
Abstract
A national Scottish audit of 282 patients with HIV infection attending 11 clinics showed the following levels of performance against quality improvement Scotland Sexual Health Services Standards: syphilis serology was offered in the previous six months to 55% of patients (range: 12–97% of patients in individual clinics), sexual history documented within four weeks of initial HIV diagnosis in 67% (12–100%) and offer of tests for sexually transmitted infections (STIs) documented within four weeks of HIV diagnosis in 45% (4–96%). Considerable variation in performance exists between clinics. The audit prompted interventions to further improve the sexual health care of people living with HIV infection.
INTRODUCTION
The management of the sexual health of people living with HIV is an important part of holistic care for the individual and of an integrated approach to HIV prevention. 1,2 Quality improvement Scotland (QIS) published Sexual Health Standards in March 2008. 3 Genitourinary (GU) medicine infectious diseases (ID) and combined units providing HIV care in Scotland were audited against Standard 5: sexual health care for people living with HIV.
METHOD
Consecutive cases diagnosed with HIV prior to 1 January 2008 and attending for CD4 count monitoring between 1 April and 31 July 2009 were identified from data obtained centrally from Health Protection Scotland. The selection criteria were based on the fact that CD4 count monitoring occurs at a fairly regular frequency of 3–6 months in all units, allowing some standardization of case selection between units, regardless of attendance frequency. A cut-off for date of diagnosis was applied to allow sufficient follow-up to audit the retesting standards. The first 36 cases attending each site (or all where less than 36 attended) during the audit period were selected for audit. There were no predetermined exclusion criteria. A retrospective case-note review on each patient was carried out by a visiting auditor using a questionnaire based on the 2006 BASHH audit 4 questions 5 but modified to incorporate the criteria required for QIS standard 5. Data were transferred to a Microsoft Excel spreadsheet for analysis.
RESULTS
Four ID, eight GU medicine and three combined units were eligible to participate in the audit. Two units were excluded (one had only one eligible patient and the other wished to defer the audit). Data were collected on 282 patients from 13 units.
QIS standard 5.1: 90% of patients have the result of syphilis serology taken within the preceding six months recorded in their HIV records, or documentation why this is not required updated at six-monthly intervals.
