
Abstract
Summary
Many countries in sub-Saharan Africa have made antiretroviral therapy (ART) available in urban settings, but the progress of treatment expansion into rural Africa has been slower. We analysed routine data for patients enrolled in a rural HIV treatment programme in Zambézia Province, Mozambique (1 June 2006 through 30 March 2009). There were 12,218 patients who were ≥15 years old enrolled (69% women). Median age was 25 years for women and 31 years for men. Older age and higher level of education were strongly predictive of ART initiation (P < 0.001). Patients with a CD4+ count of 350 cells/μL versus 50 cells/μL were less likely to begin ART (odds ratio [OR]: 0.19, 95% confidence interval [CI]: 0.16-0.23). In rural sub-Saharan Africa, HIV testing, linkage to care, logistics for ART initiation and fears among some patients to take ART require specialized planning to maximize successes. Sustainability will require improved health manpower, infrastructure, stable funding, continuous drug supplies, patient record systems and, most importantly, community engagement.
Introduction
Sub-Saharan Africa has been disproportionately affected by HIV, sustaining greater than two-thirds of the world's burden of HIV infections. 1 Since the early 2000s, increasing funding support has improved access to antiretroviral therapy (ART) in sub-Saharan Africa and elsewhere.2-5 The initial roll-out of many of these programmes targeted capital cities and other urban centres; urban areas of Mozambique began to receive substantially expanded free access to ART in 2004. Between 2004 and 2007, there was a dramatic increase in the number of persons receiving treatment in Mozambique, with an estimated 150,000 or more on ART by 2008. 6 Since the initiation of free HIV care and treatment in Mozambique, there has been a move to expand services into the lower level clinics at the district level and the more rural settings, coinciding with efforts to achieve equity in care in sub-Saharan Africa between historically better-served urban areas and commonly deprived rural areas.7,8 Zambézia Province, like the rest of Mozambique, is suffering from a severe shortage of physicians. In 2007, not all districts in the province had a physician. Currently (late 2010), all of Zambézia's districts have one or two national physicians, but they serve district populations of 100,000-400,000 persons and typically have substantial administrative burdens. As a result, the vast preponderance of health care is delivered by clinical officers (Técnicos de Mediana) and nurses. 5 Other challenges of ART roll-out and service delivery in this extremely rural, resource-limited setting include: low capacity of existing human resources; war-torn physical conditions of the healthcare infrastructure; extremely limited laboratory infrastructure; large geographical distances to reach services, and; frequent ‘stock outs’ of essential medicines due to an under-capacitated supply chain management system.
In 2004, the Mozambican Ministry of Health (Ministério da Saúde or MISAU) initiated a national ART expansion programme funded primarily by the President's Emergency Plan for AIDS Relief (PEPFAR) and the Global Fund to Fight AIDS, Tuberculosis and Malaria, with additional support from the World Bank, the Clinton Foundation HIV/AIDS Initiative, and other government and private sources.2,35 Mozambique's decentralized health system resembles that of many other sub-Saharan African countries.9-11 Within the 11 provinces, three have central hospitals that serve as tertiary care referral centres. The remaining eight provinces have a provincial hospital (including Zambézia Province) that serves as the principal referral centre for the given province. District capitals within each province have health centres or rural hospitals that provide local care. Services are then further decentralized into smaller health centres and health posts that are classified according to the infrastructure and services provided. At the time of its 2004 inception, the ART service initiative was offered in only 10 health centres within six of Mozambique's 11 provinces (Maputo City, Maputo Province, Niassa, Sofala, Tete and Zambézia). As of March 2010, ART services were offered in 223 health centres distributed throughout all 11 provinces of the country. 12
Although there have been analyses conducted of patients enrolled in the larger, urban clinics in sub-Saharan Africa, there are few critical analyses about patients enrolled in PEPFAR-supported care and treatment services in rural areas.13-19 We describe the baseline characteristics, enrolment trends and predictors of ART initiation to present the initial challenges inherent in ART-based rural HIV care.
