
Abstract
Bone infection, particularly of the skull and the long bones of the legs and arms, despite being a common characteristic of tertiary stage syphilis and congenital syphilis in the past, is seldom encountered clinically due to effective antibiotic therapy. We report a case of a 62-year-old man who presented with one-month acute pain in the left leg. Treponema pallidum particle agglutination test was positive, and radiography showed a pathological fracture of the left tibiofibula. Surgical debridement and biopsy of the bone marrow were performed and a pathological diagnosis of syphilis osteomyelitis was entertained. The patient's symptoms resolved completely after a six-week course of penicillin. We identified 17 previously published cases of bone lesions of syphilis, eight of which had syphilitic osteomyelitis, seven were syphilitic osteitis and two had syphilitic periostitis. We suggest that bone lesions such as osteomyelitis caused by syphilis can be the only manifestation of late latent syphilis.
Keywords
Introduction
Syphilis is a sexually transmitted infection (STI) caused by Treponema pallidum (T. pallidum). After a period of decline, there has been a recent resurgence in the number of cases of syphilis reported and approximately 12 million new infections occur annually worldwide. 1 Syphilis, which was nearly eliminated in China about 50 years ago, has staged a precipitous increase in the number of reported syphilis cases in the country over the decade.2,3 Syphilitic osteomyelitis is a recognized but rare manifestation of tertiary syphilis and usually occurs in conjunction with other cutaneous and mucosal lesions. 4 Late latent syphilis occurs when the symptoms of syphilis become manifest between one year after the initial infection and up to 25 to 30 years later. 5 Here, we describe a case in which bone pain was the only presenting feature of syphilis and we also reviewed recent literature reporting bone lesions of osteomyelitis as the only manifestation of late latent syphilis.
Case Report
A sexually active 62-year-old man presented with a one-month history of pain in the left leg. The pain started below the ankle and along the shank one month ago. Pain was not relieved by rest and was worse at night, keeping the patient awake. The patient was otherwise well and denied experiencing weight loss, weakness, subjective fever, chills, headache, shortness of breath or nausea. The patient had a history of pulmonary tuberculosis in 2008 and had been disease free for one year. He smoked half-a-pack of cigarettes per day and drank 1–2 L of wine per day for 40 years.
Physical examination showed a well-developed man with a temperature of 36.4°C and a blood pressure of 120/80 mmHg. The skin overlying the anterior aspect of the distal left leg was warm, and swelling could be seen below the left knee joint. Joints were not inflamed and lymph nodes were not palpable. Laboratory examination showed that electrolytes, blood urea nitrogen, creatinine, liver function tests, total protein and albumin were all normal except for an elevated alkaline phosphatase level of 281 U/L (normal < 132 U/L). The initial radiographic examinations included plain radiographs and magnetic resonance imaging (MRI). X-ray examination of the skeleton showed osteoporosis and a pathological fracture of the left tibia and fibula bones, with evidence of focal osteolytic lesions and an onion skin-like periosteal reaction (Figure 1). Chest X-ray findings were compatible with a previous history of pulmonary tuberculosis. Routine presurgery physical examination and serological tests for syphilis were performed. T. pallidum particle agglutination test yielded a positive result at a 1:1280 dilution. Serological tests for HIV were negative.
Radiograph of the left tibiofibular showing the presence of pathological fracture
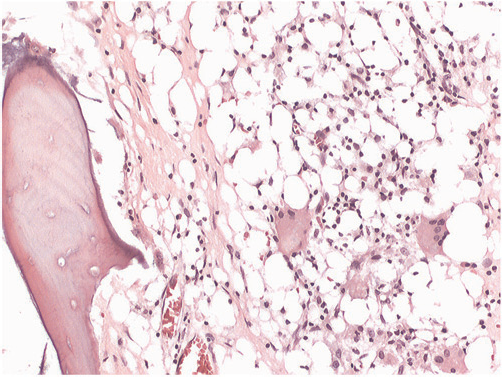
Multiple dark-red sequestra and granulation tissue were seen on surgical debridement of the distal left leg area, and from the biopsy specimens of the tibia and fibula, and the bone marrow. Examination of the biopsy specimens also revealed the presence of bone necrosis with perivascular infiltration of plasma cells, lymphocytes and giant cells. Lymphocytic infiltration was particularly apparent around the small blood vessels (Figures 2 and 3). The final diagnosis of syphilitic osteomyelitis was established by pathological examination.
