
Abstract
Objectives
National Health Service (NHS) foundation trusts have been created to decentralize the management of NHS provider organizations through the substitution of central government control with local accountability to citizens and employed staff. Our aim was to explore the roles adopted by elected and appointed governors of a first wave NHS foundation trust and the extent to which governors shared power with trust directors and influenced the management of the trust.
Methods
A one-year case study of a single NHS foundation trust (Homerton Hospital in East London) was conducted. Data were collected using face-to-face interviews with a sample of governors and directors, as well as through non-participant observation of public and private meetings of governors and documentary analysis.
Results
Governors and directors found the new role of foundation trust governor ambiguous and difficult to define. This lack of clarity impeded the development of the new governance function. Governors perceived that they had made little impact on the decisions of the Trust during the year of study. However, evidence was found of an increased involvement of governors and the public in the activities of the Trust.
Conclusions
Government plans to decentralize accountability of public hospitals to local communities appear problematic, at least in the short term. Unless the effectiveness of the new local governance arrangements is addressed, an accountability ‘gap’ may emerge as prior mechanisms for public accountability to the centre are dismantled. In these circumstances, decentralization may lead in practice to a loss of public accountability.
Introduction
Foundation trusts have been created in the English National Health Service (NHS) as part of a policy to decentralize the management of publicly owned health care provider organizations. 1 This is consistent with an international trend towards the separation of government from the delivery of public services (‘new public management’). 2
Foundation trusts are intended to replace state ownership of hospitals with ‘social ownership’ where citizens and staff can enjoy membership rights and a formal role in the governance of the organization.3,4 This paper reports on an evaluation of the early implementation of these new governance structures at one London hospital (Homerton Hospital) and considers whether or not the objective of greater public and staff involvement in decision-making has been achieved.
Why and how to involve the public?
The desire for public involvement in health services is a formal policy goal for many health systems. 5 This goal stems from two beliefs: that public involvement will lead to health services that better reflect the needs of patients; and that public involvement in a publicly funded health system is an inherent democratic right of the citizen and a means of ensuring the accountability of public agents. 6
The Council of Europe has recommended that citizen participation should apply to all aspects of the health care system, including priority setting and decision-making at national, regional and local levels. 7 This includes participation in decision-making within health care providers. However, while this guidance sets out the scope of involvement, it says little about the desirable intensity of that involvement (i.e. the extent to which it results in the redistribution of power from decision-makers to citizens or patients). Intensity of involvement has been conceptualized as a scale or ladder with the degree of power sharing by citizens rising with each step.8,9
Charles and DeMaio 10 have developed an analytical framework that brings together the different domains of decision-making and the extent of citizen involvement. Three domains of decision-making are identified: ‘macro’ (policy decisions at national, state or provincial level); ‘service’ (resource allocation decisions about what services are delivered, where, how and by whom) and ‘treatment’ (decisions about care to be given to individual patients). The extent of citizen involvement is defined as: ‘consultation’ (an opportunity to express views with no guarantee that they will be taken into account); ‘partnership’ (a redistribution of power through shared decision-making and planning); and ‘dominant’ (citizens in full charge of decision-making). For the purposes of this paper, we shall use ‘involvement’ as a generic term that encompasses a range of concepts such as consultation and participation. 5
What are foundation trusts?
Foundation trusts are public hospitals (and latterly mental health service providers) that have been freed from the direct control of central government and are instead authorized and regulated by an independent regulator (known as Monitor). They enjoy a number of freedoms compared with other NHS hospitals, including the ability to borrow money for investment.
Foundation trusts have been established as ‘public benefit organizations’ with ‘members’ drawn from among patients, staff and the wider public. Members’ interests are represented formally within the governance structure by elected ‘governors’ who form a Board of Governors, the majority of the members of which must represent public members. This Board of Governors is formally recognized within the constitution of the Trust and has a number of important statutory powers including the appointment and removal of the Chair and the non-executive directors of the hospital's management board and the right to be consulted on the Trust's future plans.