Methods
Study population
Friends in Global Health LLC (FGH) is a Mozambican-registered non-governmental organization (NGO) affiliated with Vanderbilt University. In 2007, FGH began providing support to MISAU in implementing HIV care and treatment programmes into government hospitals in six rural districts (total estimated 2007 population ∼1.14 million) of Zambézia Province, including Alto-Molócuè (estimated 2007 district population 271,650), Gilé (169,285), Ile (289,542), Inhassunge (91,196), Lugela (135,485) and Namacurra (186,410) 20 (Figure 1). Zambézia Province is Mozambique's second most populated province with ∼4 million people, of whom <14% live in an urban area. 21 In Zambézia, HIV prevalence is an estimated 19% based on antenatal sentinel surveillance of pregnant women aged 15-49 years, ranging from 7% in the northern part of the province to 35% in the provincial capital of Quelimane. 22 Under the ‘emergency’ response model of the early phase of PEPFAR, FGH assumed a role of co-implementer for service delivery during the reporting period, while initiating capacity building of its MISAU counterparts to prepare for the eventual transition of service responsibility.

Map of Mozambique, Zambézia Province, with districts highlighted that receive support from FGH. FGH = Friends in Global Health
Each of these districts has 7-15 health centres or health posts included within their catchment areas. However, at initial expansion and through the period of this report, only one site located in each of the district capital health centres had been authorized by MISAU to provide ART care and treatment. This plan sought to ensure an adequate standard of physical infrastructure and human resources prior to the delivery of ART care and treatment. Due to severe human resource constraints (i.e. health workforce), combined with Mozambican and USA government mandates to limit the number of foreign staff members, it was not possible to support full-time expertise in all of these outlying Zambézia clinics. 23 We analysed data from the cohort of patients enrolled into the HIV care and treatment programme in the six districts between 1 June 2006 and 31 March 2009. Support was provided to the sole MISAU-approved ART health centre in each of these extremely rural, resource-limited districts. Because patients ≥15 years of age are considered adults by MISAU in Mozambique, all patients who had age included in the chart and were identified as adults were included in the analysis (Figure 2).

Total number of patients enrolled in a rural HIV care and treatment programme in Zambézia Province, Mozambique (1 June 2006-30 March 2009) ART = antiretroviral therapy
Care and treatment protocols
During the reporting period, patients who tested HIV-positive in one of the clinics, either in voluntary counselling and testing (VCT) services or in prevention of mother-to-child transmission (PMTCT) services, were referred to the HIV care and treatment programme. While the VCT services are based on an ‘opt-in’ policy where patients voluntarily seek HIV testing, throughout the period of this report Mozambique also practiced an ‘opt-out’ policy towards counselling and testing within the health facilities. In general, the greatest uptake of this policy happens within the PMTCT services, tuberculosis (TB) services and in the inpatient wards.
At the first visit to the HIV care and treatment programme, a nurse provided an initial evaluation consisting of WHO staging and blood drawing for a CD4+cell count, chemistry and haematology. Patients were given appointments to return in two weeks for laboratory results and for a complete clinical evaluation. Patients were eligible for ART if they had a CD4+ count <200 cells/μL and/or WHO stage IV, or 200-350 CD4+cells/μL and WHO stage III. We initiated treatment for eligible persons as per national guidelines with the first line regimen of lamivudine (3TC), stavudine (d4T) and nevirapine (NVP). MISAU guidelines recommend that patients receive three sessions of adherence counselling before initiating treatment. If patients did not qualify for ART after the clinical and laboratory evaluation, they were provided with a return date as per MISAU guidelines, based on the results of the CD4+ cell count: patients with CD4+ count of 201-350 cells/μL returned in three months, those with 351 -500 cells/μL returned in six months and those with >500 cells/μL returned in 9-12 months (unless persons became ill, in which case they were seen at an earlier time point). 24 Of note, as of May 2009, HIV-positive adult patients are determined eligible for ART if: CD4+ count <250 cells/μL independent of clinical status, CD4+ count ≤350 cells/μL and WHO stage III, or WHO stage IV independent of CD4+ count.
