
Abstract
The aim of this revision is to evaluate ethnicity and gender rate of enrolment in registrative clinical trials of the protease inhibitors (Pis) from 1996 to 2009. Company-sponsored, phase II or III registrative clinical trials of PIs were evaluated. Forty-nine clinical trials were included. Clinical trials were conducted in centres in North America (n = 39), Central-South America (n = 22), Europe (n = 22), Africa (n = 8), Asia (n = 5), Australia (n = 10). Overall mean age was 39.6 years; median proportion of women was 16.3%. The most represented ethnic group was Caucasian. A test for trend over time (1996-2009) shows a significant increase in the proportion of women included (P = 0.012), and a decrease in the proportion of Caucasians included, reaching borderline significance (P = 0.061). An inverse correlation was observed between the proportion of Caucasians and that of women enrolled in each study (r = 0.65, P < 0.0001). Women were less likely to be included in double-blind studies (11.2% versus 17%, P = 0.019). Clinical trials for treatment-naive subjects were more likely to enrol ethnicities other than Caucasian compared with Caucasian (44.7% versus 27.1 %, respectively, P = 0.04). Rates of enrolment of minorities in registrative clinical trials for PIs show a positive trend since 1996, mirroring the growing number of people of different ethnic groups accessing ART.
Background
The generalizability of results is a prerequisite of a clinical trial. In fact the results of a research should be applicable to the heterogeneous patient population, in terms of race, gender, age and other sociodemographic factors. 1 According to these observations, a US Food and Drug Administration (FDA) requirement is that women and minorities be adequately represented in registrative trials.1-4
In case of HIV infection, this issue is particularly relevant, since persons living with HIV infection are variegated and spread throughout the world. Of the 33 million people estimated by World Health Organization (WHO) living with HIV, the majority was born in the developing world; sub-Saharan Africa has roughly 70% of all people living with HIV; an estimated five million people were living with HIV in 2008 in Asia, and two million in Central-South America. Moreover, according to WHO data women account for half of all people living with HIV worldwide (http://www.who.int/gho/hiv/en/).
Registrative trials are mainly conducted in high-income countries, and representation of populations from low- and middle-income countries and women is frequently suboptimal; therefore, clinical trials are usually underpowered for ethnicity and gender comparisons due to low rates of enrolment of women and other than Caucasian patients.5,6
The aim of this review is to evaluate ethnicity and gender rates of enrolment in phase II and III registrative clinical trials of the HIV protease inhibitors (PIs) from 1996 to 2009.
Methods
For the literature search, we followed the QUORUM guidelines on search strategy. 7
Company-sponsored, phase II or III registrative clinical trials of PIs enrolling HIV-infected adult patients (amprenavir and fosamprenavir [APV], atazanavir [ATV], darunavir [DRV], indinavir [IDV], lopinavir [LPV], nelfinavir [NFV], ritonavir [RTV], saquinavir [SQV], tipranavir [TPV]) were selected for evaluation. Papers reporting duplicate patients were excluded. Studies cited in drug labels and medical reviews on the US FDA Approved Drug Products list, for which no publication were available, were retained and information collected from the same source (http://www.fda.gov/oashi/aids/virals.html).
A search was conducted using PubMed. The medical subject headings were developed in collaboration with an experienced medical librarian. Keywords anywhere in the text for PubMed were: ‘[generic drug name] and clinical trial’ in the full paper.
Clinical trials (ongoing and closed) performed on the single drug were searched also on http://www.clinicaltrials.gov. On each retrieved article a hand-research of references was performed.
From each study, the following information was extracted on a standardized form: molecule being investigated, number of study patients, age (median or mean), gender and ethnicity, country/ies where it was conducted, blindness, naïve or experienced patients enrolled, phase and number of participating centres, year of study data publication. The following categories were identified for ethnicity: Caucasian, African/African-Americans, Hispanic, other (including original category of ‘other’ and ‘Asian’), not reported (calculated by subtracting all other categories from the total number of subjects enrolled). If only proportions were reported, data were converted to actual numbers by calculation and rounded to the nearest integer.
Pearson's chi-squared test was used for trend over time (calendar year of publication) was used to assess changes over time in proportion of women and of non-Caucasians included in trials. Spearman correlation coefficient was used to evaluate correlation between proportion of females and proportion of non-Caucasians. Wilcoxon rank-sum test (Mann-Whitney) was used to compare the proportion of females and of different ethnicity according to blindness of the study, being naïve at enrolment and the participation in the study of patients from at least one developing country.
Results
Forty-nine clinical trials were included and data relative to a total of 10,224 patients were analysed (Table 1). Clinical trials were conducted in centres in North America (n = 39), Central-South America (n = 22), Europe (n = 22), Africa (n = 8), Asia (n = 5) and Australia (n = 10) (Table 2). Most trials (n = 37) were conducted in more than one continent.
