
Abstract
Bone involvement in secondary and tertiary syphilis is a well-documented but unusual phenomenon. We report the case of an atypical presentation of secondary syphilis in a 25-year-old HIV-positive man who has sex with men. He presented initially with headaches and an unusual calvarial swelling. The skull findings were consistent with osteitis and he later developed systemic symptoms. Treponema pallidum serology was positive and the lesions and systemic symptoms resolved completely after administration of appropriate antibiotic therapy.
INTRODUCTION
The spectrum of clinical manifestations of secondary syphilis is both wide and variable. Several organs are commonly implicated, although bone involvement is uncommon. As the prevalence of syphilis remains high among men who have sex with men (MSM), clinicians must become vigilant for both common and unusual signs and symptoms of treponemal disease.
CASE
A 25-year-old white European MSM was admitted to hospital for investigation of a large discrete left frontal bone swelling of recent onset (Figures 1a and b). He reported a three-week history of generalized headaches preceding the swelling. Two years previously he was diagnosed with HIV and was antiretroviral-naïve with a most recent CD4 count of 627 cells/μL and HIV viral load of 10,936 copies/mL. He reported several episodes of unprotected anal and oral sex with casual male partners in the six-week period before presentation but denied any anogenital or mouth ulceration, anogenital discharge or pain. A routine sexual health screen performed two months prior was negative and Treponema pallidum antibodies were not detected. There was no history of recent foreign travel.
(a) and (b) left-sided frontal swelling – images taken by patient at home. (c) and (d) magnetic resonance images of skull showing soft tissue swelling and irregular lytic bone lesions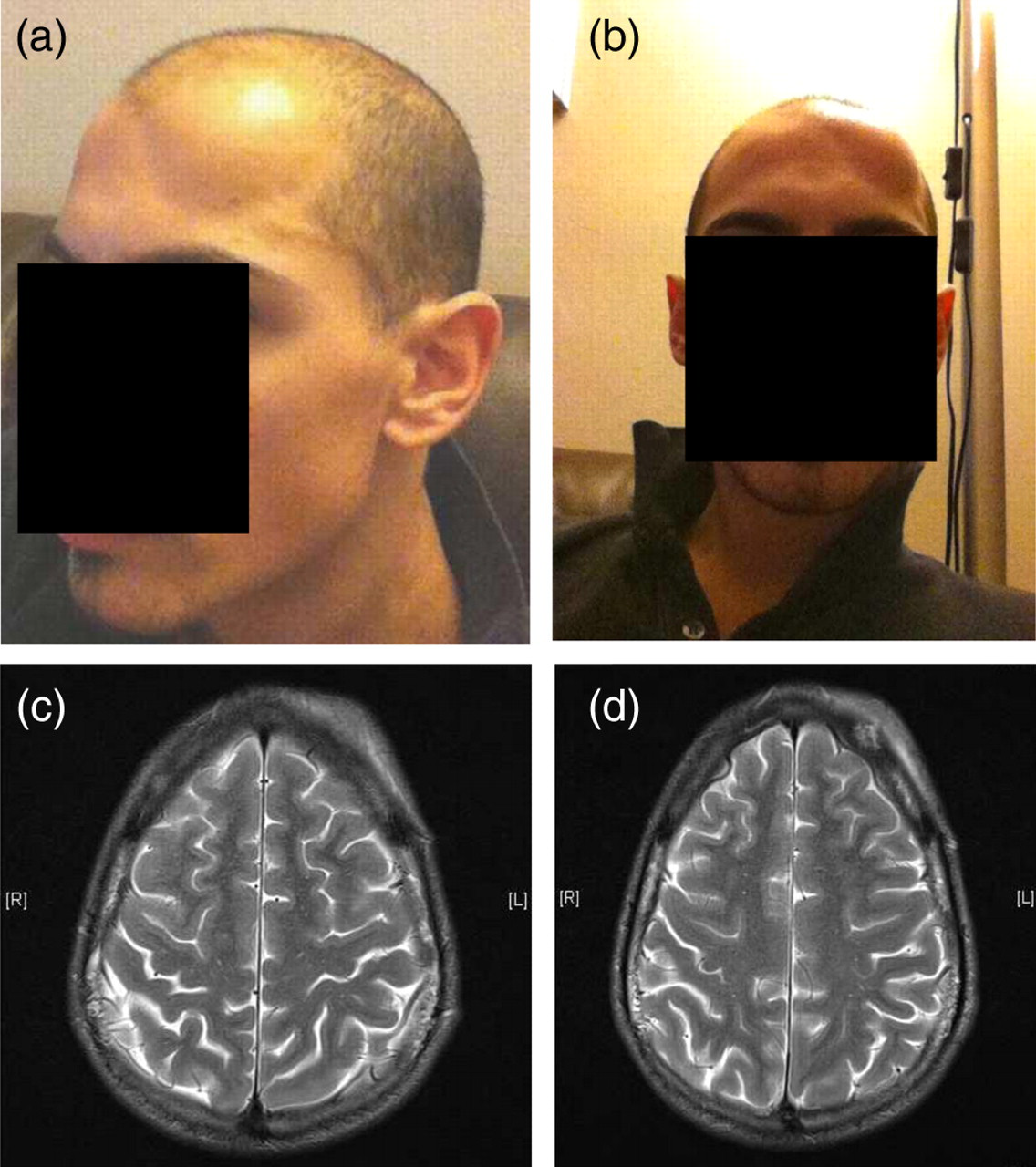
Examination revealed a palpable 4 cm × 6 cm discrete tender fluctuant swelling over the left side of his forehead. No other abnormal signs were elicited and anogenital examination was normal. He was apyrexial and all vital signs were normal. Initial liver biochemistry results were deranged with a raised alkaline phosphatase of 158 IU/L (normal 35–129), alaninine aminotransferase of 161 IU/L (35–129) and γ-glutamyl transferase of 88 IU/L (4–72); his C-reactive protein was 16 mg/L. Full blood count and renal function were within normal limits. Computed tomography (CT) of the head showed soft tissue swelling over the left frontal region and left vertex with underlying irregular lytic bone lesions, findings that were confirmed on magnetic resonance (MR) imaging (Figures 1c and d).