Data collection
We conducted our study using routine data collected for monitoring and evaluation by MISAU. Paper forms were completed by the clinicians, pharmacists and counsellors who met with the patients. Data were entered after the patient visit by a data entry staff member at each site into an electronic patient tracking system (PTS) maintained by MISAU and FGH staff. Baseline characteristics were defined as those that were measured within 90 days of enrolment into the programme. We queried out-of-range and missing values. If clearly out-of-range values could then not be confirmed against the paper source, then extreme values were deleted from the database for height (n = 64), haemoglobin (n = 64) and CD4+cells (n = 28) results.
Statistical methods
Enrolment trends for gender and WHO stage were assessed using logistic and proportional odds models. To detect improvement in data collection over time, presence of baseline CD4+cell count or haemoglobin records were modelled by date of enrolment using logistic regression. The aforementioned analyses were conducted for all patients enrolled into care (n = 12,218) and the following model contains all patients that were enrolled by 31 December 2008 (n = 10,712). Predictors of ART initiation within 90 days of enrolment were modelled using multivariable logistic regression, including district, age, gender, education, weight, WHO stage, CD4+cell count, haemoglobin and date of enrolment. To account for possible nonlinear associations, continuous variables were included in the models using restricted cubic splines. 25 In multivariable analyses, missing values of baseline predictors were accounted for using multiple imputation techniques. 26 In this technique, we use other baseline characteristics to predict the missing value for each patient, and then we perform regression on the imputed data. We repeat this task 10 times and take the average estimates from multiple logistic regressions. R-software 2.9.2 (www.r-project.org) was used for data analyses. Analysis scripts are available at http://biostat.mc.vanderbilt.edu/ArchivedAnalyses
Results
Between June and December 2006, each of the six districts began enrolling patients into the HIV care and treatment programme. FGH support for these districts began in early 2007 and by the end of March 2009, 13,045 HIV-infected persons had been enrolled into care. Of those patients, 12,218 (94%) were ≥15 years of age, 673 (5%) were <15 years of age and 154 (1%) did not have age documented in the medical record. For the purpose of our analysis of adult data, we included the 12,218 patients with a documented age of ≥15 years old (Figure 2). While FGH at this time did not provide direct support to the PMTCT or VCT programmes, MISAU data corresponding to the same time period show that 88% of women entering into prenatal care were provided counselling and testing for HIV and that 52% of VCT clients were women (data not shown).
Characteristics at enrolment
Of the patients enrolled in the HIV care and treatment programme, 69% were women. The median age of the female enrollees was 25 years (interquartile range [IQR]: 21-31), and the median age of men was 31 years (IQR: 25-39). We found that 83% of adult patients were illiterate or had received only basic primary school education. Median CD4+ count at enrolment was 371 cells/μL with 13% <200, 17% <250 and 23% ≤ 350 cells/μL (not mutually exclusive categories). Advanced clinical disease was noted in 38% of patients (WHO stage III or IV). Men were more clinically ill at enrolment (51% with WHO stage III or IV) than women (31%), and men had a lower CD4+ count (290 cells/μL) than women (406 cells/μL) at enrolment. Of the 42.9% of patients enrolled for whom we had a body mass index (BMI), 27% had some degree of malnutrition as defined by a BMI < 18.5 (Table 1).
Summary of patient characteristics by gender: newly enrolled HIV/AIDS patients, Zambézia Province, Mozambique, 2006–09

ART = antiretroviral therapy; BMI = body mass index
Continuous variables are reported as medians (interquartile range)
Percentages are computed using the number of patients with a non-missing value
Enrolment data are collected in a window of ±90 days from date of enrolment
Enrolment trends
The percentage of patients enrolling in the clinic who were women increased over time (P < 0.001). In 2006, 61% of patients enrolling were women, whereas in 2009, 72% were women (Table 2). As these HIV care and treatment programmes matured, patients enrolled earlier in their disease process as identified by a lower WHO stage (P < 0.001). In 2006, 42% of patients enrolled with a WHO stage I or II classification, whereas in 2009, 75% of patients were classified as WHO stage I or II at enrolment (Table 2, Figure 3).
