
Abstract
Hepatitis C virus (HCV) is a major cause of liver disease in HIV-infected patients. The HCV treatment outcomes and barriers to HCV referral were examined in a centre with a HIV/HCV co-infection clinic. Patients who were antibody positive for both HIV and HCV between 1987 and January 2009 were identified. A retrospective chart review was undertaken. Multivariate analysis was performed to assess predictors of HCV clinic referral. Data were collected on 386 HIV/HCV patients; 202/386 had been referred to the co-infection clinic and 107/202 had HCV treatment. In addition, 29/202 were undergoing pretreatment work-up. Overall sustained virologic response (SVR) was 44%; SVR was equivalent in those who acquired HIV/HCV infection from intravenous drug use (IDU) and others. On multivariate analysis, patients who missed appointments, were younger, with active IDU and advanced HIV and who were not offered HCV treatment were less likely to be referred to the clinic. Patients attending the clinic were more likely to have been screened for hepatocellular carcinoma than those attending the general HIV service. Two-thirds of patients referred to the clinic had engaged with the HCV treatment programme. Dedicated co-infection clinics lower the threshold for treatment and improve management of liver disease in co-infected patients.
INTRODUCTION
Co-infection with hepatitis C virus (HCV) occurs frequently in HIV-infected intravenous drug users (IDUs), 1 those who acquired HIV infection through contaminated blood products 2 and, increasingly, in HIV-infected men who have sex with men (MSM). 3,4 HIV modulates the clinical course of HCV. It has been shown to decrease spontaneous clearance of HCV, accelerate progression to end-stage liver disease and to reduce response to interferon (IFN) therapy. 5 Since the advent of highly active antiretroviral therapy (ART) the incidence of and mortality from AIDS-related illnesses in HIV-infected patients has fallen dramatically. 6,7 Recent large cohort studies have reported HCV-related liver disease as a leading cause of morbidity and mortality in HIV/HCV co-infected patients. 7–10
Despite proven efficacious treatment with combination pegylated IFN-alpha and ribavirin, 5,11,12 uptake of HCV treatment by HIV/HCV co-infected patients has been limited. Studies have consistently showed extensive barriers to accessing treatment, both patient and provider related. 13–19
In 2001, a dedicated HIV/HCV co-infection clinic was set up within the Department of Genito-Urinary Medicine and Infectious Diseases (‘the department’) at St James's Hospital, Dublin, Ireland. Its objective is to provide HCV therapy to co-infected patients within the setting of their HIV primary care provider. Patients with a diagnosis of HIV/HCV co-infection should be referred from the department's general HIV clinics to the co-infection clinic for ongoing management of their HIV, initiation of treatment of their HCV and ongoing surveillance for complications of chronic viral hepatitis. The group have previously published successful outcomes of HCV management in HIV/HCV co-infected patients facilitated by (a) cohorting of patients, (b) individualization of duration of HCV treatment, (c) use of weight-based ribavirin aided by adjuvant use of growth factors and (d) role of rapid virological response to predict primary outcomes. 20–22
In 2009, a review was undertaken to examine the outcomes of the HCV treatment programme. Our aims were to report on the outcomes of (1) HCV treatment, (2) monitoring of liver disease and (3) the prevalence of barriers for HCV clinic referral and treatment in our cohort.
METHODS
A retrospective review was carried out of patients co-infected with HIV and HCV attending the department from its inception in 1987 until January 2009. Patients who had tested positive for both HIV antibody and HCV antibody were identified from the records of the microbiology department. The hospital information system was examined to identify patients who had died or defaulted from care. A chart review was carried out between October 2008 and January 2009 to identify patient demographics, HIV and HCV status, and treatment outcomes. Barriers to HCV treatment for non-treated individuals were identified from the literature and defined for the purpose of the study 13–19 (Table 1).
Definitions of HCV barriers to treatment
HCV = hepatitis C virus; IDU = intravenous drug use
Laboratory parameters
All viral serological and polymerase chain reaction (PCR) studies were carried out at a centralized laboratory (National Virus Reference Laboratory, University College Dublin, Dublin, Ireland). HIV viral load assays were processed using the Versant® bDNA HIV-1 RNA 3.0, (Siemens, Berkeley, CA, USA). The dynamic range of this assay is 50–500,000 copies/mL. From 1994, HCV–RNA was detected using the qualitative Roche COBAS AMPLICOR HCV assay (Roche Molecular Systems, Inc., Branchburg, NJ, USA). In 1997, the Bayer HCV branched DNA (bDNA; Bayer Diagnostics, Berkeley, CA, USA) assay was added to produce a quantitative result. From 2007, hepatitis C viral load assays were processed using the Ampliprep CAP/CTM assay (Roche Molecular Systems, Inc.), which has a range of 15–69,000,000 IU/mL, replacing both previous assays. All assays were used as per the manufacturer's guidelines.