On the fifth day of his admission he became pyrexial and his headaches worsened. A lumbar puncture was performed (opening pressure 12 mm H2O, white blood cell count 1 × 106/L, protein 0.34 g/L [0.00–0.44 g/L], red blood cell count 1 × 106/L, glucose 3.6 mmol/L 1 ) as was a myeloma screen, blood cultures, hepatitis A, B and C and Toxoplasma serology. He was commenced on intravenous co-amoxiclav to cover possible lower respiratory tract infection. Over the next three days his fevers settled, his liver function normalized, the calvarial swelling began to subside and he was discharged.
T. pallidum antibodies (Architect Syphilis TP CLIA, Abbott Diagnostics, Wiesbaden, Germany) were detected on serum taken during his admission, confirmed with T. pallidum particle agglutination assay (TPPA; Serodia, Fujirebio Inc., Tokyo, Japan), and a positive rapid plasma reagin (RPR) with a titre of 1:128. He was subsequently treated with intramuscular benzathine penicillin 2.4 MIU and the residual frontal bone swelling resolved within 48 hours.
DISCUSSION
Bone involvement is common in tertiary and congenital syphilis. In primary and secondary syphilis it is an uncommon phenomenon that can go unnoticed in the presence of more obvious syphilitic manifestations such as mucocutaneous involvement or lymphadenopathy. It is felt that the haematogenous dissemination of spirochetes that occurs following primary infection results in their deposition in the periosteum, Haversian canals and the medullary space of all bones. 2 Spirochetes then induce a perivascular response with production of inflammatory infiltrates and highly cellular granulation tissue. The inflammatory process is ultimately the cause of the periostitis, osteitis or osteomyelitis. The response of bone is dependent on the part of the bone involved, host response and the virulence of the organism. 2,3
In the largest case series to date, Reynolds and Wasserman 4 identified only 15 patients with destructive bone lesions in 10,000 cases of early syphilis from 1919 to 1940.
Thompson and Preston 5 performed skull radiographs on 80 patients with secondary syphilis and found seven with osteolytic lesions, of whom only four had headaches. The most frequent type of bony lesion in early syphilis is a destructive osteitis; osteoperiostitis and osteomyelitis occur less frequently. 6 The skull, clavicular, tibial, fibular, ulnar and radial bones are most frequently affected in osteomyelitis. Syphilitic periostitis tends to affect the long bones in both the arms and the legs – skull involvement is less frequent. 7
In conventional radiographs of syphilitic osteitis, typical findings are of round, osteolytic areas with demineralization or sclerosis of the outer table and diploë. 5
In the two reported cases with MR imaging reports of calvarial skull lesions to date, both demonstrate focal enhancing skull lesions with periosteal and marrow space involvement with adjacent scalp soft tissue abnormality. 1,8
In our patient both the CT and MR imaging findings of the skull were characteristic of early syphilis, showing irregular atypical worm-eaten appearance of osseous destruction with adjacent enhancing soft tissue abnormality. The diagnosis of syphilis was, however, delayed as a result of his recent negative syphilis serology and the absence of mucocutaneous involvement or lymphadenopathy. Partial resolution of his symptoms that occurred with a five-day course of a penicillin-based antibiotic (co-amoxiclav) further obscured the underlying diagnosis that was only revealed to the treating physicians upon receipt of the positive syphilis serology results.
This case illustrates the protean ability of the spirochete to evade the differential diagnosis of even experienced HIV/genitourinary medicine physicians and reminds us that all clinicians should maintain a low threshold for suspecting infectious syphilis in MSM patients, particularly with the recent global re-emergence of the disease. In patients with HIV the threshold of suspicion should be even lower as the clinical presentation may often be atypical or more aggressive. 1