
Abstract
Objective:
To assess the impacts of different forms of case management for people aged over 65 years at risk of unplanned hospital admission, in particular the impacts upon patients, carers and health service organization in English primary care; and, in these respects, compare the Evercare model with alternatives.
Methods:
Multiple qualitative case studies comparing case management in nine English Primary Care Trusts which piloted the Evercare model of case management and four sites which implemented alternative forms of case management between 2003 and 2005. Data were obtained from 231 interviews with patients, carers and other key informants, and from content analysis of documents and observation of meetings.
Results:
All the projects established functioning case management services, but none led to major service reorganization or savings elsewhere in the health care system. Many informants reported examples of admissions which case management had prevented, but overall hospital admissions did not significantly change, possibly due to increased case-finding. Patients and carers valued case management for improving access to health care, increasing psychosocial support and improving communication with health professionals.
Conclusion:
Case management was highly valued by patients and their carers, but there were few major differences in outcomes between Evercare and other models.
Introduction
The Evercare pilot projects run by UnitedHealth Europe (UHE) 1 and subsequently the Community Matron programme2,3 reintroduced case management for frail elderly people to the English NHS. Case management has been defined as the assessment, coordination, monitoring and delivery of services to meet patients’ needs, 4 in the present case preventive and responsive care for patients aged over 65 years at high risk of emergency hospital admission. Reducing the rate and duration of unplanned emergency hospital admissions for these patients was Evercare's best-known, but not sole, objective.
While some studies report beneficial outcomes from case management, its impact is unpredictable and may depend heavily on the context in which it is introduced; 5 – 8 i.e. the organizational structures of the programmes, the financial and regulatory framework, the physical and human resources available, and the knowledge and motivation of health and social care staff. We carried out a combined quantitative and qualitative evaluation of the Evercare pilots. The quantitative component, reported elsewhere, 9 analysed the effect of Evercare on hospital admissions, bed days, and mortality. This paper describes the qualitative part of the evaluation. Policy-makers expressly assumed that the Evercare model would be effective in:
stimulating a wider re-engineering of primary care for older people, in the sense of service redesign beyond the introduction of case management itself;
reducing unplanned hospital admissions by substituting case management in primary care;
being acceptable to stakeholders, especially patients and carers.
This paper provides qualitative evidence which tests these hypotheses, thereby allowing more detailed interpretation to be made of existing quantitative studies. In doing so it compares several models of case management with each other rather than compare one case management model with a control of no case management.