HCV treatment
All patients who undertook HCV treatment received once weekly subcutaneous pegylated IFN alpha 2a (Pegasys®; Roche Pharmaceuticals, Reinach, Switzerland) or pegylated IFN alpha 2b (Pegintron®; Schering-Plough, Kenilworth, NJ, USA) and weight-based dosing of ribavirin twice daily as described in published reports. 20–22
Statistical analysis
Data were collected using a standardized data collection form and an analysis of potential differences between patients who had been referred to the co-infection clinic and those who had not been was performed. Chi-square and Fisher's exact tests were used to examine categorical variables. Mann-Whitney U-tests were used to analyse non-parametric continuous variables. A multivariate backwards stepwise logistic regression analysis using likelihood ratio tests was performed on those variables found to be significant on univariate analysis. Adjusted odds ratios (AORs) and 95% confidence intervals (CIs) are reported. A result was considered to have reached statistical significance if the P value was <0.05. All data analyses were performed using SPSS V.17 (SPSS Inc., Chigaco, IL, USA).
RESULTS
Cohort description
Between January 1987 and December 2008, 3360 HIV-infected patients attended the clinical services of the department. Four hundred and forty-one were identified as having a positive HCV antibody result. HCV PCR was available for all but three HCV antibody-positive patients who were assumed to be HCV PCR positive for the analysis. Forty-two patients (10%) had spontaneously cleared their HCV infection. The medical records of 13 patients could not be located for review despite multiple attempts; eight of these had not attended in the preceding five years. These 55 (12%) individuals were excluded from further analysis. Data were collected and analysed for the remaining 386 patients. One hundred and seven patients (28%) had been treated for their HCV. Ninety-five patients were attending the co-infection clinic but not yet treated (24%). One-hundred and eighty-four patients had not been treated and had not been referred to the co-infection clinic (48%). This comprised 69 patients who had died (37%), 14 patients who had transferred their care (8%) and 101 patients currently attending the general HIV service (55%). The demographics, HIV parameters and HCV genotypes at last documented clinic review are summarized in Table 2.
Univariate analysis of demographics and HIV/HCV parameters of HCV-treated and non-treated patients
HCV = hepatitis C virus; ALT = alanine aminotransferase; ARV = antiretroviral; IDU = intravenous drug use
Treatment outcomes
One hundred and seven (28%) patients had initiated HCV treatment; four (3%) of these patients had subsequently died of liver-related complications (Figure 1).
Treatment outcomes in HIV/HCV co-infected patients HCV = hepatitis C virus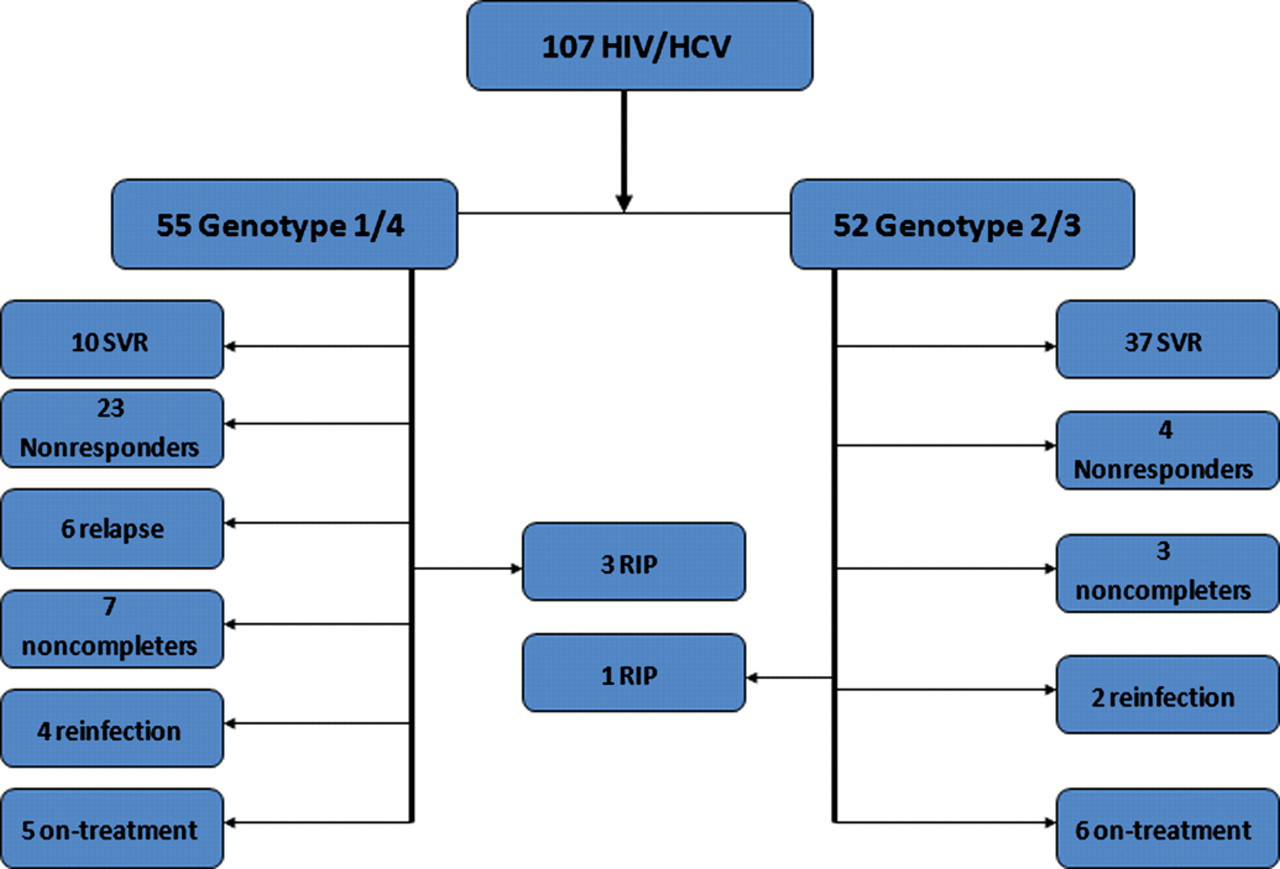
The overall sustained virologic response (SVR) on intention to treat analysis was 47/107 (44%). There was no statistically significant difference in the SVR rate between patients who acquired their HIV/HCV infections through IDU n = 29/47 (62%), and those who acquired their infections by other routes n = 18/47 (38%) (P = 0.2). There was a highly significant difference in SVR rates between those infected with HCV genotype 1/4 and those infected with HCV genotype 2/3 (P < 0.001). Patients infected with HCV genotype 1/4 infection achieved an SVR in 25% of cases (10/54); patients with HCV genotype 2/3 infection achieved an SVR in 71% of treatment courses (n = 37/52).
