
Abstract
Australian and New South Wales Sexually Transmissible Infections Strategies recommend sexual health clinics actively target particular populations, including men who have sex with men (MSM), who have increasing rates of sexually transmitted infections (STIs). We describe trends in MSM attendances, STI testing and diagnostic yield from 1996 to 2007 at a Sydney public sexual clinic. Aggregate data were extracted from the clinic database. There was a 76% increase in the number of individual MSM attending, more than three-fold increase in the number of STI tests performed and the proportion of MSM tested. The increase in testing was greatest for rectal infections. The positive yield increased for rectal chlamydia and infectious syphilis; remained stable for pharyngeal gonorrhoea; and decreased for urethral gonorrhoea, rectal gonorrhoea and urethral chlamydia. Our results demonstrate successful service reorientation in response to a local STI epidemic. Differing trends suggest evolving transmission dynamics for different STIs in the context of increased testing of asymptomatic MSM.
Introduction
Australian and New South Wales (NSW) Sexually Transmissible Infections Strategies recognize that sexually transmitted infections (STIs) disproportionately affect some population groups, including men who have sex with men (MSM), and that sexual health services should be oriented towards these groups.1,2 In response to the increasing rates of STIs other than HIV in MSM in inner Sydney, STI testing guidelines were developed in 2000–2001. 3 These guidelines were implemented by the Sydney Sexual Health Centre (SSHC) in 2001, and a subsequent increase in MSM STI testing rates was demonstrated. 4 Concurrently, SSHC and local MSM and HIV community organizations encouraged increased clinic attendance by MSM. Local surveillance data continue to show rising notification rates for gonorrhoea, chlamydia and infectious syphilis. 5 The relative contributions to this rise from increased STI incidence or increased STI testing are unclear because most notifiable STIs are diagnosed in general practice where detailed testing information is not routinely collected. We describe changes in attendance and STI testing practices among MSM, and the anatomical site-specific yield of diagnostic tests over a 12-year period at the SSHC, a public sexual health service in inner Sydney.
Method
SSHC maintains a database of behavioural, symptom, testing and diagnostic information for all patients. Every year during 1996–2007 the following variables were extracted: number of attendances by MSM; number of asymptomatic MSM having bacterial STI tests; numbers of urethral gonorrhoea and chlamydia, rectal gonorrhoea and chlamydia, pharyngeal gonorrhoea and syphilis tests performed in MSM; and the number of diagnoses (late latent syphilis was excluded). Over the study period, the clinic used Roche Amplicor® polymerase chain reaction (PCR) for chlamydia and asymptomatic urethral gonorrhoea infections, and gonococcal culture for all other gonorrhoea testing. Until May 2000, syphilis was tested using Treponema pallidum particle agglutination and rapid plasma reagin, and thereafter a T. pallidum antibody enzyme immunoassay was used. Chi-square test for trend was used to determined trends in the positive yield of testing, and the proportion of MSM tested for STIs, over the period 1996–2007. The South Eastern Sydney Illawarra Area Health Service human research ethics committee granted ethical approval.
Results
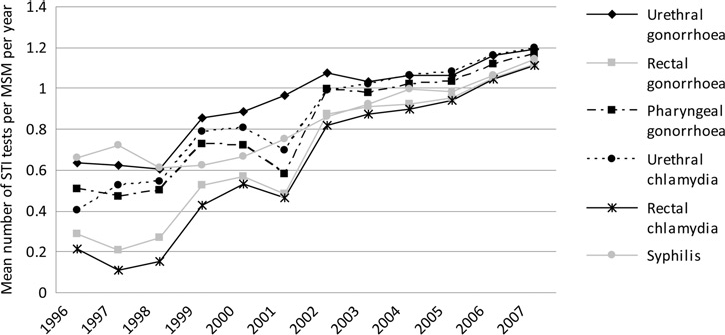
There was a 76% increase in the annual number of individual MSM attending during the period 1996–2007 from 1350 to 2376 men. The number of STI tests performed increased markedly (Figure 1) with the greatest being a five-fold increase in testing for rectal infections. The mean number of tests per individual MSM attending the clinic increased markedly for all infections (Figure 2). Approximately two-thirds of attendances by MSM were for asymptomatic STI testing for which no significant trend in this proportion was detected (data not shown).