Methods
We used an explanatory multiple case study design 10 to test the above policy assumptions (hypotheses). Taking the local case management project as the unit of analysis (‘case’), data were collected predominantly through key informant interviews, supplemented with content analyses of documents collected from official websites and which fieldwork informants had indicated were seminal, and with field-notes made in ‘observer-as-participant’ role 11 at national level meetings and training sessions. The cleaned field notes, content analyses and interview schedules were all structured using the common set of categories described below.
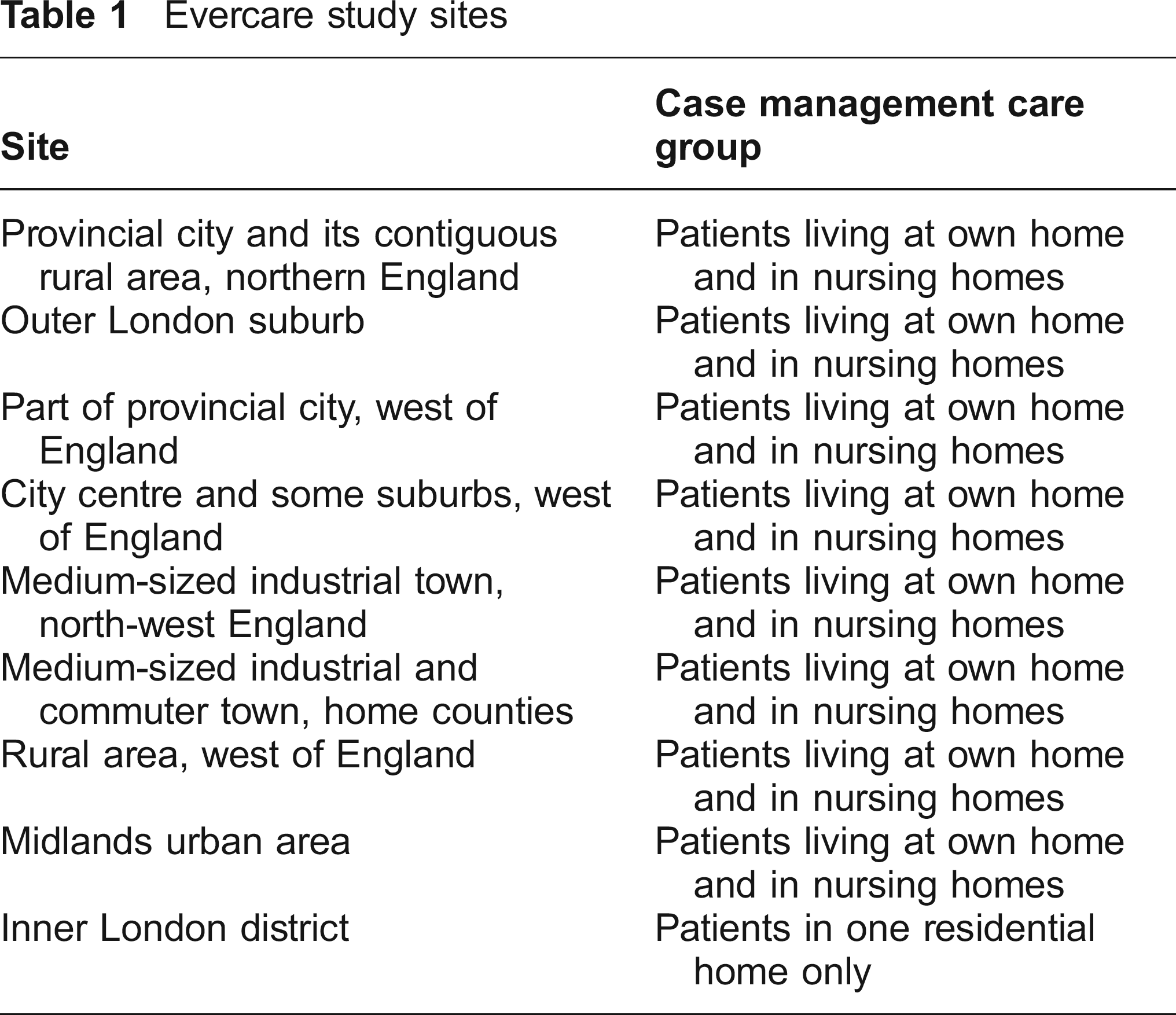
We conducted the study in two phases. To obtain an overview of case management implementation from the outset, the first phase (April 2003–August 2004) comprised case studies of all nine Evercare pilot sites and two non-Evercare models. NHS managers had selected the pilot sites for practical reasons not as a representative sample of Primary Care Trusts (PCTs), although the sites did include urban and rural areas, and were widely dispersed across England. Table 1 briefly characterizes the Evercare sites.
Evercare study sites
We examined the professional press and official websites to discover well-developed alternative case management models as comparators. Table 2 briefly characterizes those sites.
Non-Evercare study sites

Except for the rural non-Evercare case which covered three PCTs, each project was implemented within one PCT. We found substantial variation in how different PCTs implemented even the relatively standardized Evercare model. To investigate more fully what circumstances might cause this variation, we purposively sampled for a second phase of more detailed study (September 2004–December 2005) the polar cases 12 of two Evercare sites which had appeared during the first phase to have made significant progress in implementing case management, two that appeared to be having more difficulty and the most developed non-Evercare site. By then, PCTs were implementing the Community Matron programme and so we added a well-developed instance of this model to the comparison. For that purpose we concentrated on one PCT, although the model was adopted in 13 others in the same region. This stage of research added a deeper understanding of the infrastructural and organizational conditions favouring case management.
We interviewed key informants from UHE and its parent UnitedHealth Group in the USA (10), PCT managers (32), Advanced Primary Nurses (46), general practitioners (10), secondary care staff (4) and five others (Department of Health, US evaluators). These interviewees were purposively selected to cover the range of people who played substantial roles in implementing case management and were likely to be well-informed about the origins, purpose and development of Evercare or alternative projects. They were identified by snowballing from the PCT and UHE project leads who were liaising with the Department of Health. Interviews lasted between 40 minutes and two hours. We used a semi-structured interview schedule based on the categories described below. This approach allowed probing of replies, particularly those which raised issues not covered by the initial analytic framework.
