
Abstract
The smoking behaviour of persons living with HIV/AIDS in sub-Saharan Africa is poorly documented. We employed a cross-sectional study design to assess the prevalence and predictors of tobacco smoking among HIV-infected patients in northern Nigeria (n = 296). Approximately one quarter of respondents were either current (7.8%) or ex-smokers (17.9%). Smoking rates among HIV-infected women were extremely low. HIV-infected men were at least three times as likely to smoke as their female counterparts living with HIV: adjusted odds ratio (AOR) 3.16, 95% confidence interval (95% CI) 2.17-7.32. Patients with tertiary education were at least twice as likely to smoke compared with their counterparts without formal education (AOR 2.63, 95% CI 1.08-6.67). The preponderance of cigarette smoking among educated HIV-infected men in northern Nigeria offers a unique opportunity for targeted smoking cessation programmes.
Introduction
Three decades into the HIV/AIDS epidemic and with an estimated 33.3 million people currently living with the infection worldwide, this scourge remains one of the most challenging health crises of our generation. 1 With the availability of combination antiretroviral treatment (cART), persons with HIV/AIDS are now living longer, even in resource-poor countries like Nigeria. However, tobacco smoking is threatening to reverse these gains. The World Health Organization (WHO) estimates that about 1.3 billion people smoke tobacco worldwide, leading to 3 million deaths annually (projected to increase to 10 million by 2030). 2
There is a striking correlation between smoking and increased mortality among HIV-infected persons. 3 Smoking among persons with HIV increases the risk of death due to cardiovascular disease, pulmonary disease and non-HIV-related malignancy. 4 Smoking also weakens the immune system, thereby increasing the risk of certain infections, including bacterial pneumonia. 5 Further, HIV-positive patients who smoke have an increased risk of oral candidiasis 6 and Pneumocystis jiroveci pneumonia. 7 Smoking can also increase the incidence of tuberculosis (TB) in HIV-infected persons, 8 which is of particular concern in high TB burden countries, such as Nigeria. Smoking accelerates the progression from HIV infection to AIDS and increases the risk of adverse effects associated with antiretroviral drugs. For instance, the incidence of myocardial infarction has been shown to increase following cART in a large prospective cohort of HIV-positive smokers. 9
The prevalence of smoking among persons living with HIV/AIDS has been reported from West Africa, including parts of Nigeria9,10 but no reports exist from Kano, the most populous city in northern Nigeria. The aim of this study is to assess the prevalence and correlates of cigarette smoking among HIV-infected persons attending Aminu Kano Teaching Hospital (AKTH), Kano. This study could yield important baseline information that could guide the development of targeted health education and smoking cessation programmes and thereby positively impact health outcomes among these patients.
Methods
Setting
AKTH is a 500-bed tertiary hospital located in Kano, the largest urban centre in northern Nigeria. The hospital receives patients from Kano, from neighbouring states and from across the border in Niger Republic. AKTH operates a multidisciplinary, specialist clinic for HIV/AIDS patients five days a week. Clinical examinations and antiretroviral drugs are provided free of charge to all patients. Patient support groups, counselling, testing and home-based care services are also provided. On average, 70 patients attend the clinic each working day.
Study design and population
We employed a cross-sectional study design. The study population consisted of HIV/AIDS patients attending the HIV/AIDS specialist clinic at AKTH from 1-30 May 2011. A systematic sampling technique was used. All men and women with HIV infection with at least one clinic visit were included in the study (whether on cART or not). Those clients that were too ill to participate in an interview were excluded from the study. Based on the average daily attendance at the clinic, a sampling interval was determined. The first respondent was determined by picking a random number between one and the sampling interval. Subsequent respondents were identified by adding the sampling interval to the preceding respondent's serial number. Participants were assured of confidentiality and informed consent was obtained in English and Hausa, the predominant local language. Participation in the study was voluntary. No incentives were provided to participants. Ethical clearance was obtained from the AKTH Institutional Review Board.
Sample size determination
A sample size of 300 was obtained using Fisher's formula. 11 This was chosen to ensure a precise estimate of the prevalence of smoking among HIV-positive patients. The reported prevalence of 22.1% among a similar cohort in northeast Nigeria was used, in addition to a 95% confidence limit, 5% margin of error and allowance for 10% non-response. 9
Study instrument and data collection
A pretested structured interviewer-administered questionnaire containing open and closed ended questions was used. The questionnaire was adapted from an earlier West African study. 10 The questionnaire included questions on sociodemographic characteristics, HIV diagnosis and treatment, tobacco smoking, attempts at cessation, reasons for smoking, knowledge of deleterious effects of smoking, change in smoking patterns on HIV diagnosis, use of cannabis and other substances. The adapted questionnaire was piloted at the nearby Murtala Mohammed Specialist Hospital, Kano where 20 patients (10 men and 10 women) were interviewed to assess the clarity of questions. The findings from this validation process did not form part of this study. For the main study at AKTH, interviews were conducted on a systematic sample of patients attending the antiretroviral therapy (ART) clinic (although not all the patients had been commenced on ART. Additional information about patients’ clinical characteristics (baseline CD4, WHO staging, cART, smoking status and counselling) was obtained from their case files. Four medical students specifically trained in the conduct of interviews collected data. The authors supervised the data collection process.
