
Abstract
The expanding services of antiretroviral treatment (ART) in sub-Saharan Africa provide unique opportunities to reduce HIV/AIDS-related morbidity and mortality. In these settings, HIV prevalence among antenatal women remains high and treating eligible pregnant or breastfeeding women with antiretrovirals can substantially reduce transmission of HIV from the mother to her infant. However, identification of women eligible for treatment and ensuring access to ART services is challenging. In this analysis, we used data from a large clinical trial (the PEPI-Malawi study, 2004–09) to prevent mother-to-child transmission of HIV through extended antiretroviral prophylaxis of infants to examine barriers for wider coverage with highly active antiretroviral treatment (HAART) of postpartum women. Maternal HAART was not part of the original PEPI-Malawi clinical trial but became available through a government programme during the course of the study. Therefore, eligible women (CD4 cell count <250) who participated in the PEPI-Malawi trial were counselled and referred to the government ART clinics to initiate HAART. Of 3335 women who enrolled in the PEPI-Malawi study, 803 (24%) were eligible for HAART based on CD4 cell count. The proportion of women newly initiating HAART at the ART clinic remained low and constant (<20%) throughout the study period. However, the cumulative proportion of women receiving HAART increased substantially over time (29% in 2005 to 69% in 2009). Similarly, counselling and referral of eligible women substantially increased and became 100% during the last two years. There were no statistically significant differences in characteristics of eligible women who received or did not receive HAART postpartum. Despite limitations of not being able to obtain detailed data, the main barriers appeared to be related to the health-care system delivery of ART services. Issues of physical space, more personnel and better delivery need to be addressed to increase access to HAART in these settings.
Keywords
INTRODUCTION
Many clinical trials as well as observational data have demonstrated the benefit of highly active antiretroviral treatment (HAART) for eligible individuals infected with HIV-1. 1–3 In developed countries HAART is recommended for all pregnant HIV-infected women regardless of the CD4 cell count, starting from at least 28 weeks of pregnancy. In these settings, women do not breastfeed postpartum.
In resource-limited settings, prevention of mother-to-child transmission (PMTCT) of HIV services revolves around the use of short-course antiretroviral regimens during labour to the mother and to the infant immediately following the birth. Before the 2009 WHO recommendations, 4 mothers in these settings were encouraged to exclusively breastfeed their infants for at least six months and thereafter wean them if replacement feeding was acceptable, feasible, affordable, safe and sustainable. 5 Exclusive breastfeeding had been shown to reduce HIV transmission through breast milk compared with mixed feeding. 6,7
In resource-limited settings, potential prevention strategies to reduce breastfeeding-associated HIV transmission include the provision of extended antiretroviral infant prophylaxis, 8 or the provision of HAART to lactating women or provision of both. The treatment of pregnant and breastfeeding women who are eligible for HAART is vital to reducing mother-to-child transmission (MTCT), 9 and in reducing morbidity and mortality among the women themselves and their children. 10,11 Ensuring access to HAART for pregnant and lactating women not only contributes to better child survival but also promotes overall health. A study in Uganda observed 81% reduction in mortality among uninfected children younger than 10 years and 93% estimated reduction in orphan-hood, over a 31-month period if their HIV-infected parents were receiving HAART and cotrimoxazole preventive therapy. 12
However, despite recent increases in the frequency of access to PMTCT services, many pregnant HIV-infected women in resource-limited settings have no access to HAART for their own health in a timely manner for a variety of reasons. Data reported by governments indicate that only about 12% of pregnant women living with HIV identified during antenatal care were assessed for their eligibility to receive HAART in 2007 based on an assessment of clinical symptoms, or by measuring their CD4 cell counts. 13 In Malawi, where HIV prevalence among women of reproductive age is ∼14%, 14 access to HAART among pregnant women living with HIV remains low. UNICEF 15 reports that in Malawi most children were infected through MTCT, which accounts for close to 30,000 of infections among newborns every year and only 24% of HIV-positive pregnant women attending antenatal clinics are receiving antiretroviral prophylaxis to prevent transmission of HIV to their baby. Among 9150 women who started HAART in the last quarter of 2007 in the public sector, only 343 (4%) had been referred from the PMTCT programme. 16
A randomized, controlled phase III trial of extended postexposure prophylactic antiretrovirals in infants (PEPI-Malawi) was conducted in Blantyre, Malawi, to prevent HIV transmission through breastfeeding. 8 Maternal HAART was not part of the PEPI-Malawi trial but was introduced as part of the government antiretroviral clinical care service during the conduct of the trial for women eligible for treatment. Most women who received HAART in the PEPI-Malawi study received treatment after 14 weeks postpartum (∼3% before 14 weeks and ∼12% after 14 weeks). 8 In this analysis, we examine barriers to HAART coverage among postpartum women who participated in the PEPI study. These women were eligible for treatment, counselled and referred to the antiretroviral clinic.
