
Abstract
Laboratory tests can be misleading for the diagnosis of syphilis and false-negative results are possible, but it is rare for both treponemal and non-treponemal tests to prove negative in different stages of the disease. We report on a case of luetic lymphadenopathy, diagnosed by histological examination and supported by immunohistochemical staining for Treponema pallidum, in the absence of skin lesions and positive serology. This case reminds us of how syphilis may present in many different clinical forms and that it should not be excluded only on the basis of negative serological tests. This patient's negative serology was probably due to inadequate initial antibiotic therapy. Given the current widespread use of antibiotics, greater consideration is warranted of the extent to which serological test results are modified by non-specific antibiotic therapies.
CASE REPORT
INTRODUCTION
Syphilis is a worldwide problem with approximately 12 million new cases annually 1 and should be considered in the differential diagnosis of lymphadenopathy. Laboratory tests can be misleading for its diagnosis and false-negative results are possible.
We report here on a case of a 46-year-old man presenting with multiple, bilateral, indolent, inguinal lymph node enlargements of unknown origin. Despite several courses of various antibiotics, including oral cephalosporin, lymphadenopathy had persisted. Serology tests for HIV, hepatitis B and C, Toxoplasma gondii and syphilis, including both Treponema pallidum haemagglutination assay (TPHA) and Venereal Disease Research Laboratory (VDRL) assays, were negative two weeks before the first antibiotic prescription and in two other tests repeated both three and six months later. Eight months after the onset of the lymphadenopathy the patient underwent a surgical excision of the three largest lymph nodes in order to exclude malignancy. The histological examination revealed a reactive lymphadenitis with a granulomatous infiltrate consisting of macrophages and epithelioid elements. Mast cells, lymphocytes and several neutrophils and eosinophils were also present. The patient was then reassured, but no specific diagnosis or treatment was given.
Five years later, the patient was referred to our unit from the transfusion centre of our hospital to investigate his positive serology for syphilis. His TPHA (titre 1:5120) and total anti-T. pallidum antibodies (enzyme immunoassay) were positive, whereas immunoglobulin M (enzyme immunoassay) and VDRL were negative. The patient had been donating blood for the previous two years with a negative VDRL performed as the only screening test. He denied having ever had any prior mucocutaneous lesions compatible with syphilis. Physical examination was normal except for some small volume inguinal lymphadenopathy. After careful investigation we learnt that a few months after having unprotected sex with a sex worker he had started suffering from bilateral inguinal lymphadenopathy, which had progressively decreased in volume with time. In view of a possible T. pallidum infection, the histological specimens of the lymph node excisions performed five years earlier were re-evaluated, and revealed the presence of plasma cells and capillary endothelial hyperplasia in addition to the chronic granulomatous lymphadenitis.
Immunohistochemistry for T. pallidum (1439–9406 polyclonal antibody; Serotec, Kidlington, Oxford, UK) performed in paraffin-embedded sections, revealed abundant spirochaetes (Figure 1), allowing us to confirm the diagnosis of latent late syphilis. Benzathine penicillin G (2.4 million units intramuscular once weekly for 3 weeks) was administered with a progressive decrease of lymphadenopathy and TPHA titre.