In phase 2 we also interviewed 72 patients (12 per study site) and 52 carers (5–12 per site), selected by community matrons to cover a range of health conditions and residential settings (own home, nursing home, other residential care). UHE commissioned Picker Europe to survey patients on their behalf. 1 We did not duplicate this. However we included selected questions from this survey for use in a (second) semi-structured interview schedule, using the survey questions as a starting point for exploring experiences of case management in greater depth. While the number of interviews was too few for meaningful statistical analysis, the range of responses to each question was broadly similar to the Picker study. All interviews were conducted face-to-face. Except for the Department of Health informants, all interviews were (with the interviewees’ permission) audio-taped and transcribed.
Cases were compared using a two-stage framework analysis.13,14 In the first stage, data from all the available sources about each site were tabulated site by site, 15 using categories suggested by previous studies of case management and health policy implementation in primary care, thereby operationalizing key concepts in the hypotheses stated above. These categories covered:
the social character and health service infrastructure of the locality at the outset of project implementation;
the model of case management actually implemented;
service and resource changes resulting from the project;
roles, activities, perceptions and attitudes of the organizations and individuals most directly affected by the projects.
Tabulation provided a way of triangulating data obtained from the different sources noted below, exposing any apparently contradictory assertions and any gaps in data collection, thereby focusing further data collection. It also helped separate data from interpretation. 10
To reveal any important patterns which the framework had not anticipated, we also analysed the interview data inductively. Three researchers individually organized and coded the data. Only themes and theories identified by all three researchers, and triangulated across the sites, underwent a secondary process of joint advanced coding. This was the main method by which patterns in patient and carer responses were found. New findings which emerged were added to those emerging from the tabulation described above. By comparing the tables across sites, we noted the patterns of similarity and difference between sites and case management models (analytical generalization). These findings were then compared with previously published studies and with the above hypotheses.
These methods have two justifications. As noted, the qualitative findings about the variants, processes and subjective effects of case management complement and help interpret recent quantitative studies of referral impacts. Case study methods are also the method best adapted for describing and explaining how case management is implemented and why different variants have emerged. Collecting data by interview risks distortion due to informants’ selectivity, recall bias, misunderstanding or attempts at self-justification, although triangulation reduces these risks. Patient informants were selected by case managers from among those judged physically and mentally capable of being interviewed. If any selection bias resulted, one might expect it to be towards patients with relatively favourable experiences of case management; but also that it would occur in all the study sites rather than in some but not others. A focus on themes identified by three researchers makes the analytic method more reliable, though it con-comitantly risks omitting possibly important themes about which the researchers did not reach consensus.
Thames Valley Multi-centre Research Ethics Committee gave the study ethical approval. The seven researchers were academics independent of UHE.
Results
We present our findings thematically matching the hypotheses above, starting with features common to all the case models but then noting any substantial differences between Evercare and the alternatives.
Re-engineering primary care
Establishing case management is in itself a limited re-engineering of primary care, but whether any wider re-engineering of primary care resulted is another question.
Establishing case management
The Evercare pilots started in April 2003. One non-Evercare site first invited general practices with the highest rates of unplanned hospital admissions to participate (all but one practice agreed). Elsewhere, the general practices were self-selected. Case managers’ occupational backgrounds were mainly district nurses, nurse practitioners or specialist nurses, but in two non-Evercare sites a minority of case managers were social workers. One of these sites also recruited physiotherapists and a third non-Evercare site chose case managers case by case from whichever profession best suited the patients’ circumstances. The fourth non-Evercare site recruited social workers only. Nurse recruits, designated ‘Advanced Primary Nurses’ (APNs), worked entirely as case managers, but the non-nurses mostly also cared for patients not receiving case management. APNs in the Evercare sites had brief training, were assigned a GP mentor and in some sites geriatrician mentors, which the APNs particularly valued.
Case managers’ next task was to recruit patients. Evercare pilot sites initially selected patients on the basis of age (65+) and two or more emergency admissions in the previous year. All sites attempted, with varying success, to use Hospital Admission Statistics for case-finding, but because they doubted the timeliness or completeness of these data, some general practices also searched practice records manually. In many sites, this selection was the first systematic attempt at finding at-risk patients that had been made. As time progressed, the criteria widened to include patients who were not in contact with regular primary care or community services, but were judged (often by GPs) to be patients who might benefit from case management.