METHODS
This is a secondary analysis of data originally collected from a clinical trial, the PEPI-Malawi study, conducted at the Queen Elizabeth Central Hospital (QECH) and five health centres in Blantyre, Malawi. The PEPI-Malawi trial started in April 2004 and completed follow-up in September 2009. The details of the clinical trial were described elsewhere. 8 In brief, pregnant women who presented for either antenatal or delivery services at the study clinics in Blantyre, Malawi, were offered HIV-1 counselling and testing. All women with known HIV infection before onset of labour received intrapartum single-dose nevirapine (NVP). Women could be enrolled in the trial if they fulfilled the following criteria: HIV infected, at least 18 years of age, pregnant or had given birth within the previous 24 hours at one of the study clinics, resident of the study area, willing to return for postnatal follow-up visits for up to two years, and intended to breastfeed. Women returned for follow-up visits every three months for two years.
At each visit, blood was drawn for complete blood count and CD4 cell count (at enrolment, 14 weeks, and 12, 18 and 24 months). Women with CD4 counts less than 250 cells per mm3, defined as HAART-eligible women, were referred to the local antiretroviral clinic at QECH to access HAART. HAART was provided free to all patients. In Malawi, the first-line antiretroviral treatment (ART) regimen is NVP plus stavudine and lamivudine in a fixed dose combination. Women having stavudine or NVP toxicity are switched to zidovudine (ZDV) and efavirenz, respectively.
Women reported to the study site alone with their babies. Information on counselling, referral and use of HAART was collected on structured case report forms at each visit. Structured interviews were administered by nurse counsellors to participating women, alone, in the local language. Other sociodemographic, clinical and laboratory data were collected as part of the clinical trial at baseline (enrolment) and follow-up visits.
For data analysis, we calculated the proportion of women who were counselled, referred and used HAART postpartum (overall and newly receiving HAART) among eligible women who returned for follow-up visits. We plotted trends in the use of HAART by calendar time. To assess the underlying factors limiting access to HAART, we performed comparisons of sociodemographic factors for those who were counselled, referred and received HAART (overall) versus those who were counselled and referred but did not receive HAART. We used chi-square and t-tests to compare categorical and continuous variables, respectively. A P value of <0.05 was considered statistically significant. The variables of interest included maternal age, parity, marital status, education, body mass index (BMI), lifetime number of partners, formal employment status, presentation at delivery (early versus late; early: arrival to the labour ward ≥4 hours prior to delivery; late: arrival to the labour ward <4 hours prior to delivery), partner's education, availability of electricity/water in the house and infant HIV infection status at 14 weeks of age. We used logistic regression analysis to assess the association of the sociodemographic factors with use of HAART postpartum. The multivariable logistic regression model included variables with P value <1.0 in the univariable model and variables epidemiologically or biologically considered important. Odds ratios (ORs) and 95% confidence intervals (CIs) are presented.
The PEPI-Malawi protocol and study consent forms were approved by institutional review boards at the College of Medicine, University of Malawi in Blantyre, Malawi, and the Bloomberg School of Public Health, Johns Hopkins University, Baltimore, MD, USA.
