhibitors) and NRTI + PI + NNRTI. Continuous variables that we examined were: age, time since HIV diagnosis (estimated by date of the first positive HIV test) and duration of follow-up before inclusion.
The Student's unpaired t-test was used to calculate the association between the LTFU and the continuous risk factors. Odds ratios (OR) for the univariate analysis of categorical variables were calculated using a logistic regression model. Variables found to be significant in univariate analysis (P ≤ 0.05) were included in a multivariate logistic regression model. The model was reduced using backward elimination of non-significant variables, and the final model included those variables with P values of less than 0.05. The one-way analysis of variance test was used to compare the average time on HAART treatment and the average time in follow-up for the different calendar years. We also describe the characteristics of patients LTFU at their last follow-up visit: their last viral load (VL; detectable, defined as >50 copies/mL; or undetectable), last CD4 count (< or ≥400/μL) and their last HAART regimen.
SPSS® for Mac v16 (SPSS Inc, Chicago, IL, USA) was used for the statistical analysis. Ethical clearance for the study was obtained from the ITM institutional review board.
RESULTS
Population characteristics
Between 30 June 1999 and 30 June 2009, 2508 patients with HIV infection were in care at the ITM outpatient clinic. One thousand one hundred and one (44%) patients were excluded from the study: 276 (11%) because they did not consult twice within one year and 825 (33%) because they were not on HAART. One thousand four hundred and seven (56%) patients with a total of 38,070 consultations were included in the study. The median number of consultations was 25 (range 2–136). The median time between two consultations was 75 days (range: same day to almost 6 years).
The characteristics of both excluded and included patients are shown in Table 1. Of the patients included in the study, 376 (25%) did not present for a follow-up visit for at least one year. Of these, two patients (0.6%) died and 16 patients (4.5%) went to another hospital. These 18 patients were not considered LTFU. For 358 (94.9%) patients, no follow-up information was available (Figure 1).
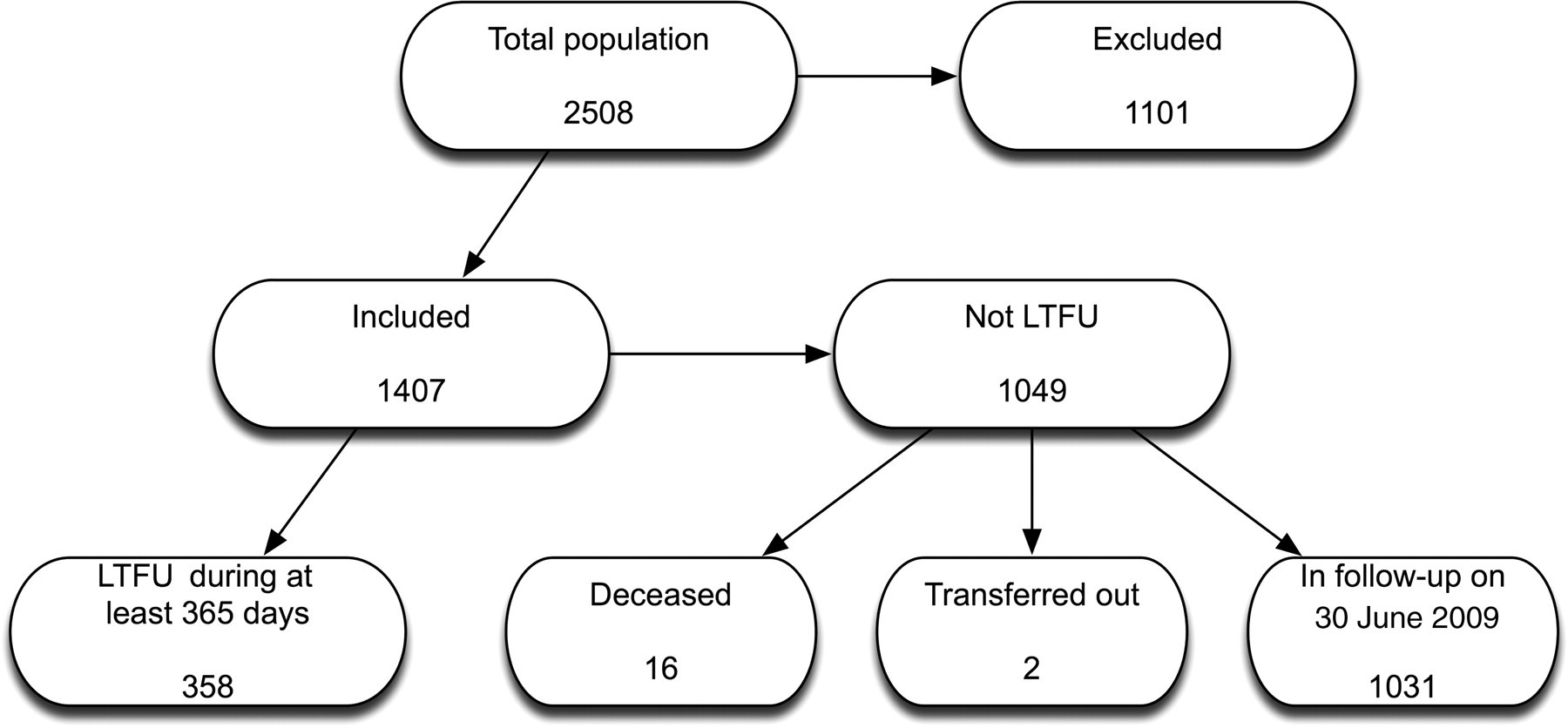
Structure of the study population. LTFU = lost to follow-up
Characteristics of the clinic population and study population
IQR= interquartile range; LTFU = loss to follow-up; HAART, highly active antiretroviral therapy; NRTI= nucleoside reverse transcriptase inhibitors; NNRTI = non-nucleoside reverse transcriptase inhibitors
The average LTFU rate for the entire included population was 5.5% over the nine years of the study. This rate varies over the different years, with a minimum of 2.5% and a maximum of 6.4%, in the years 2008 and 2004, respectively. LTFU proportions remained stable over the years; only the number of patients LTFU in 2008 was low because our analysis stopped at 30 June 2009, thereby not including patients LTFU in the second half of 2009 (Table 2).