The government's aim for foundation trusts is that they increase local accountability of decision-making with respect to the provision of health services. Foundation trusts are described as ‘democratic’ by the government and they expect that, through the actions of governors, ‘major decisions [will be] informed by active participation from members based in local communities’.1(p. 7)
If the government's aims are realized, greater public accountability will result across a number of different dimensions of accountability identified by Ashworth and Skelcher: 11 the views of members and citizens will be ‘taken into account’ through the work of governors; the foundation trust will be obliged to ‘give an account’ in the shape of reports to members and governors and trust management will be ‘held to account’ in that they may be dismissed by governors. Foundation trusts’ governance arrangements are an example of citizen involvement consistent with the recommendations of the Council of Europe and fit Charles and De Maio's second domain of decision-making (‘service’).
Methods
Two earlier studies have examined the governance arrangements of the initial tranche of 20 foundation trusts in broad terms.12,13 They both suggested that the role of foundation trust governors was variable and ambiguous. This study explores the role of governors in-depth and over time through a case study of a single hospital during its first year of operation as a foundation trust (April 2004 to March 2005). The aims of the research were to identify:
the role(s) adopted by Homerton Hospital's governors;
the extent to which governors shared power within the decision-making structures of the hospital;
the impact, if any, governors had on the management of Homerton Hospital.
A case study method was selected as the objective was to study a contemporary event (the introduction of new governance structures) in a real life context, where the context was not clearly distinguishable from the phenomenon under investigation. 14 The research was conducted through face-to-face, in-depth interviews with a broad range of stakeholders involved in the governance of Homerton Hospital. In addition, one researcher (RL) attended five public and private meetings of the governors and the Annual Members’ Meeting as a non-participant observer. In addition, descriptive data (such as the managerial groups that governors belonged to) were collected to illustrate the way in which the new governance arrangements were implemented.
The Council of Governors (the name given to the Board of Governors at Homerton Hospital) had 25 members at the time the fieldwork commenced in June 2004 (this later rose to 27 members) and a random sample was enrolled into the study ensuring each constituency was represented in the same proportion as on the Council of Governors (Table 1). In addition, four trust executive and non-executive directors most involved with the establishment of the trust (including the Chair and Chief Executive) were selected to be part of the study.
Study sample
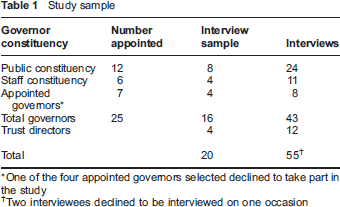
One of the four appointed governors selected declined to take part in the study
Two interviewees declined to be interviewed on one occasion
Interviews were held on three different occasions to allow respondents to reflect on changes over time. Interviews were semi-structured and schedules were developed for each category of interviewee. The sequential rounds of interviewing allowed the themes that emerged to be developed during later interviews and interview schedules were amended accordingly.
Interviews were tape recorded (although there were technical difficulties with a number of interviews) and detailed contemporaneous notes were made at each interview and at the meetings of governors attended. Direct quotes contained in this paper have been verified using tape recordings of interviews.
The researchers adopted an analytical approach based on modified grounded theory. 15 Initial themes were identified from theory, in this case theories of public accountability together with the government's espoused aims for foundation trust governance, and used to guide the semi-structured interviews. Data collected in each round of interviews (and through observation) were analysed by the researchers who identified further themes independently and then met to discuss and validate these themes jointly. This form of progressive analysis allowed data collection to be informed by the hypotheses as they were evolving.
The analysis and resulting findings were validated through the triangulation of interview data with data collected through observation (i.e. views espoused during interview were considered in the context of actions and opinions expressed during private and public meetings). Observational data were also used to identify implicit governor roles that had not been explicitly raised during interview. Any bias among the researchers was challenged through the process of independent then joint data analysis.
Results
This section reports on the results of the study and considers them in the context of the government's espoused aims for the new governance arrangements for foundation trusts.
Representing and involving the local community
The aim that foundation trusts should involve citizens and staff in decision-making is dependent, in part at least, on the extent to which foundation trusts are able to attract members from within the local community, the extent to which those members are active, and the extent to which governors can accurately reflect the interests of the local community.
