
Abstract
Prior to 2006, diagnoses of heterosexually acquired syphilis were rare in Teesside (an area in the north east of England, UK). Since 2006, there has been an increase in such cases, with 24 cases diagnosed in 2006 and 22 in 2007. There was a marked reduction in cases in 2008 with six cases reported, but a large increase in diagnoses in 2009 (34 cases). There have been 14 cases to date in 2010. Of concern is the increase noted in women and younger age groups. Geographical mapping of cases shows a wide dispersion across Teesside although some clusters were identified, mostly in areas of high deprivation. Little detailed information is available to help identify social and sexual networks widely and target intervention. A multiagency outbreak control team is addressing this problem, based on the principles of partner notification, increased awareness, increased screening and health promotion activities. A range of measures, including a detailed communications plan, have been implemented.
INTRODUCTION
Since 2006 there has been a distinct heterosexually-transmitted syphilis outbreak in the Teesside area of north-east England, UK. A dedicated multiagency outbreak control team (OCT) has been addressing this problem.
This short report outlines the current epidemiology associated with this outbreak and describes the control measures taken to date.
CURRENT EPIDEMIOLOGY
There are three genitourinary (GU) medicine clinics across Teesside situated in Hartlepool, Middlesbrough and Stockton-on-Tees. The Teesside area comprises a population of 560,000 people. Prior to 2006, diagnoses of heterosexually-acquired syphilis were rare in Teesside, with typically between zero and three cases per year. Since 2006 there has been an increase in such cases, with 24 cases diagnosed in 2006 and a further 22 in 2007. There was a marked reduction in cases in 2008, with six cases reported. However, a large increase in diagnoses was seen in 2009 with a total of 34 reported. There have been 14 cases reported to date in 2010 (Figure 1).

Epidemic curve of heterosexual syphilis cases for the Teesside area, 2006–10
Of concern is the increase noted in women and the increasing trend towards younger age groups. Of the cases who presented in 2009, 23 of the 34 reported cases were women (68%). Thirteen (57%) of these female cases diagnosed in 2009 were aged 19 years or younger, with 19 (83%) being under 30 years. Two (18%) of the male cases were aged 19 years or younger with 10 (91%) being under 30 years. The majority of cases are white British, with 85% of those cases seen in 2009. Most cases have been diagnosed as primary syphilis in the outbreak to date (82%), though there has been a small increase in the numbers of early latent cases since 2009. This trend will need to be observed further.
Cases have been detected by a mixture of presentations such as self-referral for symptoms (either directly to GU medicine clinics or via primary care services), antenatal screening and through contact tracing of cases.
To put this rise in heterosexual syphilis cases into context, although rates of teenage pregnancy are higher than the national average across Teesside, the broad trend has remained stable or declined during the same time period. Numbers of cases of gonorrhoea and chlamydia diagnosed in GU medicine clinics across Teesside have not shown the same increases as syphilis. Similarly, numbers of cases of syphilis diagnosed in men who have sex with men in GU medicine clinics have not shown the same increase in numbers and have varied little in the same time period.
A worrying development has been the recent diagnoses of two cases of congenital syphilis. This emphasizes the importance of good community control of disease as neither of these cases were preventable otherwise. The mother of the first case was diagnosed on antenatal screening and received appropriate treatment but despite evidence of response to treatment, her baby subsequently developed congenital syphilis. The second case actually screened negative initially in pregnancy and appears likely to have acquired disease later during pregnancy.
Geographical mapping reveals cases in many areas across Teesside although there were clusters seen in central Middlesbrough and central Stockton-on-Tees, as well as in east Middlesbrough. Many cases were found in geographical areas of high deprivation (Figure 2).
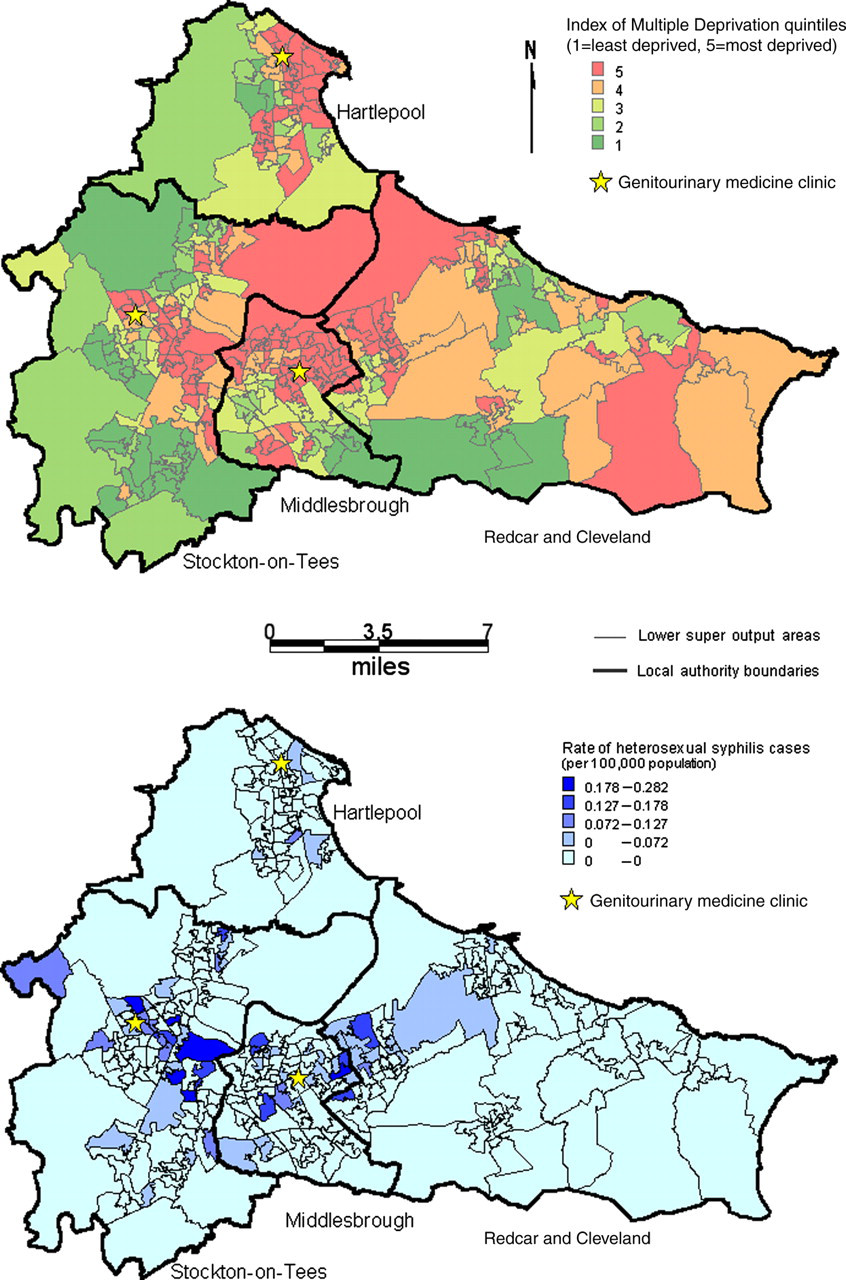
Maps showing rates of disease by Index of Multiple Deprivation (indices of deprivation for 2007 can be found at:
Further analysis reveals that although some cases appeared to be clustered geographically, other cases known to be linked to each other live some distance apart. In the course of this outbreak to date there have been numerous examples of linked cases, but these have rarely been greater than two, or occasionally three, in number. The only sizeable cluster was of seven cases linked indirectly to each other. Investigation revealed these contacts were mainly through an informal network of friends only, with no other obvious link being available to target.
Despite re-interviewing cases, little information has been obtained that helps to identify social and sexual networks widely and hence target intervention, although a number of cases have mentioned social networking sites as a source of sexual partners (20% of those seen in 2009). New cases continue to be interviewed in detail to help identify any such networks.
There appears to be no known links to the sex worker industry.
CONTROL MEASURES AND COMMUNICATIONS
The multiagency OCT is basing their work on the principles of partner notification, increased awareness, increased screening and health promotion activities. A range of measures has taken place including raising awareness through primary care, sexual health services both in GU medicine clinics and in the community and linking with others such as teenage pregnancy coordinators and local authority partnership groups. Increased screening has been suggested in community clinics but any further targeted screening is difficult at present due to a lack of appropriate groups to target specifically. Partner notification of cases has been hampered by the fact that many contacts are simply unknown or untraceable. Overall, approximately half of all contacts have been traced.
A detailed communications plan was developed and implemented. This included production of posters and leaflets, press releases, a radio advertising campaign and street promotions teams to distribute materials, including pubs and clubs across Teesside. There has been consequent media interest in reporting this outbreak, particularly around the issue of social networking sites being used as a potential way of sourcing sexual partners generally.
In addition, advertisements were placed on a social networking site linked to the user's registered postcode. Over an eight-week period these adverts were seen by large numbers of local people. There were 10.5 million page impressions for women and 2.74 million for men, resulting in 3785 and 1656 clicks, respectively, through to the National Health Service Tees website where more information was available.
ISSUES FOR FUTURE CONTROL
A number of issues and challenges remain in the control of this outbreak. The OCT is agreed that the same principles of control apply and work will continue to be framed by these. However, this is now a long running outbreak and an important issue is that of repeated messages to the public. The OCT is mindful that having recently implemented a detailed communications plan that any future activity will have to be tailored and targeted where possible to keep the messages fresh and maximize the chance of these being effective.
Further challenges remain with identifying networks where possible, monitoring and controlling numbers of antenatally diagnosed cases and the issue of integrating this defined outbreak into the wider sexual health agenda locally. There are also challenges to be faced with partner engagement through imminent health service reorganization and reform.
LESSONS IDENTIFIED TO DATE
A multiagency approach with local knowledge is needed to tackle such an outbreak;
Sexually transmitted infection outbreaks can be a challenge, as control measures are not directly in the hands of an OCT;
Despite widespread awareness raising it can be difficult to change behaviour;
Targeting interventions may not be possible if cases are widespread and apparently often unlinked. Without specific information, control measures can only be generic and this may reduce their effectiveness;
Media coverage may not be in a manner an OCT anticipates. However, this may provide benefits by raising the profile of an issue in a different way;
Advertising on social networking sites can significantly increase the reach of health messages and make them visible to large numbers of people.
Footnotes
ACKNOWLEDGEMENTS
GU medicine clinic health advisers and the Health Protection Agency North East Information team are thanked for their ongoing work in helping to document and control this outbreak.