Clinical trials per molecule (n = 49)

Countries involved in 49 registrative trials of protease inhibitors

Overall mean age was 39.6 years (calculated on the 27 studies reporting mean age). Overall, 19.4% of included patients were women (calculated on the 45 studies reporting gender distribution); median proportion of women was 16.3% (range 0 in a NFV trial to 41.2% in an ATV trial). Pooling for each drug, median proportion of women ranged from 8.1% – in RTV trials to 35.9% in ATV trials.
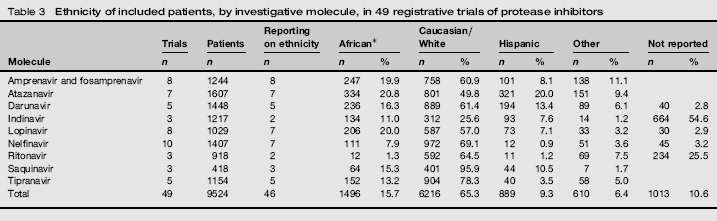
Of the 49 reports, 46 (93.9%) reported data on ethnicity, but in six studies ethnicities other than Caucasian were not specified. Overall, the number of study subjects for whom ethnicity was not reported was 1013 (9.9%). The most represented ethnic group was Caucasian, including 6216 (60.8%) subjects. Africans comprised 1496 (14.6%) and Hispanics 889 (8.7%) of subjects. In the group ‘other’ were gathered 610 (6.0%) subjects. Breakdown per molecule is reported in Table 3.
Ethnicity of included patients, by investigative molecule, in 49 registrative trials of protease inhibitors
A test for trend over time (1996-2009) shows a significant increase in proportion of women included (P = 0.012), and a decrease of proportion of Caucasians patients included, reaching borderline significance (P = 0.061) (Figure 1). Trends for individual ethnicities were not significant.
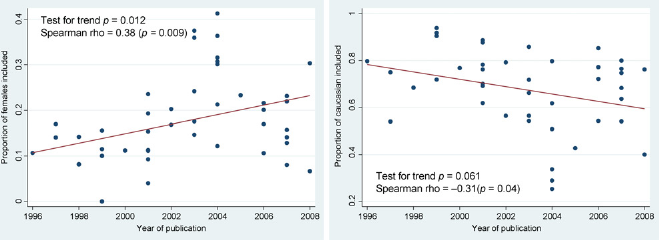
Proportion of females and of Caucasians included in 49 registrative clinical trials of protease inhibitors, over time (years of publication 1996-2008)
Interestingly, an inverse correlation was observed between the proportion of Caucasians and that of women enrolled in each study (r = -0.65, P < 0.0001) (Figure 2). Moreover, the median proportion of women in studies including at least one developing country was higher than in studies conducted only in developed countries (21.4% versus 12.7%, P = 0.018), as well as the median proportion of patients classified as ‘other than Caucasian’ (37.4% versus 23.6%, P = 0.016).
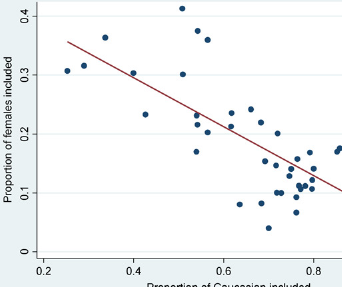
Correlation between proportion of females and of Caucasians included in 49 registrative clinical trials of protease inhibitors
With regard to study design, women were less likely to be included in double-blind studies (11.2% versus 17%, P = 0.03), while no difference in this regard was observed for ethnicity. The proportion of female patients enrolled in trials for treatment-naive compared with that for experienced patients was borderline significance (25.8% versus 15.4%, P = 0.042).
Discussion
Rates of enrolment of women and minorities (other than Caucasian ethnicity) in the registrative clinical trials for PIs, the cornerstone treatment drugs for HIV infection, show a positive trend since 1996, mirroring the fact that the number of people of ethnic groups accessing antiretroviral therapy (ART) is globally growing.8,9 In absolute numbers, though, patients belonging to minorities recruited remain low, compared with that of Caucasians, although the majority of people living with HIV belongs to other-than-Caucasian ethnic groups; the same can be said for recruitment of women compared to that of men.
It had already been demonstrated in the past that participation in research trials for HIV-infected patients was influenced by gender, race or ethnic group, 5 in particular non-Hispanic whites were over-represented.