When Homerton Hospital was legally established as a foundation trust in April 2004, it had attracted 2916 members. This figure rose to 3660 by August 2004, but remained a very small proportion of the approximately 250,000 residents eligible for membership. This suggests that the Trust had not engaged with a broad sweep of its local community. However, the membership when analysed in 2006–07 was broadly in line with the socioeconomic make-up of the local community 16 suggesting that, in this regard at least, it was ‘representative’ as desired by the government. Moreover, this small membership proved relatively active. In the elections of 20 staff and public governors, a turnout of 42% of members was recorded. 17 This compares favourably with local elections where turnout averages around one-third of eligible voters. 18
It was notable that a number of governors were ambivalent about the merits of the foundation trust policy on joining the Council of Governors (Box 1). They were not convinced that foundation trusts would prove an effective vehicle for public involvement.
Governors’ views on foundation trust policy
‘I was sceptical… Would it be lip service or empower people to make decisions?’
(Public governor 1 – Interview round 1)
’I opposed foundation status because I felt that the elements of democratic accountability that were being brought in were woefully inadequate.
(Public governor 2 – Interview round 1)
’One of the reasons that motivated me to get involved was the very fact that I am an apolitical animal, I have no political affiliations and I was afraid that it appears to be such a hot potato… that [the foundation trust] would be dominated by the political actors with their own agendas.
(Public governor 3 – Interview round 1)
Public governors were also unclear about how best to represent the very diverse communities of the inner London population served by the hospital. How to provide an adequate channel of communication with members (and with the wider public, the vast majority of whom had not sought membership) presented an ongoing problem. By the end of the first year, several governors were frustrated that they had not yet, in their view, established an effective way of understanding members’ views and feeding these into the decision-making of the hospital.
This finding was mirrored by staff governors who also struggled to engage with the members they represented, notwithstanding the fact that they had a largely captive audience. Staff governors made themselves available to staff members at designated times but these opportunities were generally not made use of by staff.
However, some opportunities to involve members of the public were developed with success. A public meeting in September 2004 attracted approximately 300 people (compared with fewer than 20 people who attended the annual hospital meeting the year before). In addition, 150 members responded to a questionnaire saying that they were keen to get more involved in the running of the hospital.
In addition, governors were involved in the management of the Trust in numerous ways (Box 2), although, as discussed below, this did not lead to a well-developed sense of empowerment.
Examples of the involvement of governors in the management of Homerton Hospital (2004–05)
Mandatory subcommittees of the Council of Governors
Nominations Committee (appointed one hospital non-executive director during 2004)
Remuneration Committee
Membership Development Committee
Subcommittees of the Board of Directors with governor representation
Clinical Governance and Modernisation Committee
Research and Development Committee
Clinical Practice Ethics Forum
Patient and Public Involvement Committee
Other areas of governor involvement in hospital management
Appointment of Trust external auditors
Membership of Clinical Practices Ethics Forum
Participation in Patient and Public Involvement Forum hospital inspections and subsequent drawing up of recommendations
Participation in training of health care assistants
Participation in open days and ‘awareness days’
Participation in topic-specific Members’ Forums
Holding open access ‘surgeries’ for members
Public accountability and the role of governors
The debate about how best to engage with members was linked to a more fundamental issue, how the new form of strengthened public accountability would be delivered in practice. As described above, governors are central to this. The Department of Health envisaged three types of role for governors: advisory (providing a steer as to how the Trust should carry out its business); guardianship (ensuring the Trust acts in a way that is consistent with its statement of purpose); and strategic (advising the board of directors on the longer term direction of the Trust).3,4
However, the governors and directors at Homerton Hospital found these roles ambiguous and open to multiple interpretations. From interviews and observational data from early meetings of the Council of Governors, a larger number of potential governor roles emerged that governors, albeit to varying degrees, considered legitimate. These were developed by the researchers into a typology that was used as a framework within which to explore the beliefs of directors and governors as to how the Council of Governors might operate within the Trust (Table 2).
Typology of potential roles of a foundation trust governor
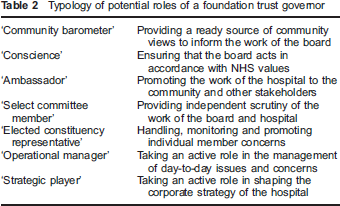
When tested with interviewees, all roles enjoyed some support among governors and most among directors. The role of ‘operational manager’ was least supported by governors and not at all by directors. This is consistent with Department of Health guidance that the day-to-day management of the Trust should remain the responsibility of the Board of Directors.