A low-power photomicrograph of the biopsy shows lymphocytic infiltration with small lymphocytes and giant cells and granulomas (stain, haematoxylin and eosin; original magnification, x40) A high-power magnification of the biopsy specimen shows bone infiltration by plasma cells, some epithelioid cells and occasional giant cells. Lymphocytic infiltration is particularly concentrated around the small blood vessels (stain, haematoxylin and eosin; original magnification, x100)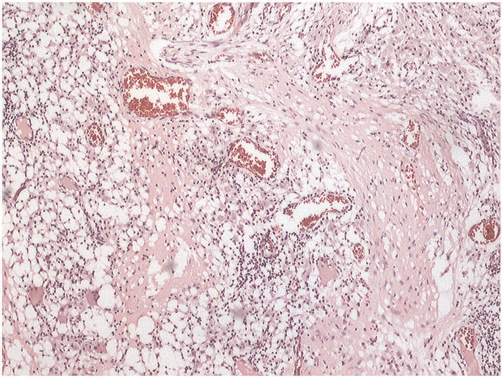
With antibiotic treatment, lower-limb swelling and tenderness noticeably improved. The patient was discharged after completing six weeks of intravenous penicillin. A follow-up in the clinic six weeks later showed resolution of the osteomyelitis.
Discussion
The bone is one of the major systems affected by treponematosis. Treponemes have a pronounced affinity for the bone tissue. Consequently, bones may be affected at all stages of syphilis. In tertiary syphilis, bone lesions may be due to gummas, periostitis or osteomyelitis. The skull and the sternal, clavicular, tibial, fibular, ulnar and radial bones are most frequently affected. 6 However, osseous lesions are encountered rarely for several reasons, such as variations in methods of evaluation and the introduction of penicillin treatment. 7 The current treatment of primary, secondary or early latent syphilis includes the use of a single dose of parenteral long-acting benzathine penicillin G. Patients with late latent, gummatous or cardiovascular syphilis should receive intramuscular benzathine penicillin G at a dose of 2.4 million units once a week for three weeks 5 In developed countries, acquired syphilis is treated promptly, resulting in a decrease in the incidence of syphilitic osteomyelitis. Nevertheless, bone invasion, especially syphilitic osteomyelitis of late latent syphilis, is still seen occasionally. Although it is a recognized feature in tertiary gummatous syphilis, it very rarely occurs as the only manifestation of this disease.