Trends in gender, WHO stage, CD4 count and data collection among newly enrolled HIV/AIDS patients, Zambézia Province, Mozambique, 2006–09
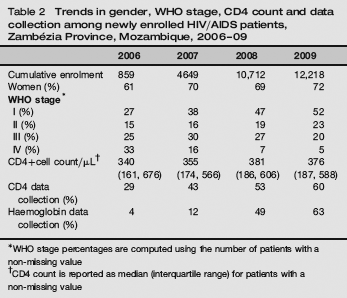
WHO stage percentages are computed using the number of patients with a non-missing value
CD4 count is reported as median (interquartile range) for patients with a non-missing value
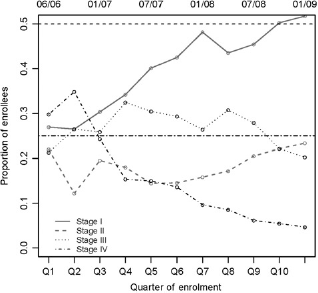
WHO stage at enrolment in programme per quarter of enrolment, Zambézia Province, Mozambique, 2006-09
Data collection trends
To assess improvements in data collection, recorded lab values over time were analysed. A majority of lab values for CD4+ count and haemoglobin were missing: 51% and 64%, respectively, i.e. no recorded measurement within 90 days of enrolment (Table 1). However, CD4+ count and haemoglobin were consistently better documented over time (P < 0.001 for both). Prior to FGH support through PEPFAR, 29% of baseline records had a CD4+ counts and 4% had a haemoglobin recorded in 2006 compared with 60% for CD4 and 63% for haemoglobin in 2009 (Table 2).
Predictors of ART initiation
The characteristics of adult patients initiating ART were summarized for the subset of 10,712 patients who were enrolled in the HIV care and treatment programme by 1 January 2009. Of these patients, 1934 (18%) initiated treatment in the first 90 days following enrolment. Of these 1934 persons initiating ART, the median age was 30 (IQR: 25-38), 68% were classified in WHO stage III or IV, and 57% were women. For persons initiating ART, the median CD4+ count was 165 cells/μL (IQR: 89-273) and median haemoglobin was 10 g/dL (IQR: 8-11). Notably, 36% of the patients who entered the programme and did not initiate treatment within 90 days were lost to follow-up after the first visit and 4% of those who started ART also did not return for a second visit (Figure 2).
Demographic and clinical characteristics were predictive of ART initiation within 90 days (Table 3). Older age and higher level of education were strongly predictive of ART initiation (P < 0.001). Women had 20% lower odds of initiating treatment (odds ratio [OR]: 0.80, 95% confidence interval [CI]: 0.67-0.96). A patient with a CD4+ count of 350 versus 50 cells/μL was less likely to begin ART (OR: 0.19, 95% CI: 0.16-0.23), and patients with more advanced clinical disease stage were more likely to begin ART (WHO stage IV versus I: OR: 7.41, 95% CI: 5.74-9.56).
