
Abstract
A 37-year-old HIV-positive Gambian woman presented with spastic weakness of the right leg six years after receiving treatment for tuberculous meningitis (TBM). Magnetic resonance imaging (MRI) of the spine showed a multiloculated syrinx in the thoracic spinal cord extending from the T2 to the T11 level. Syringomyelia and syringobulbia have been reported as complications of TBM. We describe the first case of syringomyelia as an uncommon late complication of treated TBM in the setting of HIV infection. Early recognition of this rare entity may avoid irreversible neurological sequelae.
Keywords
CASE REPORT
A 37-year-old woman of Gambian origin presented to the emergency department in June 2003 with a six-week history of headaches, fever, night sweats, weight loss and diarrhoea. She had been in the UK for 18 months and had not travelled outside the country in that time. Clinical examination revealed fever, oral candidiasis, palpable cervical lymphadenopathy and meningism. Initial investigations showed a normocytic anaemia, lymphopaenia, abnormal liver profile (transaminitis and an elevated alkaline phosphatase) and a raised C-reactive protein. The blood film for malarial parasites was negative. Blood, urine and stool cultures were negative for bacteria.
Chest radiograph at presentation demonstrated widespread tiny nodular shadowing highly suggestive of miliary tuberculosis (TB). Computed tomography (CT) scan of the brain was normal. Cerebrospinal fluid (CSF) analysis showed raised protein, low glucose and a lymphocytic pleocytosis with negative stains for acid-fast bacilli (AFB) and cryptococcus. Bronchial lavage analysis was negative for bacteria, viruses and fungi.
At this stage, she tested HIV-positive and was found to have a baseline CD4 count of 10 cells/mm3 (2%) and a plasma viral load of 7,170,000 copies/mL. A provisional diagnosis of miliary TB with associated tuberculous meningitis (TBM) was made. She was commenced on anti-tuberculous treatment (ATT) with rifampicin, isoniazid, pyrazinamide and ethambutol together with oral corticosteroids. Combination antiretroviral therapy (cART) with zidovudine, lamivudine and ritonavir-boosted lopinavir was commenced. Co-trimoxazole prophylaxis and fluconazole were also initiated.
After two weeks, bronchial lavage and CSF grew Mycobacterium tuberculosis. The isolate was resistant to both isoniazid and streptomycin; hence ATT was modified to include daily ethionamide and ciprofloxacin. The boosted lopinavir was switched to efavirenz to reduce drug–drug interactions.
One month into treatment, she re-presented to the hospital with nausea, dysphagia and poor oral intake. Upper gastrointestinal endoscopy and biopsy revealed invasive herpes simplex virus (HSV) oesophagitis. Treatment was complicated by significant rises in liver transaminases that warranted cessation of the TB therapy and cART. These were re-introduced gradually once the liver profile had improved. The patient remained adherent to all treatments offered. Six months into ATT, the chest radiograph showed complete resolution of the miliary shadowing. At this stage, she developed thoracic back pain without any focal neurological signs. Magnetic resonance imaging (MRI) of the spine revealed an epidural abscess causing irregular cord compression between C7 and T10/T11. The abscess was drained and fluid from the collection was subsequently AFB-negative and culture-negative for mycobacteria. However, the epidural tissue was polymerase chain reaction (PCR)-positive for M. tuberculosis. Her clinical course was further complicated by the development of necrotic abdominal lymphadenopathy which occurred after 10 months of ATT. CT-guided abdominal lymph node biopsy showed granulomatous inflammation consistent with TB and a lymphoma was excluded. It was felt that this represented immune reconstitution inflammatory syndrome to TB as her CD4 count had risen to 140 cells/mm3 with an undetectable plasma HIV viral load. She eventually completed 18 months of TB treatment and CSF was culture negative for TB on two separate occasions. Her cART was simplified to a once-daily combination of tenofovir, emtricitabine and efavirenz.
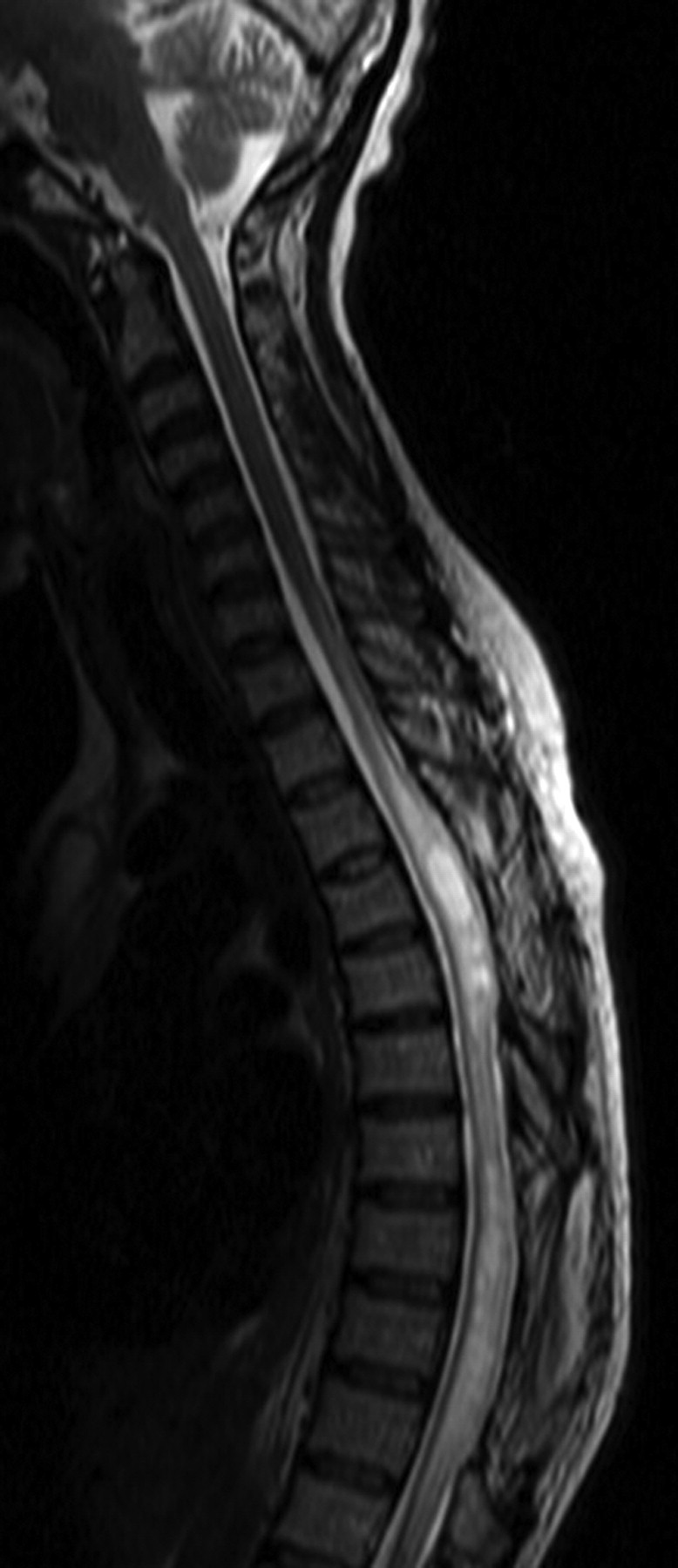