Data analysis
The data from the questionnaires and case files were entered and analysed using SPSS version 16. 12 Odds ratios (ORs) and 95% confidence intervals (CIs) were used to determine the strength of association of different factors with smoking. Logistic regression analysis was used to adjust for the effect of predictor variables that were significantly related to the outcome variable at the bivariate level. All tests of hypothesis were two-tailed with a type 1 error rate fixed at 5%.
Results
Four patients were excluded on the basis of severe ill health (3 patients with diarrhoea and 1 with high-grade fever). Of the 300 patients sampled for study, 296 agreed to participate, a response rate of 98.7%. Two hundred and twelve patients (71.6%) were men and 84 (28.4%) were women (gender ratio of 2.5:1). The mean age (± standard deviation [SD]) was 37.5 ± 9.1 years. The average age (± SD) of the male and female respondents, respectively, was 40.5 (± 8.3) and 29.8 (±6.3) years (P < 0.001). Approximately 62% of the patients were aged between 30 and 50 years. Fifty-three patients (18.0%) were employed privately or by the government, while 98 (33.1%) were unemployed. The remainder (145; 48.9%) were self-employed. Seventy-five patients (25.3%) had tertiary education, 103 (34.7%) had secondary school education, 60 (20.3%) had primary school education and the rest (19.6%, n = 58) had no formal education. Although a higher proportion of male respondents had tertiary education, this gender difference was not statistically significant (P > 0.05).
At presentation, 85 (28.7%), 41 (13.9%), 57 (19.3%) and 113 (38.1%) patients were in WHO AIDS stage I, II, III and IV, respectively. The median baseline CD4 count was 237 cells/μL (interquartile range: 128-393 cells/μL). About one-third of patients (34.5%) had a baseline CD4 count of <200 cells/μL, 46.0% between 200 and 599 and 19% greater than 600. The duration since HIV diagnosis ranged from 3 months to 13 years. Of the 296 respondents, 269 (90.9%) were on cART.
Out of the 296 respondents, 23 (7.8%) reported that they were current smokers, 53 (17.9%) were ex-smokers and the rest 220 (74.3%) denied ever smoking. When stratified by sociodemographic and clinical characteristics, smoking behaviour varied by gender, age and level of education. Specifically, a significantly higher proportion of men smoked cigarettes compared with female respondents: 10.8% of men were current smokers versus 0% of women (P<0.05). An increasing trend in smoking prevalence was observed among older respondents compared with their younger counterparts (P < 0.05). Further, smoking habit increased with the level of education of respondents (P < 0.05). However, WHO clinical stage, CD4 count, duration since HIV diagnosis and being on cART did not significantly affect the prevalence of cigarette smoking (Table 1). For all smokers, the mean age ± SD at commencement of smoking was 20.5 ± 6.1 years. In current smokers, the number of cigarettes smoked per day ranged from 1 to 40 with a median of 10. Only 161 of the 296 respondents (54.4%) indicated that they were counselled about the dangers of smoking and the need for smoking cessation during their initial or subsequent evaluations at the clinic. At HIV diagnosis, 42 of the 296 (14.2%) respondents were smokers. After HIV diagnosis, 34 of them (80.9%) attempted to quit with 23 out of the 34 (67.6%) quitting successfully. The proportion of smokers therefore dropped from 14.2% to 7.8%. This change was statistically significant (McNemar's χ2 P < 0.05).
Sociodemographic and clinical factors associated with tobacco smoking among HIV-positive patients, Aminu Kano Teaching Hospital, Kano, 2011 (n = 296)
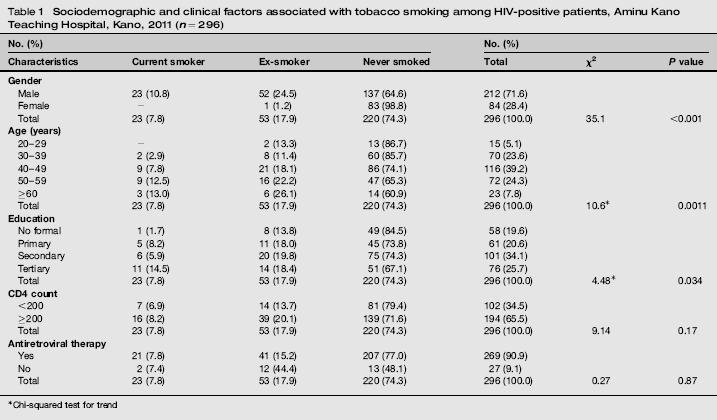
Chi-squared test for trend
Only two of the factors associated with cigarette smoking at the bivariate level remained significant predictors of smoking after adjusting for confounding using multivariate analysis. Specifically, there was a more than three-fold increased risk of smoking among men compared with women (adjusted odds ratio [AOR] [95% CI] =3.16 [2.17-7.32]. Patients who had tertiary education were also more than twice as likely to have smoked compared with their counterparts without formal education (Table 2).