RESULTS
Overall, 3335 women were enrolled in the PEPI study. Of these, 803 (24%) were eligible for HAART based on CD4 cell count (<250 cells per mm3) and 2532 were not eligible for HAART postpartum. Figure 1 shows the quarterly frequency of women who were counselled, referred and received HAART during the period 2005–09. The proportion of women counselled and referred for HAART initiation increased from 89% in July 2005 to 100% in 2009. The proportion of women in the study newly initiating HAART at the ART clinic remained low and was approximately constant each quarter during the study period or showed a trend of decline over time; area A – Figure 1. The overall proportion of women who initiated and continued on HAART increased over time from 29% in 2005 to 69% in 2009; area B – Figure 1.
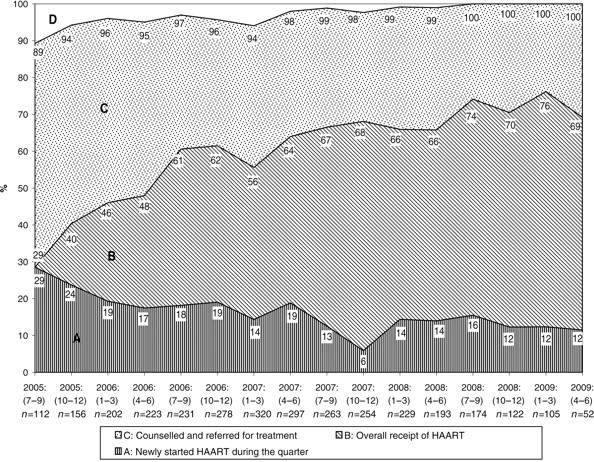
Quarterly proportion (%) of HAART eligible women counselled, referred and treated, Blantyre, Malawi, 2005–09. HAART = highly active antiretroviral treatment
A comparison of the sociodemographic characteristics of women who were either eligible or not eligible for HAART in the PEPI-Malawi cohort is shown in Table 1. Women eligible for HAART, compared with those not eligible, were significantly (P < 0.05) older, had higher parity, lower BMI, more lifetime number of sexual partners, fewer presented early at time of delivery, more were formally employed and more had children HIV infected at 14 weeks of age.
Comparison of characteristics of HAART eligible and non-eligible women in the PEPI study, Blantyre, Malawi
HAART = highly active antiretroviral treatment; BMI = body mass index
*Baseline data if not indicated otherwise
By the end of the study, among the 803 women who were HAART eligible, counselled and referred, 513 (64%) received HAART and 290 (36%) did not receive HAART. We were able to ascertain the reasons for not receiving HAART in 235 (∼81%) women. These reasons included unwillingness of the woman herself (25.5%), terminations from the study and death while waiting to initiate HAART (19.0%), missing a follow-up visit after being referred to the HAART clinic (15.5%), no guardian available (12.4%) and other reasons related to the waiting period to initiate therapy (9%). In ∼19% the reason why the woman did not start therapy was not available. Table 2 shows the sociodemographic characteristics of the women who received HAART compared with those who did not receive HAART. With the exception of age and parity, where women who received HAART were older and had higher parity, there were no statistically significant differences in other sociodemographic characteristics of women who received or did not receive HAART.
Comparison of characteristics of women who received or did not receive HAART among HAART eligible women (n = 803), Blantyre, Malawi
HAART = highly active antiretroviral treatment; BMI = body mass index
*Baseline data if not indicated otherwise
Table 3 shows the factors associated with the use of HAART among eligible women who were counselled and referred for treatment. Maternal age, parity and marital status were included in the multivariable model because they were statistically significant at P < 1.0. BMI and availability of electricity at the house were included because they are important biological (BMI) or socioeconomic (having electricity) indicators. After simultaneously adjusting for these factors, none of these variables were significantly associated with HAART use among eligible women. Removing age or parity from the multivariable model to avoid collinearity did not change these results.
