
Abstract
We measured plasma human herpesvirus 8 (HHV8) DNA load in consecutive patients presenting with HIV-associated multicentric Castleman disease (MCD) and in contemporaneous patients who had Kaposi sarcoma (KS), lymphoma or other diagnoses. All 11 patients with MCD had detectable plasma HHV8 DNA compared with 18 (72%) of 25 patients with KS, none with lymphoma and one of 38 patients with other diagnoses. Detectable plasma HHV8 DNA levels were higher among MCD patients, median (interquartile range [IQR]) = 43,500 (5200–150,000) copies/mL, when compared with those with KS, median (IQR) = 320 (167–822) copies/mL and those with lymphoma and other diagnoses (one-way analysis of variance; P = 0.0303). Using receiver operating characteristic analysis, a cut-off of >1000 copies HHV8 DNA/mL of plasma helped to discriminate between MCD and other diagnoses, with a specificity of 94.7% and a negative predictive value of 97.3%. The level of HHV8 viraemia, while not diagnostic, may aid discrimination between patients with MCD and those with KS and other systemic illnesses.
Keywords
INTRODUCTION
Human herpesvirus 8 (HHV8) otherwise known as Kaposi sarcoma-associated herpesvirus (KSHV) was first described in association with Kaposi sarcoma (KS) from a patient with AIDS. 1 Subsequently, in patients both with and without HIV infection, HHV8 has been shown to be associated with all epidemiological types of KS, 2–4 with multicentric Castleman disease (MCD) 4,5 and with primary effusion lymphoma. 6,7 In post-transplant patients HHV8 is associated with bone marrow failure 8 and lymphoproliferative disorders. 6,9
HHV8 DNA has been detected in the peripheral blood mononuclear cells (PBMCs) and plasma from patients at presentation with KS, MCD and lymphoma. 2,10–13 Tedeschi et al. 14 recently demonstrated that both PBMC and plasma are adequate for HHV8 quantification. There are conflicting data on the association between detectable plasma levels of HHV8 and specific diagnoses. One study described higher plasma HHV8 ‘viral load (VL)’ among patients with MCD when compared with patients who had KS or lymphoma. 12 In contrast, another study has described lower plasma HHV8 loads in patients with MCD when compared with those who had HHV8-associated solid and primary effusion lymphoma. 11 In patients with confirmed MCD, several studies have described high levels of PBMC-associated HHV8 DNA during clinical relapses, 15,16 in contrast to those who are in remission. 14
Among HIV-infected patients MCD typically presents with fever and lymphadenopathy, with or without hepatosplenomegaly. 17–19 This clinical presentation has a wide differential diagnosis including non-Hodgkin's and Hodgkin's lymphoma, KS, infection with Mycobacterium tuberculosis, disseminated Mycobacterium avium-intracellulare, leishmaniasis and histoplasmosis. 20,21
In this study we measured the plasma HHV8 load in consecutive patients with newly diagnosed HIV-associated MCD and in patients presenting contemporaneously who had KS or other diagnoses; the majority of patients had presented with fever, with or without splenomegaly or lymphadenopathy. Our aims were first to determine the relationship between plasma HHV8 VL and specific diagnoses, and second to identify whether measurement of plasma HHV8 load could be used adjunctively to aid diagnosis of MCD.
METHODS
Patients
Consecutive patients attending the HIV service at either Bloomsbury Clinic, Mortimer Market Centre (MMC), London, UK, or University College London Hospitals (UCLH), London, UK, between January 2007 and July 2009 with a diagnosis of MCD-confirmed histologically 22 and with evidence of fludeoxyglucose (FDG) avidity in lymph nodes with positron emission tomography-computed tomography (PET-CT) 23 were identified from the hospital electronic Clinical Data Repository (CDR) system at UCLH and the e-Oasis system at MMC. All patients with MCD had active disease as defined by the French ANRS (Agence Nationale de Recherche sur le SIDA) 117 CastlemaB trial group: 19 i.e. fever, CRP >20 mg/L in the absence of any other cause and three or more of peripheral lymphadenopathy, splenomegaly, jaundice, ascites, cough, autoimmune haemolytic anaemia and nasal obstruction.
Patients presenting contemporaneously with KS, or other diagnoses, most of who had fever and or lymphadenopathy/splenomegaly and in whom plasma HHV8 VL had been measured were also identified. Information collected from CDR, e-Oasis and from clinical case-notes included details of patients' clinical presentation, in particular the presence of fever, lymphadenopathy or splenomegaly, their CD4 count and HIV VL at the time of plasma HHV8 VL measurement and the final diagnosis. The HHV8 measured closest to the time of patients' diagnosis was used.
