
Abstract
The differential diagnosis in anogenital ulcer-adenopathy syndrome in men who have sex with men (MSM) is becoming more complex, particularly with lymphogranuloma venereum and syphilis re-establishing endemicity among MSM. Sexual contact has been shown to transmit methicillin-resistant Staphylococcus aureus (MRSA), probably through intimate skin-to-skin contact. We present a case of MRSA genital ulceration and local lymphadenopathy in a man whose sexual partners are men, reporting high-risk sexual behaviour, highlighting the importance of also considering MRSA infection in these cases, and the potential for spread of MRSA infection in the MSM community.
Keywords
In recent years, outbreaks of bacterial sexually transmitted infections (STIs) such as lymphogranuloma venereum (LGV)1,2 and syphilis have occurred among men who have sex with men (MSM) in Europe.3,4,5 The differential diagnosis of genital ulcer-adenopathy syndrome in MSM is thus becoming more complex. Sexual contact may be a route of transmission of methicillin-resistant Staphylococcus aureus (MRSA) infection. 6 This may not represent sexual transmission in the classical sense, but may result from intimate skin-to-skin contact. We report a case of MRSA causing a genital lesion with inguinal adenitis in an HIV-positive man whose sexual partners are men, reporting high-risk sexual behaviour. The potential exists for spread of MRSA within the MSM community.
A 32-year-old white British man presented to our London genitourinary (GU) medicine clinic in May 2011 with a history of a tender penile ulcer and right groin pain for one day. He had no other genitourinary, throat, rectal or systemic symptoms. He was sexually active with other men and had been diagnosed with HIV and hepatitis C virus (HCV) since 2000. He had also been treated twice in the past for early syphilis infection with benzathine penicillin injections. He had commenced antiretroviral therapy over nine years ago, but had had some unplanned treatment interruptions. He was taking tenofovir/emtricitabine, atazanavir and ritonavir once daily (restarted a year ago after a treatment interruption), and his surrogate markers two months prior showed a CD4 lymphocyte count of 358 cells/μL (26%) and HIV viral load (VL) of 184 copies/mL. He had a past history of intravenous drug use but last injected several years ago. He had never received treatment for HCV, and remained RNA-positive with a HCV VL of 3 million IU/mL 17 months prior.
He reported recent unprotected receptive and insertive anal and oral sex, insertive fisting and receptive sex toy use with multiple HIV and HCV co-infected partners at a sex party three days prior to presentation; he mentioned that one of these contacts had multiple skin sores over his back. He also underwent ‘suspension’ at this party: a practice that involved the use of multiple metal hooks inserted under the skin of his lower limbs for the purposes of hanging him in mid-air. He gave no history of travel outside of the UK in the last six months.
On examination, there was a single tender 1 × 1 cm ulcer on the base of the ventral penis that was moderately indurated; on close inspection it had a honey-coloured crust and pustular edge (Figures la and b). He also had an exquisitely tender enlarged right inguinal lymph node (LN). There was no urethral discharge, and the rest of the anogenital examination was normal.

(a) Tender ulcer (1 cm × 1 cm) at base of ventral penis, (b) Close-up view of penile ulcer
The differential diagnosis included pyogenic ulcer with adenitis, LGV ulcer with adenopathy/bubo, primary syphilis and genital herpes, with possible secondary bacterial infection of the latter three. The ulcer was cleansed with sterile saline solution and two samples obtained for darkfield microscopy; both were negative. Swab samples were then taken from the ulcer for Gram stain, bacterial culture, herpes simplex virus DNA polymerase chain reaction and Chlamydia trachomatis (CT) RNA (Aptima Combo2 [AC2], Gen-Probe Inc, San Diego, CA, USA). Suspecting LGV adenitis, a fine-needle aspiration of the inguinal LN was performed aseptically, and 0.5 mL brown purulent exudate was obtained. Gram stain of the ulcer swab and the LN aspirate showed a dense neutrophil and lymphoid cell infiltrate with many clusters of Gram-positive cocci (GPC; Figure 2). Urethral Gram stain showed >10 polymorphs/high-power field, but no intracellular Gram-negative diplococci. In addition to the penile ulcer and inguinal LN aspirate material, urine, and rectal and pharyngeal swabs were also obtained for CT and Neisseria gonorrhoeae (GC) RNA testing using AC2, as well as for Neisserial culture on a selective medium containing vancomycin, colistin, amphotericin and trimethoprim (VCAT; Oxoid Ltd, Cambridge, UK). In addition to darkfield examination, syphilis serology was performed for Treponema pallidum antibodies (Architect Chemiluminescence Immunoassay, Abbott Laboratories, Abbott Park, IL, USA) and rapid plasma reagin (RPR).