Logistic regression model effects: ART entry in first 90 days post-HIV diagnosis in newly enrolled patients, Zambézia Province, Mozambique, 2006–09
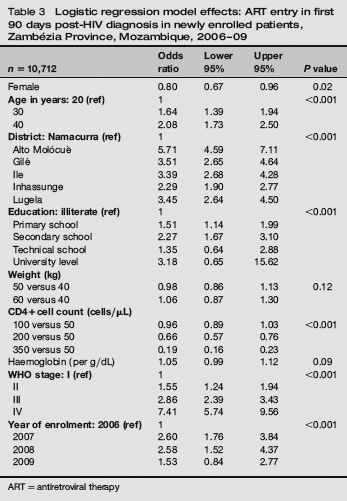
ART = antiretroviral therapy
There were 2268 patients (of 10,712; 21%) who qualified for ART initiation at enrolment (as per MISAU guidelines: CD4 count <200 cells/μL or WHO stage IV or CD4 < 350 cells/μL and WHO stage III). These patients were generally in very advanced stages of HIV disease, with a median CD4 of 134 (IQR: 67-206). However, of these qualifying patients, only 1305 (58%) initiated ART within 90 days of enrolment. Among qualifying patients, those who initiated tended to be older (40 versus 20 years: OR: 1.38, 95% CI: 1.06-1.80), more educated (secondary school versus illiteracy: OR: 2.01, 95% CI: 1.40-2.90), have even lower CD4+ counts (100 versus 50 cells/μL: OR: 0.96, 95% CI: 0.89-01.03) and presented in earlier years (2009 versus 2007: OR: 0.45, 95% CI: 0.31-0.66) (Table 4).
Logistic regression model effects: antiretroviral therapy (ART) entry in first 90 days post-HIV diagnosis in newly enrolled patients determined eligible * for ART, Zambézia Province, Mozambique, 2006–09
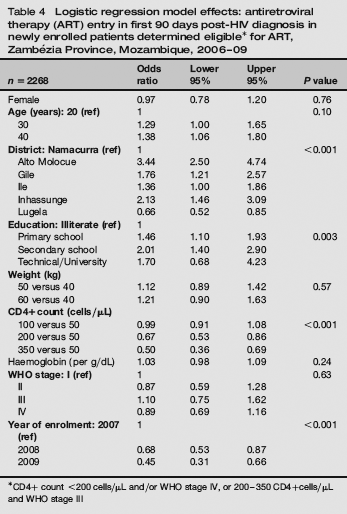
CD4+ count <200 cells/μL and/or WHO stage IV, or 200–350 CD4+cells/μL and WHO stage III
Discussion
Programmatic data from rural Zambézia Province reveal the huge challenges of care and ART-based interventions in the context of a rudimentary health system and severe health manpower shortages. Predictors of ART initiation, for both the total number of patients enrolled in the HIV care and treatment services by 1 January 2009 (10,712) and for the 58% of eligible patients which did initiate ART include higher age and education level, decreased weight, decreased CD4+cell count and advanced WHO clinical stage. The data presented here show that as services matured over time, an improvement in identifying and enrolling patients into care earlier in their disease course was evidenced by lower WHO stage and higher CD4+cell count at entry. While the rural Zambézia programme is improving, there remain serious challenges in the need for targeted interventions to ensure even earlier testing, earlier enrolment into care, earlier treatment initiation and retention after enrolment. These challenges and the lessons learned to overcoming them are presented in much greater detail in a qualitative assessment by the authors. 5
Despite these challenges, the number of persons enrolling into HIV care and treatment in sites supported by FGH increased substantially over the period of study. Characteristics of patients enrolled resemble reports from other sub-Saharan African countries.14,1627 Our enrolled patients were more likely to be female, of younger age, in WHO stage IV, with CD4+ counts <350 cells/μL and with low haemoglobin levels. Given that ART eligibility recommendations of the Mozambican national protocols are based on higher WHO stage and lower CD4+ counts, and given that women of reproductive age are more often seeking health care, these predictors are not surprising.
Outcomes research is not always flattering to a given programme. Overall, of patients who met eligibility requirements, only 58% were initiated on ART within the first 90 days of contact with the health system. In addition, despite treatment protocols from MISAU outlining the eligibility requirements for ART based on WHO stage and CD4+ cell count, of those who were initiated on treatment, a majority were initiated at well below the recommended thresholds. These findings may be attributable to several different factors: (1) three separate pre-ART counselling visits are mandated by MISAU before ART can be prescribed; (2) only a physician or medical technician (técnico de medicina) can initiate the first prescription for ART in a country heavily dependent on task shifting to nurses; (3) there is a bottleneck created for decisions to initiate ART in that a case review at a once-weekly ART committee meeting is required; (4) ART pharmacy stock shortages (‘stock-outs’) are not infrequent, requiring the patient to return to the clinic at a future date.