HHV8 assay methodology
Venous blood was collected in ethylenediaminetetraacetic acid (EDTA) tubes. Samples were centrifuged within 24 hours of venesection and plasma was removed off the cells in order to reduce the likelihood of cell lysis causing release of HHV8 virus and/or viral genome. The resultant plasma fraction was not further centrifuged.
HHV8 DNA was measured in EDTA plasma using the Qiagen MDx QIAamp96 (QIAGEN, Crawley, UK). Virus nucleic acid purification procedure for DNA extraction and ABI Prism 7000 real-time polymerase chain reaction (PCR) machine (Applied Biosystems, Foster City, CA, USA) with ABgene TaqMan-PCR reagents for detection. KHSV sequences were amplified using the primers and probe for the LANA gene previously described by Bourboulia et al. 24
The quantification was based on a standard curve with a tissue culture-derived in-house standard, calibrated by comparison to a DNA standard calculated by Poisson endpoint dilution. The assay used murine cytomegalovirus (mCMV, VIC/TAMRA probe) as an internal control introduced at the extraction stage. 25 The multiplex real-time PCR detected both HHV8 and mCMV with the differently labelled TaqMan probes. An in-house ‘run control’ of 1000 copies, as well as the performance of the standard curve, was used as routine monitors of test performance. This assay is intended for detection of HHV8 DNA in the serum or plasma, and quantification of HHV8 DNA between 100 and 28,300 copies/mL with extrapolation to higher VLs.
Statistics
One-way analysis of variance (ANOVA) was used to compare results of detectable plasma HHV8 DNA among different patient groups. GraphPad Prism Version 5.0c (GraphPad Software Inc, La Jolla, CA, USA) was used for statistical analysis; P < 0.05 was regarded as statistically significant.
RESULTS
Between January 2007 and July 2009, 86 HIV-infected patients (67 men) had plasma HHV8 VL measured. Their median (interquartile range [IQR]) CD4 counts were 160 (60–320) cells/μL. Eleven patients had MCD; all had peripheral lymphadenopathy, 10 had splenomegaly, six had jaundice, four each had ascites, cough or autoimmune haemolytic anaemia, two had nasal congestion and one had pleural effusions. Of the 11 patients with MCD, four also had visceral KS. Twenty-five patients had KS (17 with disseminated or visceral disease and 8 with cutaneous disease only), 12 patients had lymphoma and 38 patients had other diagnoses (Table 1), including one patient with the hyaline vascular variant of Castleman disease. Of the 12 patients with lymphoma, two had primary effusion lymphoma (in one the diagnosis was made on cytology of pleural fluid and in the other on histology of a pleural biopsy); in both HHV8 was demonstrated by immunohistochemistry. 26 Four patients had Hodgkin's lymphoma and six had non-Hodgkin's lymphoma (4 had diffuse large B-cell lymphoma and 2 had plasmablastic lymphoma). Of the six with non-Hodgkin's lymphoma, immunohistochemistry for HHV8 was negative in four and not done in two.
Diagnoses in 86 HIV-infected patients in whom plasma HHV8 was measured
DRESS syndrome = drug rash with eosinophilia and systemic symptoms; CMV = cytomegalovirus; PCP = Pneumocystis jirovecii pneumonia; HHV8 = human herpesvirus 8
*Four patients also had visceral Kaposi sarcoma
The patients' clinical presentations are shown in Figure 1. All 11 patients with MCD had lymphadenopathy; nine also had splenomegaly (of these, 7 also had fever); both patients without splenomegaly had fever.

Clinical features at presentation among 86 HIV-infected patients. (a) Patients with detectable plasma HHV8 DNA (n = 30). Four patients had no lymphadenopathy, splenomegaly or fever. (b) Patients without detectable plasma HHV8 DNA (n = 56). Nine patients had no lymphadenopathy, splenomegaly or fever
Detectable HHV8 DNA was identified in plasma from 30 (35%) patients (Figure 1a). Among 73 patients who had lymphadenopathy, fever and or splenomegaly, HHV8 was detectable in 28 (38%). All patients with MCD had detectable quantifiable plasma HHV8 DNA whereas only 18 (72%) of patients with KS had detectable plasma HHV8 DNA (Table 2). KSHV DNA was quantifiable in 16 of these 18 patients and detectable but below limits of quantification in two patients. Of the 38 patients with lymphadenopathy but no detectable HHV8 DNA in plasma, surgical lymph node biopsy was performed in 19 and fine-needle aspiration of a lymph node performed in two patients. There was no histological evidence of MCD in any of these 21 patients.