Patients LTFU per year (between 6 June 1999 and 6 June 2009)
LTFU = lost to follow-up
*During half a year
The duration of seropositivity before LTFU was on average 10 years. The duration of HAART before LTFU was on average 3.5 years.
Factors associated with LTFU
Patients more likely to become LTFU were started on a PI-containing HAART regimen, were not covered by health insurance, were injecting drug users (IDUs), and lived outside the province where the outpatient clinic is located (Table 3), compared with patients remaining in care.
Baseline risk factors for LTFU in univariate and multivariate analysis
LTFU = lost to follow-up; OR = odds ratio; CI = confidence interval; HAART = highly active antiretroviral therapy; NRTI = nucleoside reverse transcriptase inhibitors; NNRTI = non-nucleoside reverse transcriptase inhibitors; IDU = injecting drug user; PI = protease inhibitor
Age was a significant risk factor in univariate analysis (per 10-year increment: OR 1.12; 95% confidence interval [CI] 1.00–1.25; P = 0.05). In the multivariate model, increasing age was also associated with increased LTFU. Patients in the age group 30–39 years were 56% more likely to be LTFU compared with the reference group (18–29 years), although this was not statistically significant (OR 1.56; 95% CI 0.84–2.90; P = 0.16), but patients aged between 40–49 years were about twice (OR 2.21; 95% CI 1.22–4.02; P = 0.01) as likely to be LTFU. Region of origin, gender, duration of first HAART regimen and language spoken were not significantly associated with LTFU. Patients LTFU frequently disappeared with a detectable VL (45.5%) and with a CD4 count <400/μL (53.9%).
DISCUSSION
The mean LTFU proportion in our cohort was 5.5%. This remained stable over the study period. In a recent report from a large European cohort (EuroSIDA) the LTFU rate ranged from 0.67 to 13.35/100 patient years between the different participating centres.
Baseline characteristics associated with LTFU in our study were: injecting drug use, lack of health insurance, living far away from the clinic, older age and a PI-containing HAART regimen. PI regimens, certainly those containing the first-generation PIs, contained many more pills and often larger ones than other regimens. Those PIs were generally also associated with more side-effects. This might have contributed to poorer adherence and more LTFU. Alternatively, PIs are more often prescribed to patients considered at risk of non-adherence.
The effect of age on LTFU is not straightforward. Increasing age was associated with increased LTFU, and the results suggest a non-linearity of the association. In previous studies, both younger 11 and older age 3,12 have been associated with increased risk of LTFU. The reason why higher age is associated with higher risk of LTFU in our study is unclear. It is certainly a matter of concern as HIV-positive patients are all growing older and further research on this subject is therefore needed.
Baseline characteristics associated with LTFU observed in our study such as lack of health insurance, living far away from the clinic, older age and complex HAART regimens were also identified in most other studies. 2,3,5,8,12,13 Region of origin was not associated with LTFU in our analysis, in contrast with several other studies. 8,11,14 In our clinic however, migrants are targeted for reinforced counselling and receive special attention to retain them in follow-up. All physicians in our clinic also speak several languages, and are able to help most patients in their respective mother tongue.
Differences between risk factors noted in our cohort and in other cohorts are most likely due to differences in clinic populations. The lack of a clear and uniform definition of LTFU makes comparing different studies a challenge. 4 Our study was done in a resource-rich setting; other investigators have performed similar studies in low resource settings. In most countries with limited resources, patients receive their medication in the hospital/clinic, and are considered LTFU after three or four months of absence. In Belgium, patients can get their prescriptions for antiretroviral treatment from a general practitioner or from any other doctor and thus do not need to visit the ITM outpatient clinic very frequently. For this reason, we have set the LTFU threshold at one year.
A study in Malawi found 50% of their patients LTFU to be dead, and only a small minority still took their pills after four months of absence. 15 The situation in Malawi is very different from our setting. Financial problems are a major obstacle for retention in care in sub-Saharan Africa. In Belgium most of the HIV care is provided free, and patients generally have more financial resources. 14
A limitation of our study is the lack of access to reliable vital statistics, for example through national health registers or databases. We also did not have a system in place to trace patients LTFU. Therefore, for most of our patients we did not know why they were LTFU (whether they were followed up in another clinic, or even country, whether they were still on treatment or whether they died). We also included only those patients who were on HAART, because for patients not yet on HAART, at ITM, there is no standardized way follow-up visits are planned.
The fact that around 50% of all patients LTFU disappeared with a detectable VL and a CD4 count <400/μL increases the risk of them transmitting HIV, including potentially resistant viruses, in the community.
To decrease LTFU proportions several options should be considered. Firstly, it is necessary to collect as many personal data as possible (e.g. land line and/or mobile phone number, address, email, etc.). 16 It is also important to collect personal data from a family member or a friend. 17 Reminder calls before appointments and phone calls by peer educators after missed appointments may be very useful. 18
CONCLUSION
It is of great importance to identify patients at risk for LTFU, to provide them with extra counselling and to emphasize the importance of retention in care, particularly after the start of HAART. 3 Strategies to prevent LTFU should be a major component in effective HIV/AIDS treatment plans and HIV treatment centres should establish systems to trace patients LTFU.