There was little agreement, however, over the appropriate balance between these roles or the practicality of governors discharging them. The question of whether or not governors should act as ‘elected constituency representatives’, in particular, excited considerable debate and disagreement. Some governors felt that by offering to take up individual members’ concerns governors would offer some tangible value. This role was closest to that of the elected local authority member (a role that a number of governors also undertook). Others believed that this role would inappropriately interfere with routine managerial processes within the Trust and also risk governors not developing a more strategic role.
By April 2005, the governors had resolved this tension by agreeing to hold monthly drop-in ‘surgeries’ at which a number of governors would be available to hear members’ views and comments. However, these surgeries would not link members with any particular governor and any sense of ‘representative government’ was deliberately played down.
Impact of governors on the decision-making within the trust
Both governors and directors were relatively modest in their aims for the first year, citing greater clarity over the role and a sound partnership with the board as reasonable and achievable outcomes. However, when interviewed in the early months of the foundation trust, many governors harboured significant doubts as to the likely efficacy and power of the council of governors (Box 3).
Views of governors on their decision-making power
‘All indications are that we are the toothless tigers… and talking puppets.’
(Public governor 4 – Interview round 1)
‘I'm very much in the dark about [the influence of governors] because my understanding from the meetings we have had so far is that the governing body has very little power.’
(Public governor 5 – Interview round 1)
‘… I am keen on empowering people, enabling patients to express themselves. From what I have seen [foundation trust status] is not going to lead to one iota of improvement in patient care.’
(Appointed governor 1 – Interview round 1)
The issue of where the appropriate limits to the power of the Council of Governors lay proved difficult to resolve and a number of different views emerged. For their part, the Trust directors were unanimous that, ultimately, the Board was responsible for making decisions. However, they were equally clear that they had a duty to listen to the Council of Governors and to take their views into account in reaching their decision.
Governors’ views were more varied and two contrasting models of appropriate governance emerged. One view suggested that, legitimized by its election by members, the Council of Governors should take an equal role in setting strategy alongside the Board of Directors, or even that it should lead strategic decision-making. This chimes with the notion advanced in official guidance that foundation trusts should be ‘democratic’ organizations, although it goes further than the advisory role set out by the Department of Health. 4 This view was challenged by other governors who believed that the complexity of trust management made it simply impractical to dictate terms to the Board of Directors, whether or not this was in fact desirable (Box 4).
The role of the Council of Governors
‘We are representative of the people… the strategic direction of this hospital is down to us with the senior management to decide.’
(Public governor 1 – Interview round 1)
‘At the moment we are very much led by directors… In five years’ time… the major strategic decisions [should be] made basically by governors with directors and professionals as their advisers.’
(Public governor 1 – Interview round 3)
‘If this hospital is going to succeed as a foundation trust it cannot simply be seen to be getting the governors to rubber stamp stuff. .. because the whole thing would just fade away, nobody would want to play the game at all, it becomes a joke.’
(Public governor 7 – Interview round 1)
‘Personally I would like to see the governors’ board deciding on major issues.’
(Public governor 6 – Interview round 2)
‘I'm not convinced that the executive necessarily needs a bunch of non-professionals telling them how to do their jobs.’
(Public governor 3 – Interview round 1)
‘I can't see how a bunch of relatively ill-informed people can second guess the board in terms of policy-making. They are already doing an excellent job and should be supported.’
(Appointed governor 1 – Interview round 1)
‘I think strategy requires a level of knowledge that we can't assume to be held [among governors].’
(Director 1 – Interview round 3)
This latter view was shared by directors who saw more potential value from governors focusing on improving what was termed ‘the patient experience’ rather than hospital strategy (for example, by developing and improving information presented to patients on admission to the hospital or ensuring that hospital services reflected different cultural needs).
By the end of the first year, most governors felt that they had exerted little or no influence over the Board of Directors (Box 5). In many cases, governors expressed disappointment over this lack of power, although there was also a belief that the new system of governance was now bedding in with governors expecting to exert greater influence in the future.
Governors’ views of their powers
‘I regret to say that I wouldn't be able to pinpoint a particular point or issue that I have been able to achieve by my being a governor.’
(Public governor 6 – Interview round 3)
‘There have been times when I thought we're have achieved nothing at all, absolutely nothing – the whole thing is a misconception and we're just making work for ourselves… But I don't always think like that... from the governors point of view I think it's been quite hard and quite frustrating.’