HHV8 viral load, HIV viral load and CD4 counts in 86 patients
HHV8 = human herpesvirus 8; IQR = interquartile range; VL = viral load
*CD4 count and HIV viral load not available for one patient
Only one patient without an HHV8-related diagnosis had detectable quantifiable HHV8 DNA in plasma with a VL of 2300 copies/mL. At this presentation the patient had fever and a lower respiratory tract infection that responded to conventional antibiotics and did not have KS, MCD or lymphoma. On FDG PET-CT imaging there was no abnormal FDG avidity and no hepatosplenomegaly or lymphadenopathy was evident. After 17 months of follow-up the patient remains asymptomatic.
Detectable plasma HHV8 DNA levels were higher among patients with MCD (median [IQR] = 43,500 [5200–150,000] copies/mL) when compared with those with KS (median [IQR] = 320 [167–822] copies/mL), and when compared with those with other diagnoses, and among those with KS when compared with those with other diagnoses (one-way ANOVA; all comparisons, P = 0.0303) (Table 2). Although there was a significant difference in plasma HHV8 levels between the groups, there was also considerable overlap (Figure 2).
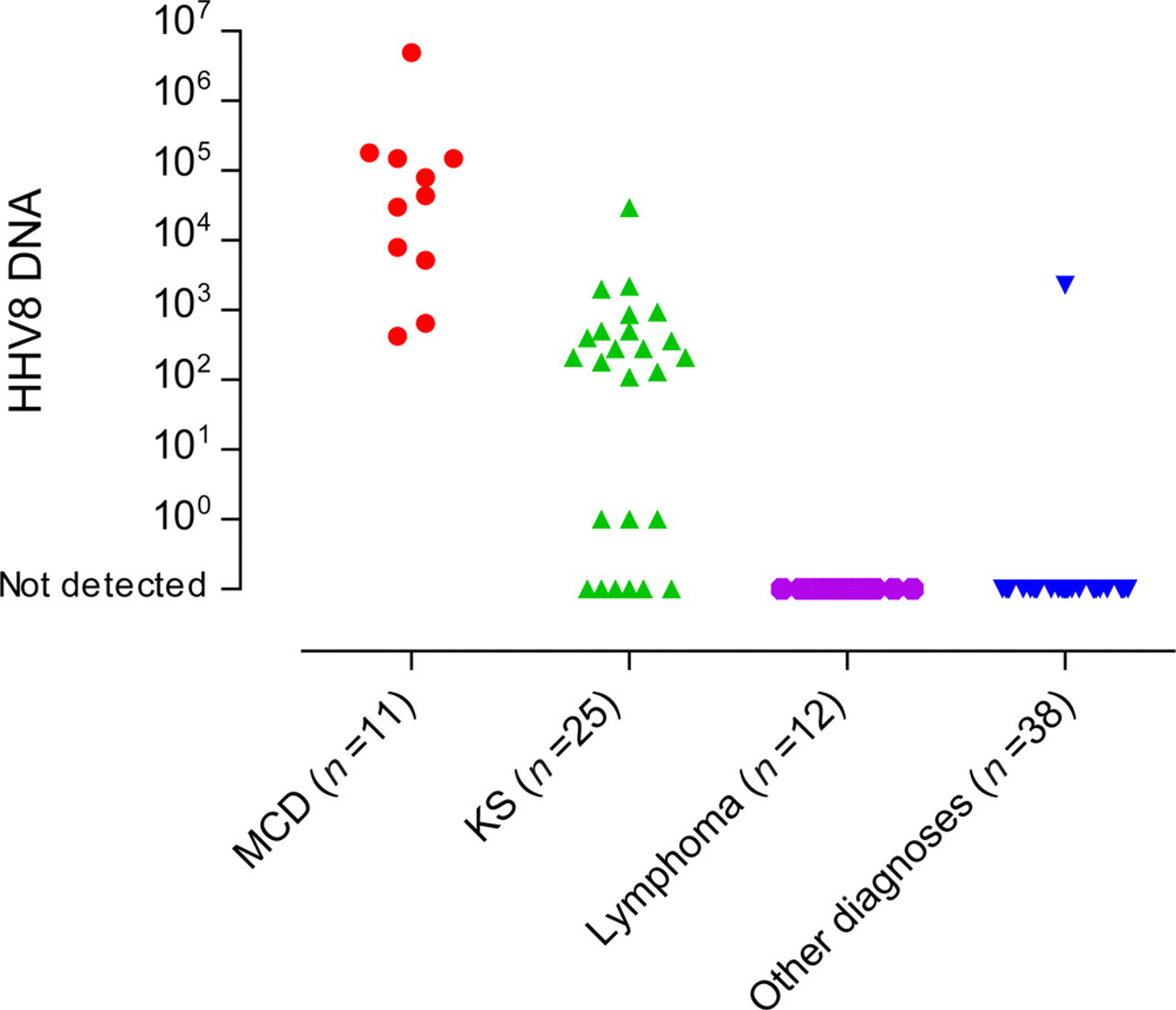
Plasma HHV8 viral loads in 86 HV-infected patients with multicentric Castleman disease (MCD), Kaposi sarcoma (KS), lymphoma and other diagnoses
An HHV8 VL of <100 copies/mL had a negative predictive value (NPV) of 100% for MCD in this group. Using receiver operating characteristic (ROC) analysis the quantity of detectable plasma HHV8 DNA enabled discrimination of patients with MCD from patients with all other diagnoses (including KS); a cut-off of >1000 copies/mL had a sensitivity of 81.8%, a specificity of 94.7% and a NPV of 97.3%; a cut-off of >10,000 copies/mL had a sensitivity of 63.6%, a specificity of 98.7% and a NPV of 94.9%.
