
Abstract
The aetiology of chronic prostatitis is poorly understood. A cross-sectional study of a population of male undergraduates in Nigeria, using a questionnaire containing the National Institutes of Health Chronic Prostatitis Symptom Index (NIH-CPSI) and some other relevant sex-related questions, was conducted. A total of 14.9% of the population had chronic prostatitis symptoms (CPSs) defined as a pain score of four or more on the NIH-CPSI pain subscale. Approximately 26 or 12% of the population had at least one, or ≥ 2 location(s) of pain, respectively. The presence of CPS was found to correlate with a self-reported history of sexually transmitted infection (STI) (r = +0.237; P < 0.05) and 73% of those with a self-reported history of STI had CPS. Both voiding scores and quality-of-life scores were significantly higher in subjects with CPS, compared with those without CPS. Self-reported history of STI may be an important aetiological factor for chronic prostatitis/chronic pelvic pain symptoms.
INTRODUCTION
Prostatitis is a common debilitating urological disease that is characterized by inflammation of the prostate gland. It has long been estimated that up to half of all men suffer from symptoms of prostatitis at some time in their lives. 1 More recently, prostatitis has been reported to be the most common urological diagnosis in men younger than 50 years and the third most common urological diagnosis in men over 50 years. 2,3 There are four categories of prostatitis according to the National Institutes of Health (NIH) classification, designated I–IV (Table 1). Chronic prostatitis/chronic pelvic pain syndrome (CP/CPPS) (NIH category III) is usually characterized by persistent perineal pain and by functional and somatic urological complaints, including abnormal urine flow, frequency and dysuria. 4 The NIH-Chronic Prostatitis Symptom Index (NIH-CPSI) is an instrument that is widely used to assess the severity of symptoms of CP/CPPS. 5
Classification of prostatitis
NIH = National Institutes of Health; NA = not applicable; EPS = expressed prostatic secretion
*Reference 30 suggests it could be YES
†EPS may not be collected as prostatic massage is contraindicated
The aetiology of CP/CPPS is poorly understood and an infective basis for it has not been identified, and yet its symptoms are bothersome. 5 Treatments for CP/CPPS are based on consensus opinion rather than on scientific data 6 and usually involve the use of antimicrobials, although response to such treatments is generally poor. However, some studies in the literature have implicated microorganisms as causative agents of CP/CPPS, including Chlamydia trachomatis, 7 Mycoplasma genitalium, 8 Staphylococcus epidermidis, 9 Staphylococcus haemolyticus, 10 Corynebacterium seminale 11 and many other coryneform (and other) bacteria. 12,13 The association of these organisms with CP/CPPS implies that there might be a relationship between sexually transmitted infections (STIs) and CP/CPPS. This study therefore surveys the prevalence of chronic prostatitis symptoms (CPS) in a population of undergraduates in a Nigerian university, and explores the differences in self-reported history of STI (and some sex-related factors) between subjects with and without CPS.
SUBJECTS AND METHODS
Male undergraduate students of Michael Okpara University of Agriculture, Umudike (MOUAU), Nigeria (age range: 17–30 years) participated in the study. A total of 2500 copies of a questionnaire containing the NIH-CPSI, and additional questions that sought information on the respondents' age, age at first sexual exposure, number of current sexual partners, frequency of ejaculation and history of STI, were distributed randomly to the students. Only those who gave an informed verbal consent were allowed to participate in the study, which lasted from April to June 2010. The study design was approved by, and ethical clearance obtained from, the Board of the Department of Biochemistry, MOUAU, Nigeria.
Respondents were separated into two groups based on scores from the pain domain. Those with a total pain score (0–21) of four or more were identified as having CPS, while those who had a pain score of zero to three were identified as not having CPS. Respondents with a voiding score (0–10) of two or more were classified as having voiding problems, while those whose voiding scores were less than two were identified as not having voiding problems. Based on their quality-of-life (QOL) scores, respondents who had a score (0–12) of three or more were identified as having poor QOL, while those with a QOL score of zero to two were identified as having good QOL.