Fifty-five percent of all cases had syphilis serology recorded within the last six months (range 12–97%). Four clinics met the standard of 90% (Figure 1). The same four clinics, plus one additional clinic also met the ‘updating’ element of the standard, having tested 90% of patients 6–12 months previously. All clinics achieving the standard did so by testing rather than recording non-offer or decline of testing.
Standard 5.1 – syphilis testing in the past six months. The coloured bars indicate: blue = declined, no reason given; violet = not offered, no reason given; green = declined, reason given; red = not offered, reason given; black = offered and accepted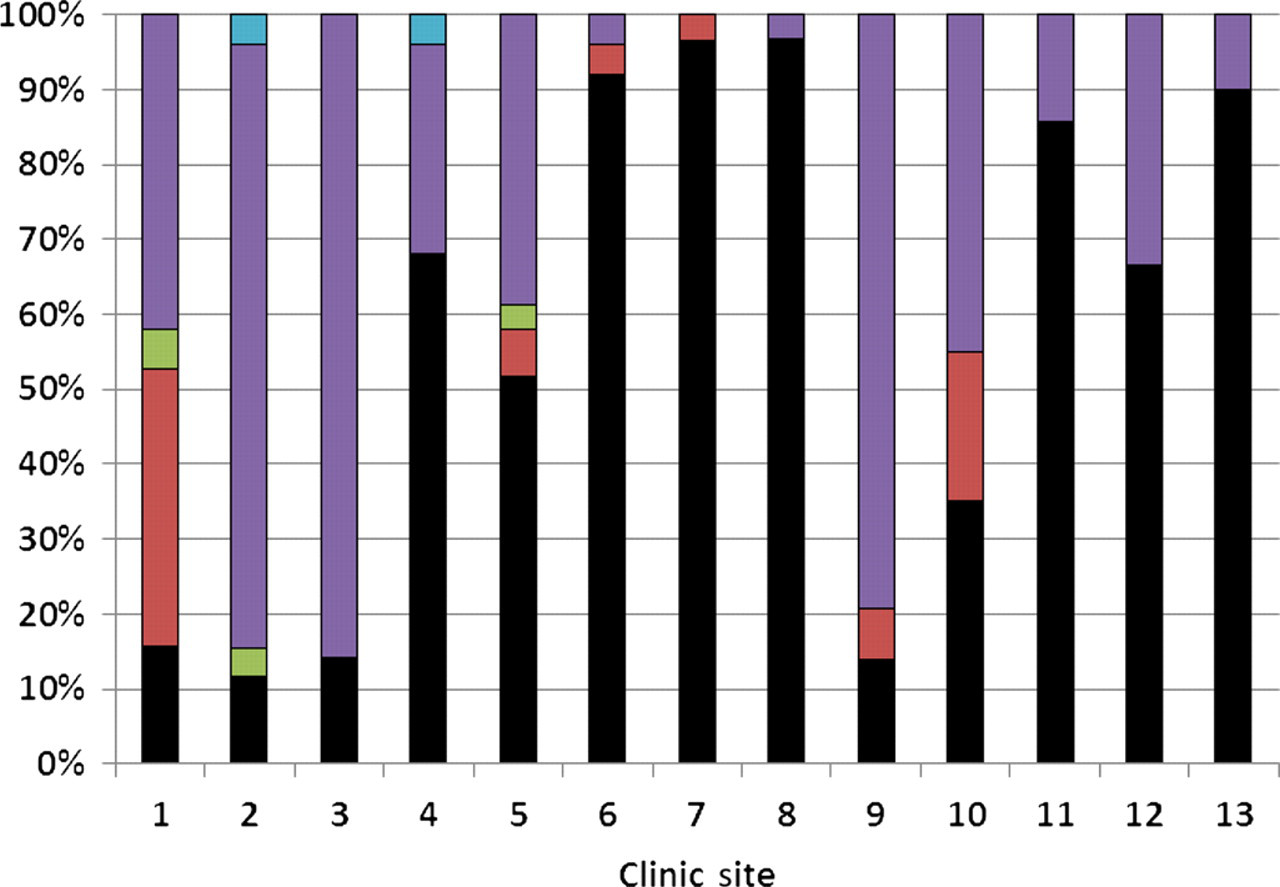
QIS standard 5.2: 80% of HIV-positive adults presenting for the first time in Scotland have their sexual and reproductive history documented within four weeks of their initial HIV diagnosis, and are given advice to prevent onward HIV transmission, backed by the availability of condoms.
Sexual history was recorded within four weeks of diagnosis in 67% of cases. Six units achieved QIS standard of 80% (Figure 2). In a sub-sample of 138 patients diagnosed after 2005, eight clinics achieved the QIS standard. In 51% of cases (range 8–90%) the partner's serostatus was recorded and 45% (range 0–91%) of cases had condom use recorded within four weeks of diagnosis. Only 7% (range 0–57%) were offered and accepted condoms within four weeks of diagnosis.
Standard 5.2 = sexual history and safer sex advice four weeks after diagnosis. The coloured bar indicates: blue = sexual history; red = condom use; green = partner status; violet = condom given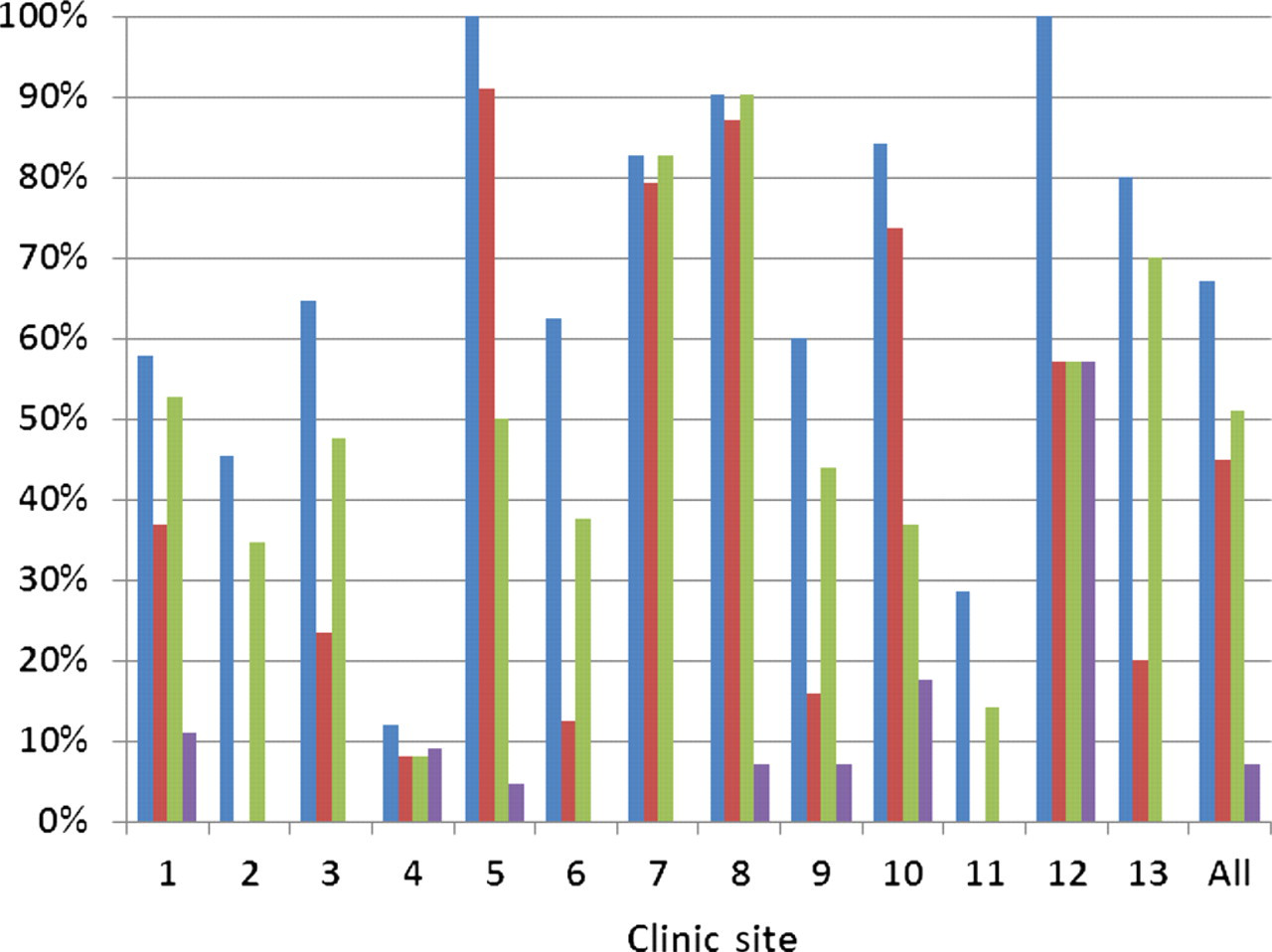
Other audited markers of safer sex interventions included offer and acceptance of condoms: Only 7% (0–57%) were offered and accepted condoms within four weeks of diagnosis, 17% (range 0–100%) in the last six months and 19% (range 0–100%) in the last year. Post-exposure prophylaxis following sexual exposure (PEPSE) was discussed or prescribed in 16% (range 0–53%) in the last year and was not required in 18% (range 0–50%) of cases who had seroconcordant partners.
QIS standard 5.3: 80% of the patients have an offer of a sexual health screen at least once every 12 months. If a sexual health screen is not required or if the offer is declined, this information is documented at 12 monthly intervals.
A total of 45% of cases were offered and accepted a sexually transmitted infection (STI) screen including chlamydia testing within four weeks of diagnosis (range 4–96%), 22% (range 0–100%) in the last six months and 32% (range 0–100%) within the last year. Three clinics met the standard. Recording of the reason for non-offer of chlamydia testing was notably better than for syphilis testing. The audit did not examine testing more than 12 months previously so was not able to provide information on the updating of test offer at 12-monthly intervals.