Monitoring for complications of chronic liver disease
In all, 147/386 patients had an alanine aminotransferase (ALT) >40 IU/mL. Those attending the co-infection clinic were more likely to have had an alpha fetoprotein level checked in the last year, to have undergone abdominal imaging to evaluate their liver parenchyma and to have had a liver biopsy performed, than those who had not been referred to the clinic (P < 0.004) (see Table 3).
Monitoring for complications of chronic viral hepatitis in HIV/HCV co-infected patients with ALT > 40
HCV = hepatitis C virus; ALT = alanine aminotransferase; AFP = alpha fetoprotein; OGD = oesophago-gastro duodenoscopy
Barriers to HCV clinic referral
There were significant differences in the rates at which barriers to HCV treatment identified from the literature (Table 1) occurred in the patients who had been referred to the HCV clinic and those who had not been referred. Multivariate backwards logistic regression analysis was performed. Age groups (in intervals of 5 years), gender, missing appointments, active IDU, advanced untreated HIV, HCV treatment not offered and patient refusal were entered into the model. Patients were more likely to be referred to the co-infection clinic if they were older and not immunocompromised, if they had HCV treatment offered to them, if they were not missing their scheduled appointments and if they did not have current IDU (see Table 4).
Univariate analysis of factors associated with HCV clinic referral and multivariate backwards logistic regression analysis of those variables found to be significant on univariate analysis
IDU = intravenous drug use; HCV = hepatitis C virus; CI = confidence interval
Barriers to HCV treatment
On univariate analysis, there were significant differences in demographics between those patients who had been treated for HCV (107/386 [28%]) and those who had not (279/386 [72%]). Those who had been treated were older (P < 0.001) and more likely to be men (P < 0.01). A greater proportion had a CD4 count greater than 200 cells/μL (P < 0.001) and they were more likely to be receiving current ART (P < 0.001). They were more likely to have advanced liver disease (P = 0.03) and to be infected with HCV genotype 2 or 3 (P = 0.01). They had significantly lower median HCV and HIV viral loads and median ALT (P < 0.001). They were less likely to have IDU as an acquisition risk factor (P < 0.001) and to be receiving opiate substitution therapy (P < 0.001) (see Table 2).
On multivariate analysis, HCV treatment was more likely if a diagnosis of advanced liver disease had been made and less likely if patients had IDU as an acquisition risk, were receiving opiate substitution, had higher ALT (in intervals of 10 IU/mL) or had a CD4 count <200 cells/μL. HCV viral load, HIV viral load, HCV genotype, receiving current ART, gender and younger age were not found to be predictive (see Table 5).