Number of sexually transmitted infection (STI) tests performed among men who have sex with men, 1996–2007 Mean number of sexually transmitted infection (STI) tests per individual among men who have sex with men (MSM), 1996-2007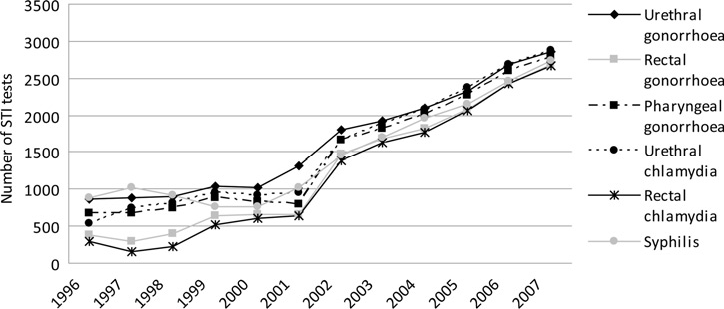
Following this increase in testing there was a corresponding rise in the number of bacterial STIs detected from 93 in 1996 to 475 in 2007; however, trends in the positive yield were variable by infection and anatomical site (Figure 3). The positive yield increased for syphilis and rectal chlamydia, and decreased significantly for urethral and rectal gonorrhoea and urethral chlamydia. The yield remained constant for pharyngeal gonorrhoea.
Positive yield (%) of sexually transmitted infection (STI) tests performed among men who have sex with men (MSM), 1996-2007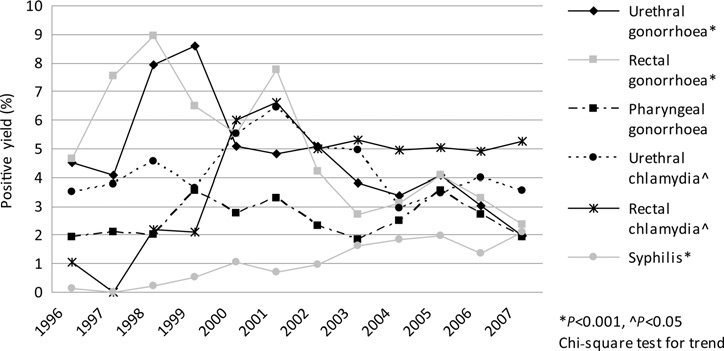
Discussion
Our results demonstrate the successful reorientation of a sexual health clinic in response to a local STI epidemic. Over the 12 years of the study both the number of attendances by MSM, and the proportion who were tested, have shown large increases. This increase in clinical services has been achieved without increasing the total budget through improved targeting of the service to local priority populations, reflecting the Australian and NSW Sexually Transmissible Infections Strategies.1,2
The trend in positive yield decreased for infections that are more often symptomatic – urethral and rectal gonorrhoea and urethral chlamydia – and either increased or remained flat for those that are usually asymptomatic - rectal chlamydia and pharyngeal gonorrhoea. Increased asymptomatic screening could account for these differing trends, as symptomatic infections would have been more likely to be detected even with a low testing rate.
Although the trends in positive yield varied between STIs, overall it remained relatively constant in the last half of the study period (Figure 2), despite the large increase in the number of STI tests performed. This continuing high positive yield from testing strongly supports the need for widespread STI testing of MSM, in particular for rectal infections. Rectal infections showed the highest yield in our study, consistent with local community-based cohorts of MSM, where rectal infections were strongly associated with practices in addition to anal intercourse. 6 Similar data from MSM attending clinics in the USA also found a relatively constant yield of rectal infections. 7 These data support the assertion that much of the increased notification rate of STIs among MSM is due to increased screening.
The increase in testing among MSM attending our clinic appears to have had limited impact on the prevalence of STIs in our patients to date. Modelling data suggest that to achieve a significant reduction in the population prevalence of syphilis among MSM, multipartnered MSM may need to be tested at least two to three times per year. 8 Although the number of MSM attending our clinic has increased, it only represents approximately 24% of the total estimated number of MSM living in the region serviced by the clinic. 9 Sydney MSM are reporting more comprehensive annual STI testing in community-based surveys, 10 but they are not being screened for STIs as frequently as recommended in general practice settings. 11 Infrequent presentation for testing and missed opportunities during other types of consultations may explain the low testing within primary care. Further increases in the uptake of testing will require mobilization of the gay community and along with other parts of the health system, particularly general practitioners.
The use of aggregate data has some limitations. As we examined crude testing rates and yield, it is possible that a smaller group of MSM were tested more frequently with some MSM tested less frequently. In addition, as the reason for testing in each individual is unknown and the overall proportion of MSM tested for STIs who were asymptomatic in each year remained constant over the period, we cannot be certain that the increase in testing overall was due to asymptomatic screening or an increasing number of presentations with symptomatic STIs. However, as the largest increase in testing was noted in rectal infections, which are generally asymptomatic, 6 it appears most likely that asymptomatic screening accounted for the bulk of the increase in testing. Finally, our data relate to men attending a single sexual health clinic and may not be generalizable to other populations.
Our findings demonstrate the successful reorientation of a sexual health service to increase STI testing of MSM. This reorientation has been associated with an increase in the total number of STIs diagnosed and treated at the clinic. The positive yield remained high, supporting the need to continue targeted testing of MSM.