Six years later, she was found to be dragging her right leg at a routine follow-up visit. She had no urinary or bowel symptoms and denied headaches and weight loss. Clinically she had a spastic gait with hypertonia. There was pyramidal distribution of weakness in the lower limbs (MRC grading of power 3/5), more prominent in the right. Lower limb reflexes were brisk with upgoing plantars. There was loss of sensation to pinprick and vibration sense in both feet up to the ankles. On the trunk, sensation to pinprick was diminished on the right side. Upper limb examination was normal except for symmetrical hyperreflexia. A contrast-enhanced MRI of the brain and spine showed an intracranial tuberculoma and a multiloculated syrinx from the T2 to T11 levels (Figures 1 and 2). There was no evidence of an extrinsic compressive lesion or extradural collection and the lack of enhancement excluded the possibility of a tumour.
Axial T2W image at the level of thoracic card showing expansion of the cord with central, altered high signal and cavitation Sagittal T2W image of thoracolumber region demonstrates the extensive, confluent cord signal abnormality
An initial CSF analysis showed small amounts of AFB but subsequent CSF culture and PCR on the culture specimen were negative for TB. This raised some important therapeutic dilemmas. Although it was felt that the development of a syrinx could have resulted from previous TBM, the possibility of re-infection or reactivation could not be excluded. The patient was re-commenced on ATT in conjunction with corticosteroids and neuro-rehabilitation. She was referred to the neurosurgeons who felt that there was no role for immediate surgical intervention and elected to observe the patient clinically with periodic imaging. She has maintained her immune recovery having had a recent CD4 count greater than 600 cells/mm3 and an undetectable plasma HIV viral load. The possibility of switching to a cART regimen with better CNS penetration was considered. However, patient preference for a once-daily regimen and potential for drug interactions with ATT precluded a switch.
DISCUSSION
Syringomyelia, which is characterized by abnormal cavitation of the spinal cord, was first described in TB in 1916. 1 Spinal arachnoiditis occurring during or after TBM is thought to produce an extensive obliterative endarteritis resulting in an ischaemic cord injury and syrinx formation. 2,3 Disturbance of cerebrospinal fluid flow around the spinal cord has an important role in the development of syringomyelia due to spinal arachnoiditis. Previous reports have described syringomyelia both as an early and a late complication of TBM despite effective ATT. 4–7 The duration between the initial episode of meningitis and the onset of neurological symptoms has ranged from less than a year to 20 years in these case reports. To the best of our knowledge, this is the first case of syringomyelia described as a late complication of HIV-associated TBM.
In contrast to previous case reports, this patient developed syringomyelia despite lack of evidence of arachnoiditis both during the initial meningitic episode and on subsequent MR imaging. The possibility of TB re-infection or reactivation was considered. Given that both TB and HIV were adequately treated, the possibility of TB reactivation was considered less likely. The intracranial tuberculoma identified in this patient at the time of diagnosis of syringomyelia could represent a ‘paradoxical reaction’ to the initial ATT. These lesions may develop or worsen due to an enhanced host immune response during ATT. Identification of such lesions after completion of adequate TB treatment does not necessarily indicate treatment failure. 8,9 Treatment of syringomyelia may require insertion of syringo-subarachnoid or syringo-peritoneal shunts 10 and suitability for these procedures in this patient will be considered if the syrinx increased in size during surveillance.
In the wake of the rising TB/HIV pandemic, this case highlights the need to recognize this late but important complication of TBM. As syringomyelia may develop several years after a TBM infection, it should be considered as a differential diagnosis of any unexplained neurological deterioration in co-infected patients. In the absence of arachnoiditis, one should also consider the possibility of reactivation or re-infection of TB. Early detection of this unusual complication may help to prevent the development of irreversible neurological damage.