Case managers carried out structured assessments of their patients, planned care, arranged and co-ordinated services, monitored patients at a frequency determined by individual need and arranged ad hoc interventions when incipient deterioration was found. The Evercare pilots initially used standardized instruments for assessment, planning and monitoring care, but elsewhere the corresponding instruments varied in number and scope. As the pilots progressed, even the Evercare sites increasingly adapted the assessment tools and used broader criteria to select patients. Case managers monitored the patients at a frequency determined by patients’ individual risk classification. On these occasions, and at need, case managers did things which patients reported had previously been done by a variety of other primary care staff, including blood pressure checks, physical examinations, ordering tests and investigations, checking medication and ordering equipment. Fuller details are in the final project report. 16 A more detailed study of community matron (nurse APN) caseloads in six of the study sites 17 showed that APNs’ initial caseloads were initially below 10, gradually rising to between 10 and 55 patients per nurse.
The teams on which the case managers could call for support generally included staff from a variety of health and social care backgrounds. As case managers’ knowledge of available services increased, they referred their patients to an increasing range of services. They became more able to find alternatives to hospital admission, although in some sites the case managers regarded their effectiveness as being limited by poor access to services, including a lack of appliances for the patients to use at home and of community alternatives to hospital admission. Communication tended to be particularly poor with GP out-of-hours services, and existing out-of-hours services did not (in the respondents’ opinion) meet the needs of this group of patients, sometimes resulting in unnecessary hospital admission. There was increasing emphasis on psychological support of patients, but, for APNs, also more line management of other staff, leading in some cases to a reduction of direct clinical duties. As their case-loads increased, APNs reported finding it harder to combine the roles of providing pro-active care with general management duties, becoming more reactive in their clinical work. 18 Social workers also experienced a tension between the managerial and the clinical components of the case manager's work.
As the pilots developed, patients were removed from case managers’ caseloads if they improved, although they could refer themselves back if their condition deteriorated. This was unlike the best-known US implementations of the Evercare model 18 which were based on open-ended access to case management. Monitoring of case-managed patients as a group was patchy because of poor information systems in PCTs. Even during the pilot projects, there was relatively little systematic collection of data at PCT level about admissions, and when they were collected such data were often collected specially rather than through PCTs’ routine data collection systems. No PCT gathered control data with which case-managed patients’ experiences could have been compared.
Evercare had a high political profile. Evercare pilot sites, but not the others, received central financial support (although not covering their full costs) and practical assistance from UHE. One apparent benefit from assistance by an organization more experienced in case management than PCTs was a more energetic, faster-paced management style than PCTs usually adopt, with stronger emphasis on collecting data and constructing management information systems to exploit them. UHE provided ready-made proprietary risk assessment and other patient management tools. However, the non-Evercare sites were able to develop case management without such external support, basing their risk assessment tools either on existing instruments or upon publicly available ones.
Impacts on local primary health services
GPs varied in their involvement with, and enthusiasm for, case management. The development of case management was reported by GPs, case managers and patients to have led to a reduction in GP home visiting for case-managed patients, with patients seeing their GP only in circumstances such as serious illness. (No quantified evidence of this effect is however available.) As case managers became more experienced, GPs spent less time liaising with other services and case managers were able to provide more patient care themselves. Case managers, patients and carers all reported many occasions when they had altered medication (in collaboration with the patient's GP) to avoid adverse reactions, coordinated care to reduce fragmentation among services, improved patient functional status and improved quality of life. English law prevents non-doctors fully adopting a GP's role (e.g. for certification of death and for prescribing, although prescribing restrictions were relaxed in 2006). Within that restricted legal competence, however, some of the case managers did take on the roles of monitoring, diagnosing, treating, prescribing and referring patients. To that extent they substituted for, and reduced patients’ reliance on, GPs.
Case management only partly covered the target population in each PCT. Overall nursing structures remained generally unchanged. APNs were employed by the PCT and in some (not all) cases attached to one particular general practice or several. All their working time was usually allocated to case management, which then functioned as a relatively self-contained activity, not integrated into other nursing teams but coordinated with them (and other services) by the same mechanisms (referrals, information exchange) as all primary care providers used. Non-nurse case managers remained with their original employers, retaining patients whom they did not case-manage, their existing team links and access to resources (e.g. respite care). To that extent, the non-nurse case managers appeared better integrated into other community care services than the APNs were. We found no evidence that care pathways beyond the services which case managers themselves provided were much re-designed. Even in the one (Evercare) site where case management was provided at weekends, it had no organizational impact on out-of-hours services. There was confusion in some places about how the case manager role fitted with other services. Case management appeared to be regarded as another add-on service competing for resources rather than as an essential part of the NHS infrastructure. The aim of having 50 patients on the case load of each full-time equivalent APN was often not achieved due to other demands on time from training, education or staff supervision, as well as the unstable risk profile of the patient groups. 17
In their impacts on local primary care services, Evercare and non-Evercare sites were essentially similar. None of the patterns noted in this section differed substantially between the two kinds of site.
