
Abstract
Lichen planus is a chronic inflammatory mucocutaneous disorder of the skin including the scalp, the nails, and the oral and genital mucosae. Ocular, oesophageal, bladder, nasal, laryngeal, otic, gastric, and anal involvement has been documented. In this report, we describe a unique case of orogenital lichen planus affecting the external urinary meatus, masquerading as sexually transmitted urethritis and erosive genital disease.
INTRODUCTION
Lichen planus is a well-known papulo-squamous disorder, generally limited to the skin and/or mucous membranes. 1 It is often erosive as well, especially in the mouth, vagina, and vulva. Nails are affected in more than 10% of the cases. 1 It is a distinct clinical entity with a characteristic colour, morphology and patterns of evolution. Microscopic features, similar to the gross morphology, are diagnostic. 2 Lichen planus presenting with simultaneous oral and genital involvement in malesmen is relatively uncommon and often difficult to diagnose. 3
Moreover, involvement of the external urinary meatus has not been reported to date. A case of lichen planus affecting the external urinary meatus and the buccal mucosa in a 42-year-old man is illustrated.
CASE REPORT
A 42-year-old man presented with complaint of intermittent dysuria and frequency for the past two years. He denied any history of urethral discharge, haematuria, or genital ulceration. He did not give any history of symptoms in the spouse, substance abuse or any significant medical and surgical history. The patient was a shopkeeper and did not report any premarital or extramarital sexual contacts. He was diagnosed as a case of genital herpes at a regional hospital and was treated with intermittent courses of oral aciclovir in a dose of 400 mg three times a day, without any improvement. Examination of the mucosa of the external urinary meatus revealed a violaceous, 1 cm sized plaque with presence of two small erosions and white striae (Figure 1). On palpation, the lesion was non-tender and non-indurated. No urethral discharge was evident on milking the urethra and the rest of the mucocutaneous examination was unremarkable except for the presence of violaceous plaques with linear, white striations over bilateral buccal mucosae. Lymphadenopathy was absent. Muco-cutaneous examination was unremarkable except for the presence of violaceous plaques with linear, white striations over the buccal mucosae bilaterally. Systemic examination was within normal limits. Potassium hydroxide preparation and Tzanck-stained smear from the meatal lesion did not reveal any fungal elements or giant cell formation, respectively. Treponemes were not detected on dark ground illumination of the secretion from the lesion. Gram stain of urethral smear, urine microscopy and culture were negative. Serology for herpes simplex virus (HSV) with enzyme-linked immunosorbent assay (ELISA) for gG1 and gG2, as well as Venereal Diseases Research Laboratory test and HIV ELISA were negative, as was a lesional sway using multiplex polymerase chain reaction for HSV, Haemophilus ducreyi and Treponema pallidum were also negative. Biopsy from the buccal mucosal lesion showed saw-toothing, basal cell vacuolation and dissolution, lympho-histiocytic lichenoid infiltrate and pigment incontinence (Figure 2). Aurologist advised against biopsy of the urinary meatal lesion due to the high risk of subsequent complications at this site. On the basis of the clinic-histological findings, a diagnosis of lichen planus involving the external urinary meatus and buccal mucosae was made. The patient was started on topical clobetasol propionate 0.05% gel for both genital and oral lesions. The urinary meatus lesion resolved completely following the treatment in three months and the oral lesions also improved partially.