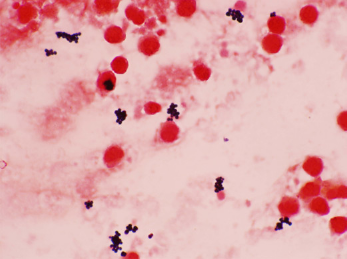
Gram stain of inguinal lymph node aspirate demonstrating clustered Gram-positive cocci among lymphoid cells and neutrophils
A provisional diagnosis was made of a pyogenic ulcer secondary to S. aureus with local adenitis/LN abscess as well as non-gonococcal urethritis (NGU). He was treated with flucloxacillin 500 mg four times daily orally for one week as per the hospital's guidelines for antimicrobial management of skin and soft tissue (SST) infections, as well as azithromycin 1 g stat, to be repeated after 48 hours in order to cover NGU as well as initial cover for possible LGV infection. The patient initially declined doxycycline therapy due to previous gastrointestinal side-effects with this drug, so azithromycin was given, although this regimen for treatment of LGV is not recommended by most authorities.7,8,9
The results for all CT, GC and HSV tests were negative. Serology for syphilis showed positive treponemal antibodies but RPR was negative, consistent with known past treated syphilis (although new primary syphilis infection could not be excluded at this stage). Methicillin-resistant S. aureus (MRSA) was isolated from the swab from the ulcer and the LN aspirate; extended sensitivities showed resistance to penicillin, ciprofloxacin and erythromycin, and sensitivity to gentamicin, vancomycin, fusidic acid, tetracycline, linezolid, rifampicin, mupirocin and trimethoprim.
He was reviewed five days later with these results and no improvement was seen in the inguinal swelling and pain, although the penile ulcer had slightly diminished in size. He was treated for MRSA with dual therapy (prior to availability of final sensitivity results) as advised by the microbiology team with doxycycline 100 mg two times daily and trimethoprim 200 mg two times daily for seven days. His symptoms had resolved completely at his next review 10 days later.
Discussion
MRSA was previously considered to be primarily a hospital-acquired pathogen, but is now recognized as a pathogen in the general community. A cross-sectional study in Toronto, Canada, found the prevalence of community acquired MRSA (CA-MRSA) colonization in MSM to be 1.6% (95% confidence interval [CI]: 0.5–2.6) 10 and outbreaks of a dominant clone of CA-MRSA (USA300) infections in MSM have been reported in San Francisco (relative risk 12.8 [95% CI: 1.8–91.3]), 6 although others have observed no increased prevalence of MRSA among MSM. 11 HIV infection did not appear to be independently associated with that specific strain of MRSA, 6 although spread among MSM has been associated with high-risk behaviour, including the use of methamphetamine and other illicit drugs, sex with multiple partners, participation in group sex parties, use of the Internet for sexual contacts and history of STIs. 12 A recent cross-sectional study among HIV-infected MSM found that MRSA carriage was associated with a history of a recent STI in the preceding year, including syphilis, and with the use of saunas. 13 Clinical manifestations have included SST infections of the buttocks, genitals and the perineum. 6 CA-MRSA infections can progress to necrotizing fasciitis of the genitoperineal region (Fournier gangrene). 14 About 1% of HIV-infected MSM had MRSA colonization identified in the perigenital area; only 50% of these were colonized nasally, suggesting that MRSA carriage may be missed on traditional nasal screening in this group of patients. 13
In current clinical practice, STIs such as herpes, syphilis and LGV should be included in the differential diagnosis of ulcer-adenopathy syndrome in western MSM. This case alerts clinicians that S. aureus, including MRSA strains, can also present with similar clinical manifestations, and such infections should be actively sought with relevant investigations, including LN aspiration where clinical uncertainty exists. In the present case, LGV with classical genital ulcer and bubo was considered to be the likely initial diagnosis prior to the Gram stain result. Although the typical presentation of LGV in MSM is that of proctitis, a small but significant number of inguinogenital cases of LGV has been observed in MSM in London. 15 However, initial empirical treatment was guided by the presence of GPC on the LN aspirate. Given the isolation of MRSA from the lesions, doxycycline therapy would have provided superior cover for both infections. The UK recommended treatment for uncomplicated soft tissue MRSA infections is doxycycline, 16 although dual therapy was initially advised until final sensitivities were determined. The prevalence of MRSA in MSM could have implications for empiric treatment of skin infections in these patients. Increasing rates of CA-MRSA infection have been reported in HIV-infected individuals, with a predilection for buttock and scrotal infection. 17
It is not clear whether penetrative anal sex, and therefore dissemination of perirectal carriage of CA-MRSA, potentiates these infections among MSM or whether they are due to skin-abrading sexual practices, or increased frequency of intimate skin-to-skin contact. Potential for MRSA colonization within the MSM population provides yet another reason to advise caution regarding high-risk sexual and piercing practices.