DISCUSSION
The main finding of this study was that having HHV8 DNA detectable in plasma was indicative of an HHV8-related disease, specifically MCD or KS. All patients with MCD had detectable plasma HHV8 DNA, as did 72% of those with KS. By contrast, none of those with primary effusion and other plasmablastic non-Hodgkin's lymphoma had detectable plasma HHV8 DNA.
We found that the quantity of detectable plasma HHV8 DNA generally enabled discrimination between patients who presented with MCD and those who had KS and other diagnoses. Specifically, using ROC analysis, if a cut-off of >1000 copies HHV8 DNA/mL of plasma was used to aid discrimination between MCD and other diagnoses, this had a specificity of 94.7% and an NPV of 97.3% for diagnosis of MCD. This study did not attempt to assess whether in patients with MCD and KS there was a correlation between the extent of tumour ‘bulk’ as seen on FDG PET-CT and the quantity of detectable HHV8. This possibility requires further investigation in a prospective multicentre study.
When interpreting the findings of this study it is important to consider its limitations. First, our study is from a single centre, second it is retrospective and third it is based on a single initial HHV8 test result obtained at a patient's initial diagnosis and before institution of specific therapy. Our observations require confirmation in a multicentre prospective evaluation. Fourth, we obtained EDTA venous blood from all patients and centrifuged to separate plasma within 24 hours of collection. It is possible that in this interval some PBMC may have lysed, releasing HHV8, or viral genome, thus potentially elevating plasma HHV8 levels in individual patients. However, once cells have lysed and released viral DNA ‘clarification’ by centrifugation of plasma will not reduce the HHV8 VL, unless the sample is pelleted, which might in turn reduce levels of detectable plasma HHV8 DNA.
Only one patient, who did not have an HHV8-associated diagnosis and who had a confirmed alternative diagnosis, had detectable plasma HHV8 DNA. Given that MCD is a disease with fluctuating symptoms and clinical signs it is possible that this could have been the underlying diagnosis at the patient's presentation with a lower respiratory tract infection and that optimization of HIV treatment alone could have treated an HHV8-related illness before significant lymphadenopathy became clinically apparent to enable histological confirmation by biopsy. 22,27–29 Alternatively, this patient may have had an interleukin-6-related systemic inflammatory syndrome. 30
The data from our study confirm the preliminary observation made by Powles et al., 12 who identified higher plasma HHV8 DNA levels in patients with MCD when compared with patients who had KS, lymphoma or other diagnoses. Simonelli et al. 11 also described detection of plasma HHV8 DNA in patients with MCD, primary effusion lymphoma and HHV8-solid lymphoma. When compared with those who had HHV8-associated solid lymphoma or primary effusion lymphoma, those with MCD had lower median plasma HHV8 VLs. 11 Our data contrast with that of Simonelli et al., 11 as we were unable to demonstrate detectable plasma HHV8 DNA in any patient with lymphoma. The observation that neither patient with primary effusion lymphoma had detectable HHV8 DNA in plasma is surprising, given previous descriptions of the association. 11,12,14 At diagnosis of primary effusion lymphoma both patients were receiving highly active antiretroviral therapy (HAART) and had undetectable HIV VLs. Recently, it has been shown that HAART alone may induce clinical and radiological responses in patients with MCD; in three-quarters of patients HHV8 VLs became undetectable. 22 Thus, it is possible that HAART in the two patients with primary effusion lymphoma had additionally controlled HHV8 expression.
Patients with advanced HIV disease commonly present with fever, lymphadenopathy and splenomegaly. The findings from the present study suggest that a lack of detectable plasma HHV8 DNA in such patients strongly infers a diagnosis other than MCD.
In conclusion, our study suggests that in HIV-infected patients presenting with fever, lymphadenopathy and/or splenomegaly, the absence of detectable HHV8 DNA in plasma excludes a diagnosis of MCD while demonstration of detectable plasma HHV8 DNA is indicative of having an HHV8-related disease, specifically MCD or KS. Furthermore, the level of HHV8 viraemia, while not itself diagnostic, can help in discriminating those patients who are likely to have MCD from those with KS.