The clinical and radiological appearance of the gummatous changes that affect bone are well known. 8 During the past half century, several cases of syphilis with destructive bone lesions have been reported (Table l).9–18 Most cases occur in conjunction with other symptoms and mucosal or skin lesions. Only a few reports show that bone lesions are the first manifestation of late syphilis. Middleton et al. 14 reported a case of secondary syphilis in a 31-year-old man who presented with bone pain only but with normal X-rays. A 99mTc bone scan showed widespread increased uptake affecting both tibiae, both ulnae and the frontal region of the skull. Our patient also had no other manifestations of tertiary syphilis, but had pathological fracture of tibiofibula, and osteomyelitis was diagnosed only on pathology examination, similar to Dumortier's findings. 19
Bone lesions of syphilitic case reports (1950–2010)
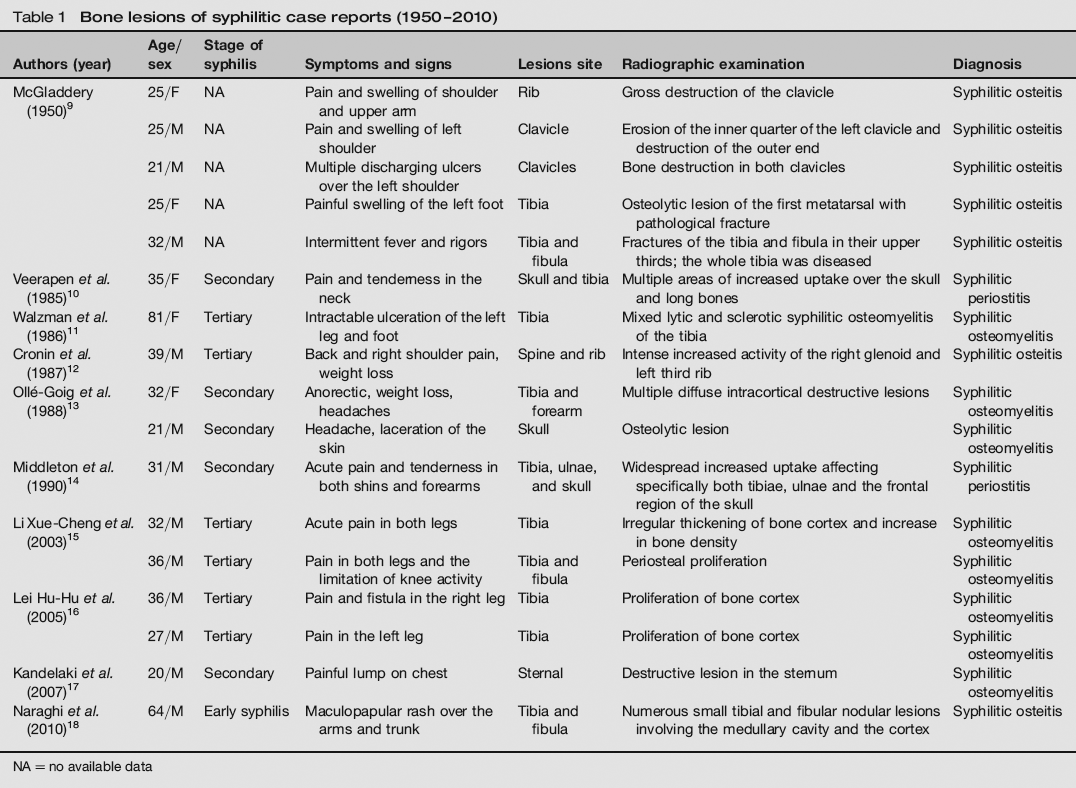
NA= no available data
Syphilitic osteomyelitis is a common occurrence in tertiary syphilis, which starts in the metaphysis, and the earliest radiological change is periostitis. The typical picture in long bones is initially a periosteal proliferative reaction with periosteal elevation, followed by deeper destructive and proliferative changes causing swelling, osteolysis and formation of sequestra. 20 The irregularly increased and decreased activity of the spine, with destructive and blastic changes evident radiographically, indicates that there may be ongoing osteomyelitis, gummatous change or both. 8 X-ray, computed tomography and MRI examinations could be routinely performed, but recent reports indicate that bone scintigraphy is more sensitive than radiography in detecting skeletal lesions in early and secondary syphilis, especially at the stage of periostitis, whereas radiography is preferable for follow-up of patients’ response to treatment. 21 A pathological examination of biopsy specimens should be emphasized as part of the arsenal in the diagnosis of syphilitic disease.
This case shows the value of biopsy pathological examinations in detecting bone lesions of osteomyelitis when the X-ray findings are often atypical. Diagnosis of bone lesions caused by syphilis cannot only depend on typical findings in radiography, but also require confirmatory serological and pathological results.
Footnotes
Acknowledgement
Zhao-yong Liu and Ying Zhang have completed the preparation and the statistics of the manuscript; Kai-feng Qiu and Shi-xin Du revised the manuscript.