Self-reported age (at last birthday) was recorded for each respondent. Means and percentages of the outcome measures (where necessary) were calculated. Differences between means for parametric data were separated by one-way analysis of variance, while those for non-parametric data were checked for significance using the chi-square test. Pearson's product moment correlation coefficients were calculated to assess the relationship between the presence of CPS and variables such as age at first sexual exposure, number of partners, ejaculation frequency and self-reported history of STI. A significant threshold of P ≤ 0.05 was employed for all analyses. Data analyses were performed using SPSS for windows version 17.0 (SPSS Inc, Chicago, IL, USA).
RESULTS
The 2500 questionnaires distributed targeted 80% of the male undergraduate population of MOUAU. Of the 2500 questionnaires, 2217 (87%) were recovered. A total of 214 recovered questionnaires were invalidated due to incomplete or multiple entries. Two thousand and three recovered questionnaires, representing 90% of recovered questionnaires and 80% of distributed ones, were effectively analysed.
Two hundred and ninety-eight subjects (14.9% of the population) had CPS. A total of 524 respondents (26.2% of the population) had at least one location of pain, while 11.8% of the population (237 subjects) had two or more locations of pain. The presence of CPS was found to correlate positively and significantly with a self-reported history of STI (r = +0.237; P < 0.05), but not with the other factors. Respondents with and without CPS had similar (P > 0.05) average age. Expectedly, subjects with CPS had significantly (P < 0.001) higher mean pain scores than their counterparts without CPS. Those with CPS also had significantly (P < 0.001) higher mean voiding scores and significantly (P < 0.05) higher mean QOL scores than those without CPS. Age at first sexual exposure and number of current sexual partners were each similar (P > 0.05) between the two CPS groups (Figure 1).
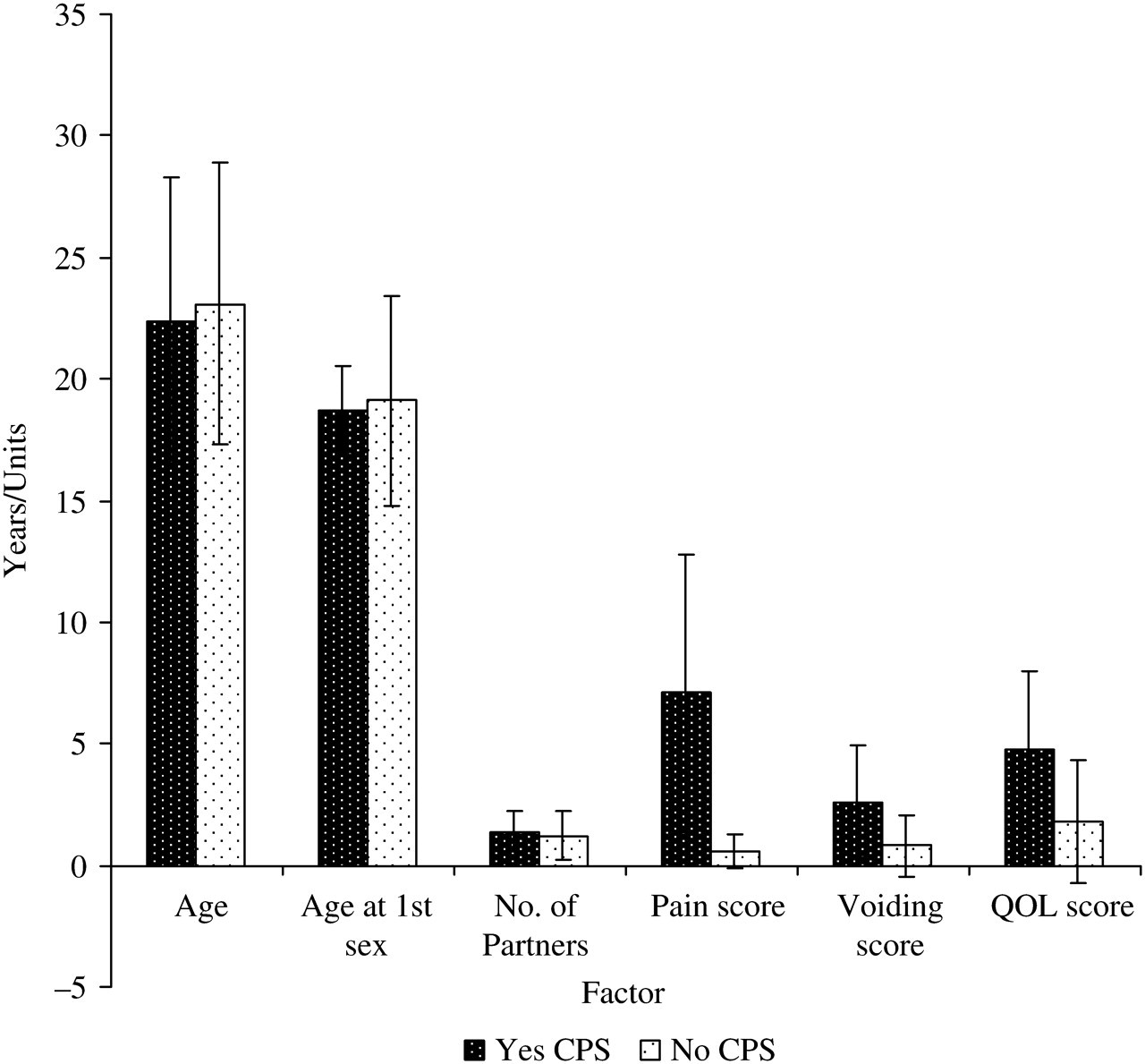