(Public governor 5 – Interview round 3)
‘I'm not aware of any decision that we've influenced… I don't know whether we are just kind of going through the process because it's now in the constitution [that] you've got to ask us.’
(Staff governor 1 – Interview round 3)
In contrast, Trust directors expressed positive opinions about the experience of the first year, perhaps reflecting their lower expectations of the governors’ impact. Nevertheless, directors found the precise benefits of the new governance arrangements difficult to describe in detail. However, they did identify a greater sense of scrutiny of the decisions of the Board of Directors.
Discussion
In its first year of operation, the Council of Governors made little tangible impact on the running of Homerton Hospital. In this regard, the new governance arrangements have so far failed to deliver the government's objectives of ‘social ownership’ where members influence the management of the Trust.
Yet, to expect that decision-making would be transformed within one year is perhaps to expect too much. There were indications that the local community had increased the scope and depth of its involvement in the hospital in a number of ways, both directly and indirectly through governors. In addition, the membership, while small, did at least broadly represent the socioeconomic diversity of the communities served by the Trust. Moreover, the Trust's directors at least felt themselves to be more locally accountable.
However, these new governance arrangements were established without a clear or shared sense of the new role of governors and members. National guidance was insufficient in this regard and Homerton Hospital was left to breathe life into the government's framework for itself. The result was that governors developed their own sense of what the role of a governor should be – sometimes going beyond that envisaged in government guidance. This lack of role clarity appears to have been present in a number of early foundation trusts. 13
Using Charles and De Maio's framework, citizen and staff involvement in the management of Homerton Hospital falls clearly into the category of ‘consultation’. The directors felt that they had a duty to listen to governors but no more (‘taking into account’ their views according to Ashworth and Skelcher's typology of accountability). Some governors felt this was appropriate and doubted their ability to take more power due to their limitations of time and expertise. Other governors had ambitions to extend their decision-making power and to institute a ‘partnership’ model, signalling that further debate within the Trust will be necessary.
The notion, promulgated in national guidance, that the foundation trust should be ‘democratic’, has led to some confusion during implementation. Public governors, like local councillors, are subject to direct elections by local people. However, once elected, governors’ powers are much more circumscribed than those of councillors. Whereas councillors set overall policy and hold officers directly to account for discharging this policy, the intended relationship between governors and the Board of Directors is subject to a more subtle balance of power – governors must be listened to, but cannot dictate policy; the Board is empowered to run the hospital but the Chair and non-executive directors can be dismissed by the governors. However, the sacking of non-executives is a major weapon and one that our study suggests would be used only in the most exceptional circumstances.
Governors exhibited little if any influence over strategic decision-making within the Trust and therefore fell short of the expectations of the government when it set out its policy. Ultimately, what is meant by the government's proposition that, through foundation trust membership, ‘local people get involved in the running of their local services’ is difficult to pin down in practice.
As with all case studies, there may be doubts about the generalizability of the findings. However, Homerton Hospital existed within the same overall policy framework and was subject to the same guidance as all foundation trusts, suggesting that, insofar as this context was important in shaping the governance (as we believe it was), this was common to all. Further, the classification of potential governor roles that we developed was discussed at a seminar with governors representing a large number of foundation trusts and found to resonate with them.
It seems unlikely therefore that these findings are unique to Homerton Hospital and consequently may have implications for wider public policy. The development of ‘social ownership’ and accountability to local communities are essential components of the policy to decentralize the management of health care provision in England, while retaining a sense of public involvement and scrutiny. As national government retreats from the provision of care, greater local accountability is intended to replace accountability to the centre and therefore prevent the opening of an ‘accountability gap’. However, if these new governance arrangements for foundation trusts are not further developed, with clearer roles for members and their representatives leading to more impact on the actions of the board, they are unlikely to deliver on this expectation. In these circumstances, decentralization may in practice lead to a loss of public accountability.
Footnotes
Acknowledgements
This research did not receive formal research ethics approval as the Chair of the Research Ethics Committee confirmed in writing that, having reviewed the research protocol, his committee did not need to consider it formally. The project was subject to Homerton Hospital's research governance arrangements and the hospital has confirmed that it is happy to be named in the article.