Immunohistochemistry for Treponema pallidum (performed using a rabbit polyclonal antibody [Serotec 1439–9406] at dilution 1/2000) reveals large numbers of spirochaetes in the lymphoid tissue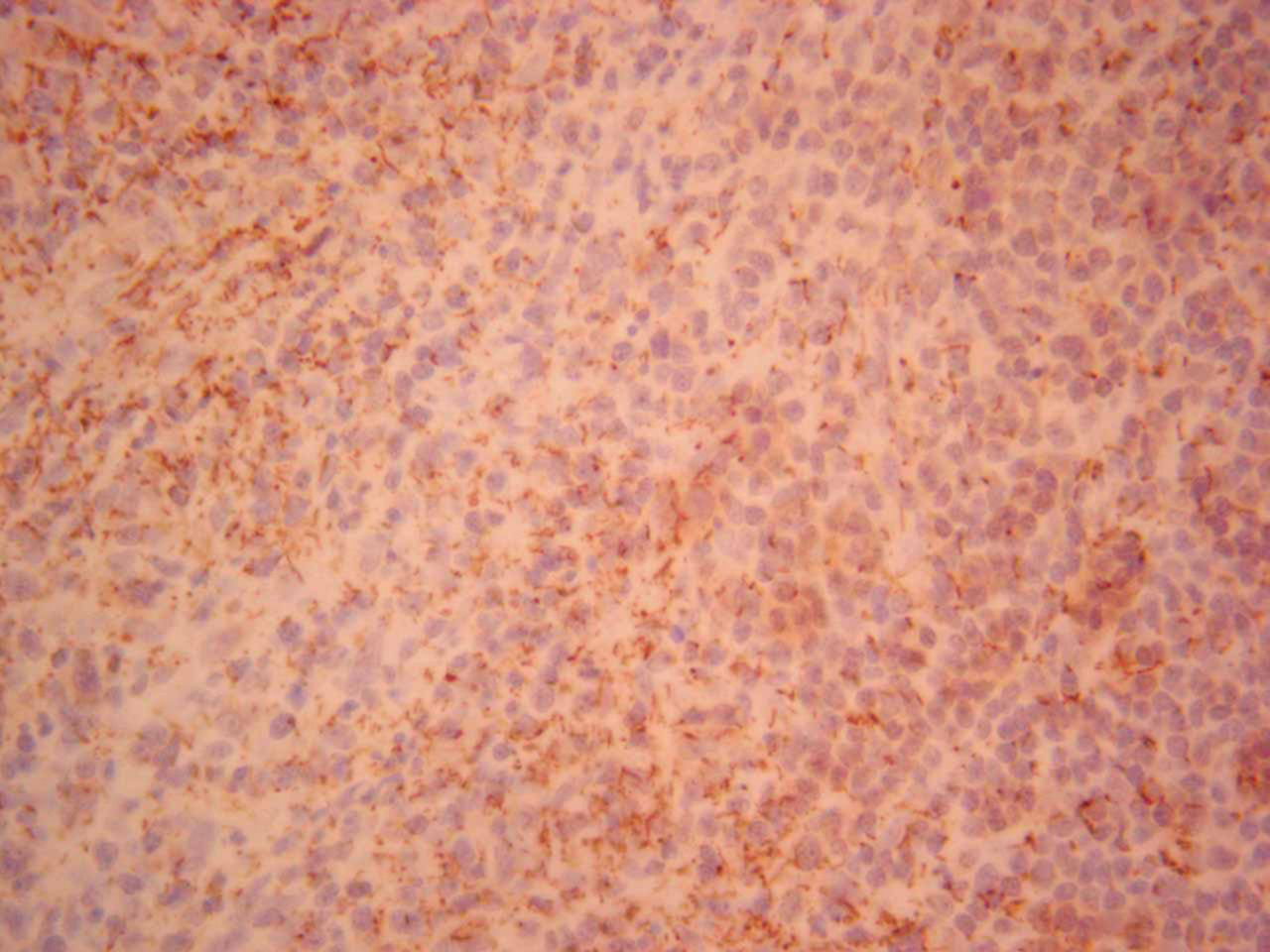
Granulomatous lymphadenitis is a morphological category that describes any, including infectious and non-infectious diseases, in which epithelioid granulomas are found in lymph nodes. In infectious granulomatous lymphadenitis, the aetiology can be confirmed by identifying the pathogen in the nodal tissue employing different methods (culture, polymerase chain reaction and immunohistochemistry) or staining paraffin sections to highlight the microorganism.
Although in our case the presence of a granulomatous infiltrate rich in macrophages and epithelioid elements, as well as of eosinophils, could suggest a luetic aetiology of the inguinal lymphadenopathy, we felt this possibility had been excluded based on the negative serology tests. We should also stress that, although not reported in the first histopathological description, plasma cells and capillary endothelial hyperplasia should be investigated because they can provide valuable clues for the diagnosis of syphilis.
T. pallidum can be responsible for persistent and typically indolent inguinal lymph node enlargement during the primary infection, whereas in later stages lymphadenopathy is usually generalized and frequently associated with systemic symptoms. In our patient, lymphadenopathy was always confined to the inguinal region and it has been the only sign of a luetic infection, given that there was absence of mucocutaneous lesions or positive serology.
However, the absence of any mucous lesions could also be explained by the peculiarity of the chancre of primary syphilis, which classically presents as a single, painless and small nodule that spontaneously heals without sequelae and can go unnoticed.
The serology for syphilis may be negative in the first days following the infection or even in the subsequent stages of the disease, although it is exceptional for both non-treponemal and treponemal tests to prove repeatedly negative. 2 There are descriptions of primary and secondary syphilis with negative non-treponemal and treponemal tests in patients with HIV infection or common variable immunodeficiency, but our patient was not immunocompromised. 3,4 Non-treponemal tests can be falsely negative due to the prozone phenomenon, 5 but in our case an inappropriate antibiotic regimen may have masked the symptoms and produced a false-negative serology result. McKenna et al. 6 found that abusive use of antibiotics is typical of subjects exposed to sexually transmitted infections, with often subcurative doses rendering the syphilis serology negative.
In conclusion, we emphasize that, given the steady increase of syphilis in recent years, this condition should be suspected in cases of granulomatous lymphadenopathy, regardless of the absence of skin lesions or positive early serology results. Given the current widespread use of antibiotics for the treatment of a multitude of infections and symptoms, greater consideration should be given to the extent to which serological test results are modified by non-specific antibiotic therapies.
Footnotes
ACKNOWLEDGEMENTS
We sincerely thank Carla Carli (Department of Pathology, University of Genoa) and Paola Stura (Transfusion Centre, San Martino Hospital, Genoa) for their precious contribution.