Variables of interest and outcome measures of the population in men with and without CPS. CPS = chronic prostatitis symptoms; QOL = quality of life
A total of 62.4% of those with CPS had voiding problems, while only 15.6% of their counterparts without CPS had voiding problems. Again, 69.1% of subjects with CPS had poor QOL, as against 23.7% of those without the symptoms who had poor QOL. Interestingly, approximately 31% of those with CPS had a self-reported history of STI (that is, 73% of all those with a self-reported history of STI had CPS). Contrastingly, only 2% of those without CPS had a self-reported history of STI. These differences (for each of the three factors above) were all significant (P < 0.05). Approximately 84% of subjects with CPS were sexually exposed, while 76.5% of their counterparts without CPS were sexually exposed. A total of 58.7% and 72.2% of those with and without CPS, respectively, had an ejaculation frequency of more than two ejaculations per month. The differences (for sexual exposure and ejaculation frequency) were, however, not significant (P > 0.05 in each case) (Table 2).
Proportions of the population with and without chronic prostatitis symptoms stratified according to some outcome measures
CPS = chronic prostatitis symptoms; STI = sexually transmitted infection; QOL = quality of life
DISCUSSION
Chronic prostatitis is hypothesized to be initiated by an event such as an infection, trauma or STI. 14 Although an infective basis is yet to be scientifically established, the finding of microorganisms in prostatic tissues and secretions 7–13 appears to lend credence to the implication of microorganisms (many of which are known to cause STIs) as aetiological factors in chronic prostatitis. This study further supports the existence of a relationship between CP/CPPS and STIs by showing a positive correlation between a self-reported history of STI and CPS. The finding that 73% of all those with a self-reported history of STI also had CPS is informative. This relationship between CP/CPPS and STI may in part explain the reason for a higher prevalence of CPS among younger men, compared with the elderly.