Even in affluent countries, what was initially a disease of men who have sex with men (MSM) is now a disease predominantly affecting minorities and women. 10 Given the relatively small representation of other-than-Caucasian ethnic groups, registrative studies might lack the power to detect differences in efficacy and tolerability of antiretroviral regimens between ethnic groups. It has been recommended that clinical trials represent the diversity of the populations to which study results will be applied, in terms of race, gender and other factors, not only for ethical reasons (reducing health disparities among population groups) but also because these elements can influence disease course, treatment response, toxicity and health behaviour. 1 For these reasons, an FDA suggestion since 2001, is that women and minorities are adequately represented in registrative trials.1-4 One motive that might account for under representation of other-than-Caucasian groups is that few registrative clinical trials are conducted in Asia, Africa and South America, owing to a number of issues, such as lack of laboratory facilities, lack of dedicated staff and absence of ethics committees.11-13 This negative attitude might be aggravated by the fact that participation in clinical trials in developing countries often represents the only way to gain access to health care.14-16
The enrolment issue of African-Americans and Hispanics in clinical trials in the USA has been an important topic in public health discussions. Minorities may be reluctant to be involved in clinical research for reasons of mistrust and prejudice against the medical profession and, possibly, for limited access to care (absence of health insurance).17-20 It is interesting that despite low participation of minorities in phase III clinical trials, a higher than expected participation of minorities as healthy volunteers in phase I studies has been observed. A crucial difference exists between these types of research, as participation in phase I studies is remunerated, while in phase III is voluntary. 21
The problem of low recruitment of minorities in clinical trials might aggravated by the fact that the scaling up of treatment 22 has not been matched by a proportional development in pharmacovigilance practice in low- and middle-income countries. 8 The current knowledge of the side-effects and adverse events of ART is based on data collected primarily in high-income countries from populations whose demographics, genetic background, nutritional status and co-morbidity may vary substantially from those of the populations in low- and middle-income countries. Of the 80,000 reports of adverse reactions to antiretroviral medicines included in the WHO global Individual Case Safety Reports (ICSR) database at the WHO Collaborating Centre for International Drug Monitoring Programme in Uppsala, Sweden, only 6000 came from low- and middle-income countries, substantially compromising the identification and optimal management of drug adverse events. 23
These issues are not of secondary relevance as drug toxicity can severely affect people's health and safety and undermine their adherence to ART, not only increasing morbidity and mortality but also leading to the emergence of secondary drug resistance.
Data about efavirenz (EFV) are indicative, among persons of African descent, there are apparent differences in genetic polymorphisms in the cytochrome P450 system that may account for prolonged metabolic clearance of efavirenz (EFV) and increased central nervous system effects. 24 Thai patients, on the contrary, in a study evaluating tenofovir/emtricitabine (TDF/FTC) plus EFV had lower rate of EFV-related neuropsychiatric disturbances than those reported in developed countries, while renal toxicity due to TDF was higher than in the published literature. 25
As reported also by others, 26 a low proportion of women enrolled in registrative trials was observed in the present analysis (19.2%); although it is interesting that a higher percentage of women was enrolled in multicentre trials conducted in at least one developing than in those conducted only in developing country. Women account for half of all people living with HIV worldwide, and nearly 60% of HIV infections in sub-Saharan Africa, 9 and it is therefore noteworthy that women be adequately represented in clinical trials, particularly in those regions where they account for the majority of patients.
In the past, women have often been excluded from clinical trials for several reasons, such as the belief that data from men were cleaner because of the lack of interference from oestrus or menstrual cycles or the fear of inducing fetal deformities in pregnant subjects. 18 The importance of recruitment of women in clinical trials has been recently emphasized by the pharmaceutical industry; in fact the GRACE study, a phase 3b study, evaluated specifically the efficacy and safety of DRV in women. 27 The results of this study evidenced a difference in adverse event rates between men and women, showing a lower virological response rate in women. It has been suggested that the susceptibility to adverse events may differ between women and men based on differences in weight and pharmacokinetics.
Other complications of treatment itself were attributed to differences relative to gender and/or race. Among women, for example, there have been reports of increased frequency of rash with nevirapine or lactic acidosis with combined use of didanosine and stavudine in pregnancy. 28 More recently, lipodystrophy syndrome was correlated to ethnicity, in particular African women seem to be more at risk to develop central lipohypertrophy than White Caucasian men. 29 A recent study demonstrated significant racial/ethnic- and gender-related differences for specific types of grade 4 adverse events due to highly active ART but not for overall adverse events rates, all-cause mortality rates or rates of toxicity-related discontinuation of therapy. 30 From an efficacy point of view, HIV subtypes in the developing world (mainly subtype C) are different from those circulating in the developed world (mainly subtype B); the latter are used for the development of antiretroviral drugs. 31 Therefore, despite the fact that observational studies conducted in Europe32,33 have demonstrated that non-B subtypes show an excellent response to first-line ART, further studies should be performed to corroborate these initial observations.
In summary, despite a positive trend was observed relative to enrolment of minorities (women and other than Caucasian) in registrative trials of PIs since 1996, the challenge for the future will be to assure an increase access to clinical trial of new antiretroviral drug for minorities in order to ensure better safety and efficacy data collection and analysis.