Factors associated with use of HAART among women counselled and referred, Blantyre, Malawi
HAART = highly active antiretroviral treatment; CI = confidence interval; BMI = body mass index
*Logistic regression analysis
DISCUSSION
We examined barriers to access ART in a cohort of postpartum women who participated in a clinical trial to prevent MTCT of HIV through breastfeeding in Malawi. Government introduction of HAART in Blantyre while this trial was ongoing allowed these women the opportunity to access HAART. However, as shown in this study, coverage was not universal despite reaching a 100% level of identifying eligible women, counselling and referral to the antiretroviral clinic. Examination of Figure 1 data shows that there have been substantial cumulative increases in number of women who are receiving HAART (an increase of 40%; from 29% to 69%). However, the number of women accessing HAART as new cases remains limited (<20% during a period of approximately 3 years), demonstrating the restricted capacity of the health services to expand and accommodate new patients in addition to continuing follow-up services for women already on therapy.
In this research study, we were able to monitor these postpartum women every three months and perform repeated counselling and laboratory testing. Women eligible for treatment were referred based on the results of these follow-up visits. Nonetheless, the HAART services were in the government clinic and open to the entire adult population. The clinic could therefore accommodate a limited number of clients every week and other logistical factors such as availability of drugs and personnel continuously influenced access. These health system barriers could be considered ‘external’ access factors to differentiate them from ‘internal’ factors inherent to the individual patient. These internal or individual factors could be sociodemographic, including behavioural and enabling factors at the community level. Such conceptual frameworks have been described 17 and could help to understand the various components associated with access in this study.
In the current study, there were no statistically significant differences in the sociodemographic characteristics of women eligible for HAART who ultimately received or did not receive HAART. This suggests that the main barriers in this setting are at the level of health systems (external factors) such as resources and organization. 16 Resource factors include personnel, infrastructure, equipment and materials utilized in providing HAART. Organizational factors include coordination of services and control processes for provision of HAART. In the HAART clinic in Malawi, a number of factors may have contributed. For example, a minimum of three visits are made before an individual can access HAART: the first visit is for counselling and testing for HIV; the second visit is for HAART eligible individuals where they are required to bring a guardian to educate them together about HAART and the third visit is to initiate treatment (Malawi National ART guidelines 2004). In other studies done in Malawi 18 to demonstrate the impact HIV/AIDS has on human resources in an already fragile health system, it has been shown that the Malawi HAART programme used far fewer health professionals than would have been expected based on the estimates from other settings. At the time HAART was commenced at QECH, facility barriers were common as only QECH could provide HAART in that whole district. This facility could only take a maximum of 150 new patients per month coupled with only a handful of trained personnel in HAART provision. Other factors such as distance from the clinic have also been reported as important barriers. 19,20
Introduction of HAART to Malawi was novel and mostly depended on existing infrastructure and capacity. We do not have detailed information about the reasons why women did not initiate HAART after being counselled and referred. Of the limited information we could obtain it appears that the major causes were related to the health-care system, such as long waiting times from referral to initiation of HAART. Refusal and unwillingness of some women to receive treatment may also suggest partner/spouse objection or fear of discrimination and the inability of women to disclose their HIV status. In the Malawi setting, as well as in other sub-Saharan countries, issues of stigma remain important in determining access to HIV care. 17
LIMITATIONS
Our current analysis has limitations because of the operational nature of the study. We did not collect data to evaluate in depth what specific health-care factors affected access to HAART for each woman. Likewise, we did not specifically evaluate adherence and subsequent perceptions after initiation of HAART. Despite these limitations, early analyses of data from women who accessed HAART suggest substantial benefits such as reductions in MTCT of HIV (<2% when eligible women received HAART postpartum) as well as higher child HIV-free survival. 9,10
CONCLUSION
The unmet need for HAART services among breastfeeding HIV-infected women in Malawi is substantial. The frequency of women newly initiating HAART did not increase over time, despite increases in counselling and referral of eligible women. There were no differences in sociodemographic factors of women who received or did not receive HAART among eligible women. The major barriers appear to be associated with structural limitations of the health-care system. Internal individual barriers to access HAART (e.g. partner-consent and discrimination issues) need further detailed evaluation.