
Abstract
The new National Institute for Health and Clinical Excellence (NICE) guidance cites genitourinary (GU) medicine clinics as one setting where screening for alcohol-use disorders should be part of routine clinical practice. Northumberland GU medicine service has routinely used the Fast Alcohol Screening Tool (FAST) since June 2009. An audit of all first attendees to the service in April 2010 (n = 256) was carried out. This audit found that the FAST questionnaire was acceptable to both patients and staff (uptake of 95.7%). Statistically significant associations between excessive alcohol and higher rates of unprotected sex (P < 0.01), an increased number of sexual partners (P < 0.01) and higher rates of sexually transmitted infection (STI) diagnosis (P < 0.05) were also demonstrated.
Introduction
Twenty-six percent of people in England have an ‘alcohol-use disorder.’ 1 The World Health Organization (WHO) has subcategorized this definition into ‘hazardous drinking’ (alcohol consumption that will probably eventually cause harm), ‘harmful drinking’ (alcohol consumption that is already causing damage to physical or mental health) and ‘dependent drinking’ (the diagnosis of which requires three of the following: a compulsion to drink, difficulty in controlling drinking, physiological withdrawal, tolerance, neglect of other pursuits, or persistent drinking despite evidence of harm). 2
Genitourinary (GU) medicine clinics specialize in the prevention and treatment of sexually transmitted infections (STIs) and problem drinking has previously been shown to be clearly associated with an increased risk of STI, across a wide variety of populations. 3 The recent publication of the National Institute for Health and Clinical Excellence (NICE) public health guidance, Alcohol-use Disorders: Preventing Harmful Drinking, therefore specifically cites GU medicine clinics as one location where screening for, and giving advice on, harmful drinking should take place. 4
There are validated questionnaires available as screening tools. FAST (Fast Alcohol Screening Tool) is a shortened form of the 10-item AUDIT questionnaire, which was developed by WHO. It contains four questions and takes 20 seconds to complete. 2 It is scored between 0 and 16 and a score of 3 or more indicates hazardous, harmful or dependent drinking. In a recent systematic review of the use of alcohol screening tools in the emergency department, FAST was shown to be the best tool for identifying alcohol misuse with a sensitivity of 93-94% and a specificity of 86-88% 5
The north east of England is recognized as being an area of the UK with a higher than average problem with alcohol 6 and this audit looks at the use of the FAST questionnaire within the GU medicine service in Northumberland.
Methods
Since June 2009, all first attendees to the GU medicine service in Northumberland have been given a FAST questionnaire upon arrival at the clinic. It is completed in the reception. Their FAST score is then available in the clinic notes when they are seen. Those patients with a score of three or more are given verbal advice and written information and are then offered brief intervention or referral into alcohol services (See Table 1). An audit was carried out looking at all first GU medicine attendees in April 2010. Local standards set for this audit were (target 100%):
Interventions provided to those scoring three or more on the FAST screening questionnaire
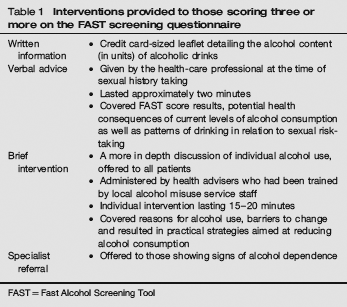
FAST = Fast Alcohol Screening Tool
All case-notes contain a completed FAST questionnaire or a documented reason for non-completion;
The score for each completed questionnaire is documented;
Those with a score of three or more had a documented intervention.
Data were also collected on rates of STI diagnoses, levels of condom use and average number of sexual partners.
Results
Two hundred and fifty-six sets of notes were audited. One hundred and fifty-four (60.2%) had a FAST score of three or more and 91 patients (35.5%) scored less than three. Only 11 (4.3%) patients declined completing the questionnaire. The average age of the sample was 25 years and 53.5% were men.
The main findings from this audit are presented in Table 2.
Summary of audit findings

STI = sexually transmitted infection; FAST = Fast-Alcohol Screening Tool
STI diagnoses included; chlamydia, gonorrhoea, genital herpes (laboratory confirmed), genital warts, molluscum contagiosum, pelvic inflammatory disease (PID) and non-specific urethritis (NSU)
People, during the audit period, presented as contacts of: chlamydia, gonorrhoea, NSU, PID or primary syphilis
A statistically significant association was found between a FAST score of three or more and a higher number of sexual partners (Mann-Whitney U test P < 0.01), higher rates of diagnosis either with an STI or as an STI contact (Fisher's exact test, P < 0.05) and higher rates of unprotected sex (Fisher's exact test, P < 0.01).
Of those patients identified with an alcohol use disorder, 94/154 (61.0%) received verbal or written advice, 12/154 (7.8%) received an additional brief intervention but 31.2% did not have their alcohol use addressed.
Discussion
The link between alcohol and poor sexual health is well documented.7,8 As has been demonstrated in our audit and elsewhere, increasing levels of alcohol use leads to increased STI exposure.3,9 Alcohol intake may lead to a loss of willpower or inhibitions, unprotected sex, not knowing whether sex has taken place or sexual assault. 10 It also has an adverse effect on the immune system.3,11
This audit has shown that screening for alcohol-use within a GU medicine setting is achievable. However, probably the main challenge in the GU medicine setting will not be screening for but dealing with issues of excessive alcohol consumption once identified. This is demonstrated in this audit by 31.2% of patients receiving no intervention. The main reason for this was patient choice, but time constraints and availability of appropriately trained staff also played a part.
The management of alcohol-use disorders is dependent on the level of alcohol consumed. Advice and brief interventions are appropriate for hazardous or harmful drinkers; however, alcohol dependence always requires specialist input. 2
With payment in the GU medicine setting being largely driven by number of patients seen, whether it is possible to dedicate this extra time will be a real challenge. However, it is clear both from this audit and prior research that excessive alcohol use and risky sexual behaviour, leading to an excess of STI diagnoses, are inextricably linked.