Hospital admissions
Case managers, patients and carers described many occasions when the case manager's intervention had prevented hospital admission. An APN said:
‘I believe I have prevented people going in, sometimes just by very minor interventions that I've done within nursing homes … Something like just getting antibiotics in quick when someone's got an infection … we haven't had to do any major rocket science type things to stop people going in, it has been early interventions really.’ (APN, site H)
Elsewhere a carer recounted that:
‘on four occasions I can say, with [the nurse] around has meant he [the patient] didn't have to be admitted to hospital. One was when he'd been in respite, came back completely dehydrated … Then another occasion when he was in respite and came back completely constipated … Another time was when he came back with pneumonia … And then another time was just here where he had a bad asthma attack and then a bad chest infection.’ (Site F Carer 1)
Effective communication between case managers, and other primary and secondary care staff about case management and which patients were being case managed was crucial for preventing unnecessary hospital admissions, but this communication was often patchy. Case managers generally found it harder to liaise effectively with hospital staff and services during patient stays, and were less confident about their ability to reduce length of stay after a patient had been admitted because they found it difficult to influence hospital procedures. In the non-Evercare sites with physiotherapist case managers, hospital and community physiotherapy services were organizationally separate, creating similar barriers to communication as existed between hospital nurse and community APNs.
Both Evercare and non-Evercare sites supplied administrative data showing reductions in unplanned hospital admissions following the introduction of case management, but these data were raw numbers of admissions without any controls or case-mix analyses. The controlled quantitative study 9 showed that in the case of the Evercare sites these differences were not statistically significant. Neither were changes in numbers of emergency bed days or mortality. The above patterns were also essentially similar in Evercare and non-Evercare sites.
Acceptability of case management to patients and carers
Another departure from the well-known Evercare implementation of case management in the USA was that the English projects made case management available to patients living in their own homes and not just those living in nursing homes (Tables 1 and 2). Increased access to health care was the most frequently recurring theme in patient and carer interviews. Patients valued the longer contact time they had with the case manager compared with their GP:
‘You know what GPs are like, don't you? You're in and out in two minutes … he's a good doctor but, as I said, he doesn't get the time to see to you like the nurse does.’ (Site E, patient 8)
Patients also mentioned that they avoided the trouble of accessing a GP:
‘There's no need to see a doctor, she [the APN] does all the arranging for me at the surgery.’ (Site B, patient 4)
‘The one thing I have got is instant access to antibiotics now. Before I used to have to go and book an appointment … Now all I have to do is phone the nurse and she gets in touch direct.’ (Site L, patient 1)
Other patients said of their APN that:
‘She's at the end of that telephone line and all you've got to do is pick it up, and if she's off duty then her phone goes to somebody else of equal capability, and they will look after you the same way.’ (Site E, patient 9)
‘It gives me confidence because I can ring her anytime, you know, any day, not like the doctors, and she'll come to me.’ (Site C, patient 10)
Case managers were also reported as providing access to equipment (e.g. stair lifts) to support living at home. However, the benefits of improved access were offset by the main perceived weakness of the service – its absence at night and, except in one Evercare site, weekends. Out-of-hours GP services were viewed as ineffective in providing for the needs of patients and at preventing hospital admissions.
The main differences in patient access to services depended above all on which resources case managers could refer to. The widest range was reported in the non-Evercare site with physiotherapist and social worker case managers, because their administrative systems gave them direct access to such resources as home equipment and respite places.