Higher education level and older age were found to be predictive of ART initiation. While this is an expected finding, it is worrisome in a rural Zambézia Province context. About 85% of patients enrolled into the HIV care and treatment programmes had received minimal to no education and 86% of the provincial population is <40 years of age. 20 Lack of transportation and the extensive distances required to travel to the clinics could possibly contribute to the loss to follow-up and/or death.
Twenty-seven percent of our patients with a registered BMI showed some level of malnutrition. While consistent with what has been reported elsewhere in the literature, the poor nutritional state of our patient population at the time of enrolment reflects the marginal economic circumstances facing the subsistence farmers and fishermen of Zambézia Province, and the programmatic consequence of enrolling patients late in disease. Nutritional support activities are limited at best. In 2009, supplemental and therapeutic foods such as PlumpyNut® were available only for children. The reality of logistical challenges in Zambézia Province often interferes with the consistent implementation of ‘wrap-around’ nutritional and agricultural programmes.
We had large amounts of missing data, particularly at programme inception. Prior to the availability of ART, district level health facilities in Zambézia Province did not have a system for archiving longitudinal patient data and no records were kept on file at the clinic. With the expansion of ART, use of medical records for the HIV care and treatment programme began being implemented using standardized national forms. In order to address the increasing data demands and to improve data quality, FGH assisted with the development of an electronic PTS in the sites in which it provides support. This PTS has proven valuable in the management of patients lost to follow-up by allowing the district health teams to generate reports identifying those patients who have not returned for medication pick-up. Patients are considered Tate’ if they do not appear within 3-59 days of their scheduled medication pick-up and are classified as ‘lost to follow-up’ if they have not appeared within 60 days. Lists are generated on a weekly basis of patients who are late or lost to follow-up, and these are used to prioritize active case finding of the patients by non-clinician community health workers and volunteers. Over time, data quality assurance programmes have also been implemented, which target improved documentation from clinicians, improved transfer of data from the paper record to the electronic PTS and improved analysis of data by the National Health System and partner organizations.
CD4+cell counts (and other routine laboratory testing) became more available during the reporting period, based on improved infrastructure for laboratory monitoring of patients, increased numbers of days open to patients for specimen collection and decreasing the number of repeat visits required by patients to get laboratory blood draws. These improvements were the result of extensive efforts having been made on the parts of MISAU, donor agencies and FGH throughout the reporting period to increase laboratory capacity. As a result, 60% of newly enrolled patients into care had a CD4+cell count in 2009 compared with only 29% in 2006 and of those initiating ART within 90 days, 74% had a CD4+cell count documented versus 42% of those not initiating ART (data not shown). Despite these advances, an ever increasing demand for CD4+cell count and other laboratory results is being placed on an already fragile laboratory system. In their current state the logistics support required for laboratory sample transport, maintenance of equipment, reagent distribution and quality control programmes will rapidly outstrip the resources of the National Health System and international partners receiving funds from a flat-lining PEPFAR programme, as programmes mature and expand. As a result, greater efforts need to be made quickly in order to bring affordable solutions such as point-of-care laboratory technologies to remote health facilities like those found in Zambézia.
PEPFAR is currently undergoing a very important transition in both philosophy and identity as it converts from an emergency response to a response focused on sustainability, and potentially from an HIV response to a broader global health initiative.2,28 Since its inception, PEPFAR has attracted controversy as to whether such global programmes were realistic and sustainable; public health authorities are still defining what is within the realm of possibility in terms of global healthcare development and local management. As PEPFAR transitions its initial ‘emergency’ response to a focus on better sustainability, our data should give pause to policy-makers who expect a rapid, effective changeover to full local control in the most undercapacitated rural settings. It is essential to analyse programme characteristics within the context and demands of a given locale to ensure that the potential policy shifts that are made account for the vast differences encountered across and within countries. 29