Contraception and cervical cytology
Contraception and cervical screening were audited against 2007 Joint BHIVA-BASHH-FFP UK SRH guidelines. 1 One pregnant and 89 non-pregnant women were included in the audit. In 38 cases no data were recorded on contraception. Of 51 in whom data were recorded, in 16 cases contraception was recorded as not applicable, 14 not known, two were celibate and five used no contraception. A contraceptive method was recorded for only 13 women.
No data were recorded on cervical cytology in 38 of the 90 women. In 17 cases a cervical smear was recorded as ‘not applicable’, in 11 ‘not known’, five had no smear performed, four had a cervical smear performed at the audited clinic and 15 were performed elsewhere.
CONCLUSIONS
Less than half of all clinics met syphilis testing standards and there was a wide variability in performance. Chlamydia testing and syphilis testing standards were not achieved by the same units; no clinic met both standards. This may be because in some syphilis testing was routinely performed along with HIV monitoring bloods and was not linked to STI testing. There was wide variation in sexual history taking, recording of condom usage and discussion or prescription of PEPSE although this may be partly due to lack of documentation. There was no evidence that performance was dependent on units being run by ID or GU medicine clinicians, or both. Results were presented in detail at Scottish BASHH and Scotland/Scottish HIV and AIDS Group (SHIVAG) meetings, and returned to units with the anonymized dataset and their own individual unit code. The auditors suggested that interventions were required to improve performance and recording in the following areas of practice: offer of sexual health screen; condom offer, acceptance and usage; safe sex and PEPSE advice; cervical cytology and contraception. The findings were used by a number of units in self-assessments for QIS peer review visits in 2011. 6 Several clinics have addressed the findings through the standardization of syphilis test offer, the inclusion on an electronic patient management system of prompts to sexual history taking or STI testing and the inclusion of sexual health parameters in an Integrated Care Pathway.
Footnotes
ACKNOWLEDGEMENTS
We would like to thank all HIV clinicians, medical, nursing and clerical staff in Scottish HIV units, Glenn Codere at HPS, BASHH Scottish branch and SHIVAG members for contributing to the audit. Funding for the audit was provided by BASHH Scotland.