
Abstract
A 21-year-old man presented to genitourinary (GU) medicine physicians with (initially) painful penile and scrotal swelling. A diagnosis of anogenital granulomatosis was confirmed on histological analysis of penile skin. Enquiring about systemic symptoms resulted in the additional diagnosis of gastrointestinal Crohn's disease. The patient is now receiving immunosuppressive therapy to treat both conditions.
Introduction
anogenital granulomatosis (AGG) is an uncommon but important condition to consider in the differential diagnoses of genital swelling. AGG may occur in isolation or, as in our patient, in association with systemic conditions, e.g. Crohn's disease. Early diagnosis, prompt initiation of treatment and referral to the relevant specialties are crucial as established genital lymphoedema is irreversible and sexually and socially debilitating.
History
A 21-year-old Caucasian heterosexual man attended a genitourinary (GU) medicine clinic with a six-week history of painful penile erythema and swelling, which subsequently became painless. He denied any urethral discharge, dysuria, testicular pain or rectal symptoms. He had one female partner for the past two years and there was no history of anal penetration.
Two years prior to developing genital swelling he was diagnosed with orofacial granulomatosis, confirmed on mucosal biopsy; symptoms had settled spontaneously. The patient also gave a recent history of intermittent lower abdominal pains. Examination revealed significant erythema and swelling of the penis and scrotal skin consistent with lymphoedema (Figure 1). It was impossible to retract the foreskin.

Penile and scrotal erythema and lymphoedema
Perianal inflammation, Assuring and skin tags were noted. No ulceration or inguinal lymphadenopathy were detected and there was no oedema elsewhere.
Investigations
A sexually transmitted infection screen, including rectal chlamydia, was negative and an abdominal-pelvic ultrasound scan was normal. The patient was referred to the lymphoedema clinic. Penile and scrotal skin biopsies revealed the presence of a non-caseating granulomatous inflammatory infiltrate (Figure 2) confirming the diagnosis of AGG. Sarcoidosis was excluded by clinical examination, normal chest radiograph and blood tests.
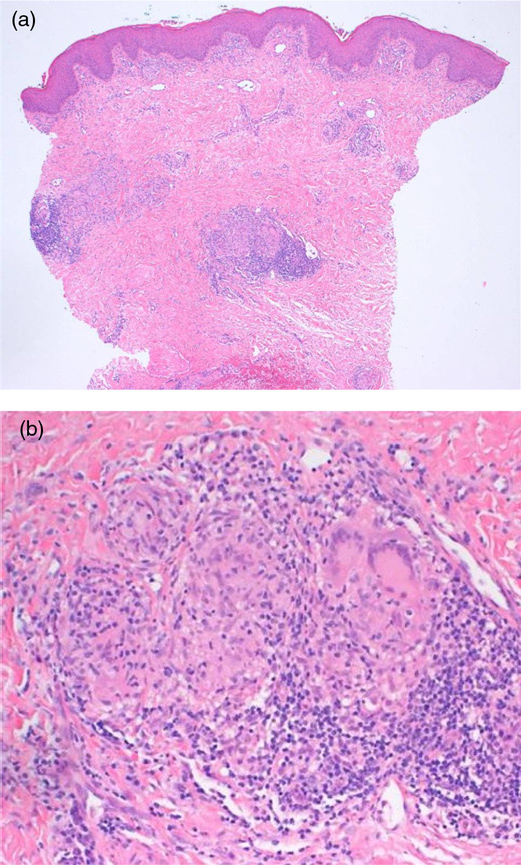
Low power view (a): normal epidermis, mild superficial perivascular chronic inflammatory infiltrate of the dermis and dense deep perivascular infiltrates forming non-caseating granulomas. Negative Ziehl-Neelson and diastase periodiacid Schiff stains. High power view (b): histiocytes, multinucleate giant cells, lymphocytes and plasma cells confirming the diagnosis of anogenital granulomatosis
Given the history of intermittent abdominal pain the patient was referred for a gastroenterology opinion and colonoscopy. Biopsies of the terminal ileum revealed changes consistent with Crohn's disease.
Treatment
The patient was unresponsive to prolonged courses of antibiotics, including co-trimoxazole 960 mg twice-daily for 12 weeks. The gastroenterologist commenced high-dose oral prednisolone (40 mg/day) and lymphoedema therapists provided supportive compression garments. Within two months the patient noted a marked reduction in penile and scrotal swelling and erythema, but with some residual swelling of the foreskin. Unfortunately he suffered recurrent penile swelling on tapering prednisolone. Subsequently azathioprine and infliximab were unsuccessful as steroid-sparing agents and he recently commenced mycophenolate mofetil. The patient has been referred to the urologist for circumcision to improve micturition and sexual function.
Discussion
Genital lymphoedema may occur as a result of infectious or non-infectious diseases that cause impaired lymphatic drainage at the level of the inguinal or pelvic lymph nodes. Infective causes are rare in Europe but include filariasis, tuberculosis, lymphogranuloma venereum, Kaposi's sarcoma, syphilis and recurrent genital cellulitis. Non-infective causes of genital lymphoedema include genital neoplasia (including tumour relapse), cancer treatment (extensive genital surgery, lymphadenectomy, radiotherapy) or inflammatory disorders (AGG, hidradenitis suppurativa). 1
AGG is a rare chronic inflammatory disorder of unknown aetiology. The term was proposed by van de Scheur et al. 2 in 2003 to encompass previously recognized entities including posthitis granulomatosa and ano-perineitis granulomatosa. A diagnosis of AGG should precipitate investigation to exclude the presence of an associated systemic disorder, e.g. Crohn's disease, or very rarely sarcoidosis. In the majority of patients, however, AGG will be an isolated diagnosis. Van de Scheur's 2 review of AGG suggested that underlying Crohn's disease was only present in one-third of patients with AGG.
AGG presents with penile, scrotal, vulval or ano-perineal swelling with or without erythema. Histological examination of affected skin reveals non-caseating giant cell granulomas. 2 It has been proposed that in AGG chronic inflammation leads to lymphoedema of the affected area due to intra-lymphatic occlusion by the granulomata. 3 These are indistinguishable from those seen in sarcoidosis and gastrointestinal Crohn's disease, making histological differentiation between AGG and extra-intestinal Crohn's disease difficult. However, patients with Crohn's disease rarely develop cutaneous ‘metastatic Crohn's’ lesions, and they tend to be granulomatous nodules or ulcerations occurring on a background of longstanding gastrointestinal disease.4,5 orofacial granulomatosis appears to be the equivalent disease of AGG affecting the mouth.
Management of AGG is based on anecdotal reports. Antibiotics, oral steroids and systemic immunosuppressants such as azathioprine, mesalazine and anti-tumour necrosis factor agents have been used with variable success.2,6
Established lymphoedema is psychosexually debilitating and often irreversible, responding poorly to both traditional lymphoedema treatments (manual lymphatic drainage and compression) and immunosuppressive therapy. Surgical management is considered for patients with severe disease where conservative measures have failed.1,7 Our clinical experience of over 20 patients with AGG has highlighted the importance of prompt diagnosis and management to minimize complications.