The 14.9% prevalence of CPS reported in this study is particularly high. Collins et al. 15 had reported that the prevalence of prostatitis in the general population is estimated to be 5.0–14.2% depending on the definition of prostatitis, study subjects and methodology. An earlier study in a different state in Nigeria, using the NIH-CPSI, found CPS prevalence to be 12.2% in the general population, but 11.9% in a subset of the population aged 20–29 years, 16 while a study of Canadian adolescents aged 16–19 years (using the same instrument) reported a CPS prevalence rate of 8.3%. 17 A total of 9.1% of those aged 20–29 years in the earlier study from Nigeria had two or more locations of pain, 16 as against the 11.8% reported in the present study. Clearly, the present figures are largely higher than those from the mentioned study from Nigeria. However, the 26.2% of this population found to have pain in at least one area is close to the 27.8% reported earlier from Nigeria, 16 but is about four-fold higher than the 6% reported for a population of young men by Ku et al. 18 The prevalence data for chronic prostatitis from earlier studies show 14.2% in Finland, 2 12.8% in Italy, 19 10.5% in Montreal, Canada, 20 9.7% in Lennox and Addington counties, Canada, 3 8.7% in Penang, Malaysia, 21 8.4% in China, 22 6.3% in Boston, USA, 23 5.9% in Portland, USA, 24 4.9% in Hokkaido, Japan, 25 2.7% in Singapore, 14 2.7% in Vienna 26 and 2.2% in Olmsted county, Minnesota, USA. 27 Although differences in sample size and characteristics as well as methodology make it difficult to compare these figures, it is clear that the rates from Nigeria are high. Genetic and environmental differences may be responsible for the observed variations in prevalence data for chronic prostatitis.
This study further shows that about 69% of those with CPS had poor QOL as against the roughly 24% of those without CPS who also had a poor QOL. Earlier reports had shown that any form of prostatitis reduces QOL for the sufferer. 16,28 The observation that subjects with CPS had significantly higher voiding scores and QOL scores compared with those without CPS is also in consonance with an earlier report. 16 The observation that age at first sexual exposure and number of current sexual partners were similar between those with CPS and those without CPS may suggest that high-risk sexual behaviour may be central to increasing the risk of CPS. The lower ejaculation frequency found in those with CPS, compared with their counterparts without CPS may be related to the urogenital pains that are typical of CP/CPPS such that the sufferer may often avoid sexual intercourse. The fact that the difference in ejaculation frequency between the two CPS groups was not statistically significant suggests that ejaculation frequency may not have a significant role in the pathogenesis of CP/CPPS.
This study is limited by a number of factors. Firstly, the NIH-CPSI was used to detect the symptoms of CP/CPPS in this cross-sectional survey, such that the other classes of prostatitis were not excluded. Secondly, self-reported history of STI rather than direct laboratory or medical records' evidence of current or historical STI was relied on in this study. Krieger et al. 29 had reported that specific polymerase chain reaction assays detected M. genitalium, C. trachomatis or T. vaginalis in prostate tissue from only 8% of a population of 135 men with chronic idiopathic prostatitis as against 30.9% of those with CPS who also had a self-reported history of STI in this study. However, Nickel et al. 30 reported that ‘localization of uropathogenic bacteria in EPS, VB3 and/or semen was similar in men with CP/CPPS (8.0%) and asymptomatic men (8.3%)’. A cautious interpretation of the data presented here is therefore warranted.
In conclusion, 14.9% of a population of undergraduate students in a Nigerian University had CPS. A total of 30.9% and 69.1% of these people (with CPS) reported a history of STI and poor QOL, respectively. Self-reported history of STI but not age at first sexual exposure, ejaculation frequency or number of current sexual partners was positively correlated with CPS. Efforts targeted at enlightening men with prostatitis and its probable relationship with STI, and therefore the need for safer sexual practices, is warranted.
Footnotes
ACKNOWLEDGEMENTS
The author wishes to thank all the volunteers who participated in the training for, and subsequent distribution of, the questionnaires to the respondents, and the respondents who graciously completed the questionnaires.