A violaceous plaque depicting white striations and two small erosions, affecting the external urethral meatus
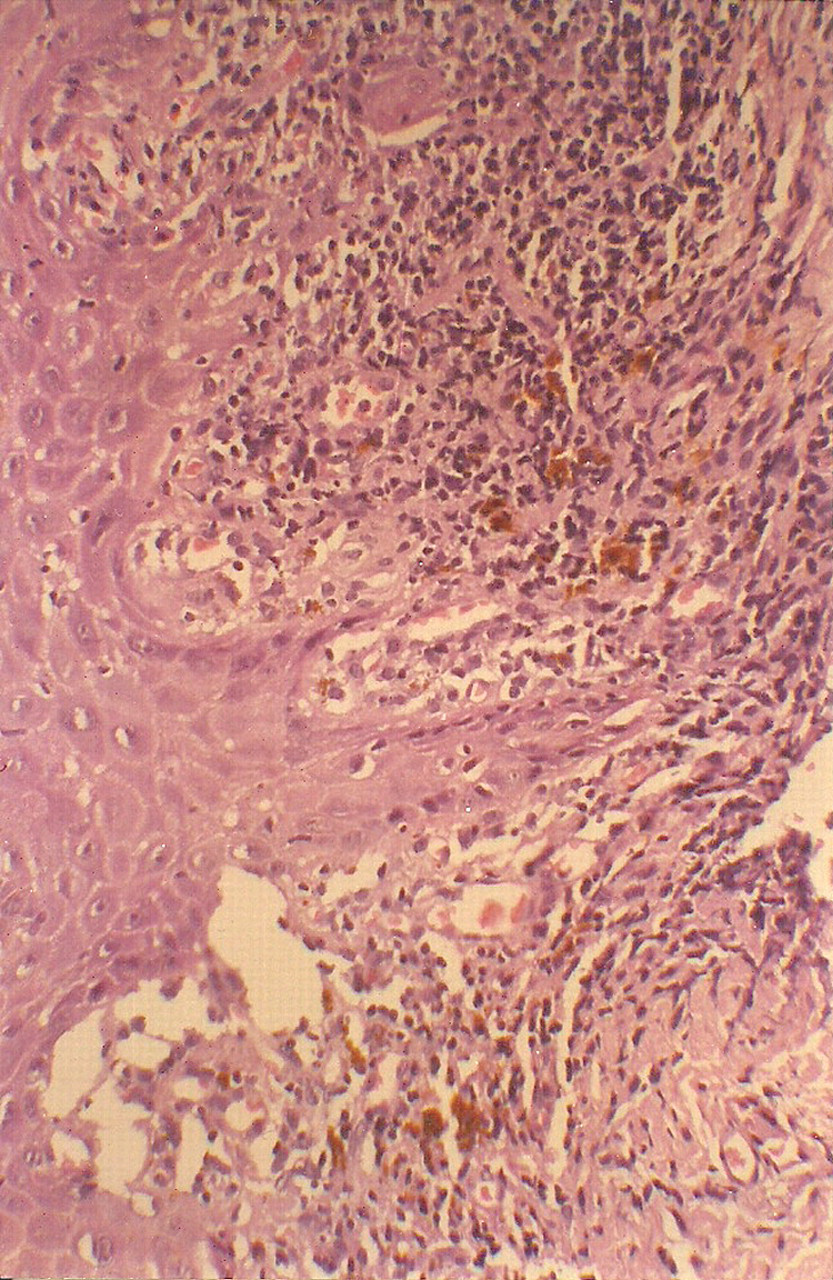
Section from violaceous plaque in the oral mucosa shows sawtoothing, basal cell vacuolation and dissolution, lympho-histiocytic lichenoid infiltrate and pigment incontinence (haematoxylin and eosin stain, ×400)
DISCUSSION
Oral cavity involvement is often the sole manifestation of mucosal lichen planus; however, a few patients with oral lichen planus have concomitant genital mucosal lesions. Lichen planus of the male external genitalia commonly involves the glans penis in the form of typical annular lesions. 2 Violaceous flat-topped papules similar to lesions elsewhere in the skin can also occur on the glans and shaft of the penis. They may subsequently coalesce to form arcuate lesions that evolve into rings of clustered papules with central clearing. Fine white streaks, Wickham striae, are usually visible on the surface of the lesions. 3 Genital lesions may also present as erythema, erosions and white patches. 3 Erosive lichen planus with concomitant involvement of genital and oral mucosa is also well known. 4–6 Lichen planus is the most common cause of desquamative vulvitis. 4 In addition, lichen planus of the vulva may result in the formation of urethral stricture; 7,8 however, lesions localized to the urethral meatus in men have not been described previously. In our case, the meatal lesion posed a diagnostic dilemma, yet a careful examination of the oral mucosa led us to consider the diagnosis of lichen planus. Corroborative histopathology of the oral lesion confirmed the clinical diagnosis. Erosive genital disease may pose a diagnostic predicament, especially in sexually active adults. It is, therefore, imperative to consider lichen planus while examining any patient with urinary complaints and/or erosive genital disease. A careful examination of the oral cavity in suspected cases of genital lichen planus may reveal the characteristic lesions and help confirm the diagnosis. The differential diagnoses include pemphigus and pemphigoid. 6 In the diagnosis of mucosal disease, it is crucial to differentiate between erosion and ulcer due to the differences in the differential diagnoses. An erosion is red, superficial and flat (genital herpes and lichen planus) while ulcers are deep, with a palpable loss of tissue and often with a white, fibrinous base (genital herpes in the immunosuppressed patient, chancre, chancroid, aphthae).
A potent topical steroid is the conventional treatment for genital lichen planus. 9 Calcineurin inhibitors 9 and cryosurgery 10 are other therapeutic options. Clobetasol propionate 0.05% gel was found to be effective and well tolerated in the current case, yet irritation may sometimes occur with the gel forms, as they are alcohol based. In that eventuality, ointment base should be substituted. To conclude, lichen planus can rarely affect the urethra, resulting in urinary symptoms, and may present as genital erosion/s, which may masquerade as a sexually transmitted infection.