Multivariate backwards logistic regression analysis of demographic and clinical characteristics that predict HCV treatment
IDU = intravenous drug use; HCV = hepatitis C virus; ALT = alanine aminotransferase; CI = confidence interval
DISCUSSION
Outcomes
Previous reports have consistently shown low eligibility for HCV treatment in both HCV-mono-infected IDU and HIV/HCV-co-infected populations. 16,17 Recent reports have shown that HIV infection still limits access to HCV treatment 19 and that patients who acquire HIV and HCV infection through IDU are less likely to receive ART. 23,24 In contrast to this, our results point to successful engagement with HCV treatment or pretreatment work-up in two-thirds of those patients referred to our service. Our treatment outcomes are comparable with those published in large trials of co-infected individuals treated with pegylated IFN and ribavirin. 25–27 This is despite the majority of our cohort being prior or current IDU, a cohort that is reputedly difficult to treat. We found no difference in outcome of HCV treatment between patients infected through IDU and those infected through contaminated blood products.
Model of care
There is extensive literature focusing on identifying barriers to HIV and HCV care in IDU and to overcoming them. 13–19,24,28–31,37,38 Key points that have been identified relate to socio-political, individual and provider-based factors. In the Irish health-care system, socio-political factors play less of a role as all health care to HIV-infected individuals is provided without charge; therefore, individual and provider-based factors predominate.
For the HCV-infected individual, uncoupling of counselling and testing services from provision of HCV treatment has been identified as a major factor in limiting access to treatment. 17 HCV treatment clinics such as ours, which are integrated into primary care provision for HIV, facilitate treatment in HCV/HIV co-infected patients. 30 As many of the challenges in providing access to care for patients with HIV are similar to those facing providers of HCV care, provider-based interventions which have proven successful in increasing the uptake of care by HIV-positive IDUs can be used to increase the uptake of HCV care. These include the establishment of a multidisciplinary team including specialist nurses, on-site pharmacists, medical social workers and physicians with extensive experience in caring for IDUs. 29 We argue that this model is in part responsible for our patients improved engagement in HCV treatment.
Barriers to HCV clinic referral and treatment
While we have successfully engaged a large number of patients, significant barriers to HCV treatment are identified. Despite the integrated clinic, nearly one-third of patients are yet to be referred. These patients were statistically younger and more likely to be women. Younger age group has previously been identified as a barrier to HCV care. 15
Those patients not referred to the HCV co-infection clinic were more likely to default from appointments, to engage in IDU, to have advanced untreated HIV and to not to have had HCV treatment offered to them. Similarly, those patients who had not had their HCV treated were more likely to be immunocompromised, with IDU as their underlying risk factor for HIV/HCV infection. These differences may reflect bias on the part of the referring medical practitioners who may have assessed their liver disease to be less of a priority than other aspects of their care. However, the literature clearly describes the impact of chronic liver disease on morbidity and mortality in HIV-infected patients. 5,8,9,32,33 This emphasizes the need to prioritize HCV treatment and monitoring in this cohort and patients referred to the co-infection clinic were more likely to receive appropriate monitoring of their liver disease when compared with those attending the general HIV service.
Future directions
Some patients referred to the co-infection service had refused HCV treatment. Specific reasons for refusing HCV treatment were not identified; however, prolonged treatment courses, fear of side-effects and low rates of treatment success have been cited as patient-related barriers to treatment. 13 The majority of patients refusing treatment were infected with HCV genotypes 1 or 4 which require longer treatment courses and have lower rates of SVR. Newer agents such as the HCV protease inhibitors, show promising results in mono-infected HCV patients and trials are underway to evaluate their effectiveness in co-infected patients. 34–36 Doab et al. 14 found the acceptability of HCV treatment increased with increasing success rates. Strategies that utilize these new agents in association with early viral kinetics may allow for individualization of treatment regimens and possibly shorter treatment courses. 20,21
Limitations
This study was retrospective and the charts of 13 patients could not be retrieved for review. Analysis of the hospital information system revealed that the majority of these patients had not attended our services for more than five years. As non-attendance was the most frequent cause for not receiving HCV treatment, the majority of these patients would fall into this category. Our cohort was relatively homogeneous, with the majority of patients being white male IDUs. This may limit the generalizability of our findings.
CONCLUSION
Significant barriers to HCV care remain, especially related to substance abuse and outpatient attendance. Establishment of an integrated HIV/HCV co-infection clinic can lower the threshold for HCV care for many patients, resulting in favourable outcomes and improved monitoring of liver disease even in the absence of definitive cure of HCV infection.