Predictors of tobacco smoking among HIV-positive patients attending Aminu Kano Teaching Hospital, Kano, Nigeria, 2011
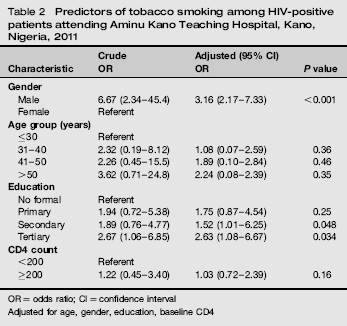
OR = odds ratio; CI = confidence interval
Adjusted for age, gender, education, baseline CD4
Discussion
The prevalence of tobacco smoking among HIV-infected patients attending AKTH was found to be 7.8%. This rate is substantially lower than figures reported from northeast Nigeria (22.1 %) 9 and other parts of West Africa. 10 Specifically, the prevalence of smoking among men in this study (10.8%) was lower than the numbers reported from similar cohorts in Mali (29.7%) and Cote d'Ivoire (14.2%), but higher than figures from Benin republic (2.9%). The zero prevalence among women in our sample replicated findings from Benin republic and was lower than statistics from Mali (1.4%). The proportion of ex-smokers among HIV-infected patients in this report (26%) was also lower than the figure (46.2%) obtained in the West African study alluded to above. 10 These differences could be due to baseline differences in the smoking habits of the general populace from which the subpopulation of HIV-infected persons are derived. For instance, the prevalence of smoking among the general populace in northeast Nigeria 13 and in Cote d'Ivoire has been reported to be (45.3% in men and 8.4% in women) and (11.2% in men and 0.7% in women), respectively. 10 Reasons given for smoking by participants were similar to those elicited in other studies.9,10,14
The zero prevalence of smoking among women in our sample is not surprising considering the cultural situation of women in the study location. In the study conducted in north east Nigeria, 9 45.3% of men and 18.4% of women smoked cigarettes. The mean age at smoking debut was also comparable with the figure reported from the same study (18.6 ± 5) years. 9 The intensity of smoking as indicated by number of cigarettes per day was relatively lower in our study participants compared with HIV-infected persons in other parts of Nigeria 3 and the world.15-17 The predictors of smoking among our respondents have also been observed in earlier studies.9,16
The high proportion of respondents that changed their smoking pattern may reflect the realization that smoking is unhealthy, regardless of serostatus. This finding may not be entirely due to counselling received after HIV diagnosis as demonstrated by the low reported tobacco counselling rate. However, healthy living messages provided during clinic visits could have contributed to the moderately high level of awareness of risks and dangers associated with smoking among HIV-positive individuals. A high proportion of the respondents indicated their intention to quit smoking, which is consistent with findings from other parts of Africa. 18 Since a high proportion of HIV-infected smokers want to quit, then it makes sense to have smoking cessation interventions integrated into HIV care services. Findings from South Africa indicate that preferred cessation strategies among HIV-infected clients include counselling and nicotine replacement. 18 Health-care providers in HIV clinics could therefore be trained in smoking cessation, an approach that has been shown to be effective in increasing cessation rates and reducing relapses. 19 Existing evidence supports the feasibility of smoking cessation, even within busy HIV clinic practices. 20 The effectiveness of counselling plus nicotine replacement therapy in increasing smoking cessation and decreasing tobacco use in HIV-positive smokers is also well-documented.21,22 Vidrine et al. 23 suggest that tailored, intensive interventions may be effective for short-term smoking cessation in HIV-positive persons. The fact that most of these studies were conducted in developed country settings does not detract from the relevance of the findings and the need to test the effectiveness of these interventions in resource-limited settings.
This study has at least two limitations. First is the limited generalizability of our findings. Our study was based on a sample of patients attending a HIV treatment clinic in a large urban tertiary hospital in northern Nigeria. The respondents’ characteristics and smoking habits may differ from HIV-infected persons in the general population, other parts of Nigeria or living in rural areas. Secondly, when enquiring about social behaviour, questions may elicit only desirable responses. However, our interviewers assured respondents of confidentiality prior to the conduct of the interview. These limitations necessitate the need for caution in extrapolating our findings to all HIV-positive persons in northern Nigeria.
In conclusion, the level of smoking among HIV-infected patients attending AKTH is low, relative to similar cohorts elsewhere. Nevertheless, the preponderance of cigarette smoking among educated men in this cohort provides a unique opportunity for targeted smoking cessation interventions. HIV clinics and providers are uniquely positioned to provide such interventions. Clinic visits provide an opportunity to reach smokers with smoking cessation interventions who are already receiving care for their HIV infection. The interdisciplinary treatment model of HIV care programmes, in which case management, counselling, nursing and medical treatment are co-located, is an ideal setting for the delivery of these interventions. These efforts should be supported by a general strategy to discourage smoking among the general populace through legislation, pricing, taxation and restriction of smoking from public places.