Patients and carers often said that another benefit of case management was that the case manager could explain such things as how to take medications:
‘She's very good at explaining. She has shown [patient] how to use all his inhalers properly … she got onto the computer, she got a list made out of everything about the inhalers and brought us a copy.’ (Site L, carer 7)
‘When the nurse came he explained all the tablets, what they did and all that and since then it gives me a boost. It makes you feel better; it makes you feel you're wanted.’ (Site E, patient 6)
Similarly for hospital documents:
‘[regarding] the discharge notes, I said, “Oh, can you tell me what that means?” And she fully explains everything, all the medical jargon; she puts it in words that we can understand.’ (Site C, carer 6)
Improved communication contributed to the psycho-social support which case managers provided and patients particularly valued:
‘It does somehow take a weight off my shoulders, that I have got somebody I can turn to immediately for help.’ (Site L, patient 7)
‘She's sort of given me more confidence, and I certainly haven't fallen over since she started coming, so I think carefully before I do anything and I'm more careful.’ (Site E, patient 5)
Carers responded similarly:
‘To me it's like it lifts like a weight off my shoulders … if anything happens to [patient], you know, like she feels ill, I can get on the phone to the nurse … and if she thinks it's serious she'll come straight down and check her out herself.’ (Site L, carer 4)
‘I really felt that she was my friend, she certainly acted that way, I mean her chief concern was the patient but I also felt she was on my side. That sounds silly but it's true.’ (Site H, Carer 3)
In general, patients reported high levels of satisfaction with both the service and its impact on their own health, regardless of the specific interventions carried out and regardless of whether case management was provided through Evercare or an alternative model. 19 All patients and almost all carers described the service as either ‘very good’ or ‘excellent’. Patients were often anxious that no-one should ‘take their nurse away’ and were often reluctant to be discharged from case management.
We found no substantial qualitative differences between the sites in terms of the above patterns of response. Among the case management models studied, none was obviously superior in terms of acceptability to stakeholders, but all models were superior to the absence of case management.
Discussion
Our conclusions about the foregoing hypotheses (assumptions of policy-makers) are necessarily provisional because case management continues to develop in the English NHS. We found no evidence that the Evercare project stimulated wider local re-engineering of primary and secondary care for older people. Re-engineering was essentially limited to the introduction of case management itself. Being a greater departure from previous practice, one might even argue that such re-engineering was greater in the non-Evercare sites which recruited non-nurse case managers. Central funding gave the Evercare sites greater external managerial, especially information management, support than the other sites. Although a wider re-engineering of primary care services did not materialize, the Evercare project did trigger debate and re-appraisal of NHS community nursing practice and the role of primary care.
The many examples which respondents gave of unplanned hospital admissions which had been avoided apparently contradict the quantitative analysis which showed no significant effect on admissions. 9 One possible explanation is that case management increased case-finding, bringing patients not previously in regular contact with primary care services into the Evercare pilots. A similar pattern was reported in the Australian co-ordinated care trials. 20 In all our study sites, case-finding systems were under-developed. If case-finding were to become more effective in future, increased case numbers might outweigh any reduction in inpatient days per patient, increasing access to primary but also to hospital care. For Evercare sites, the balance of evidence was against the hypothesis that case management would reduce unplanned hospital admissions by substituting case management in primary care, and the same applies to the other sites.
Access to case management added a frequency of contact, regular monitoring and knowledge of a range of referral options that had not recently been provided by GPs or anyone else. Case managers, patients and carers reported impacts on patients in terms of improved quality of life (better communication and psycho-social support) and on the NHS in terms of reduced GP workload. Case management was highly acceptable to the key stakeholders involved, especially patients and carers. Both Evercare and non-Evercare models were popular.
The conditions which appeared to make case management more effective were: reliable case-finding systems; providing case management out-of-hours; full exploitation of population-level data about case-managed patients; varied and sufficient community based services and resources (appliances, respite care, etc.) that case managers could call upon; effective liaison with hospital ward staff; and minimizing APNs’ managerial workload. The main differences between Evercare and the other case management models were in implementation and management information support, in which the Evercare model had some clear advantages; in the choice of professions to undertake the case manager role, a question which requires further research; and whether to use proprietary or published risk assessment systems, a comparison which in our opinion favours the non-Evercare models because the published systems have explicitly undergone independent critical scientific peer review, and are usually available free of charge and with fewer restrictions on how they may be used.
Certain policy implications follow from these findings. While the Evercare project was under way, it was decided to ‘roll out’ case management across the English NHS with APNs, now designated ‘community matrons’, as the case managers. While the community matron system has substantially extended case management in England, there is still scope to invent and evaluate further variants, in particular to rethink primary care pathways more radically and systematically. Admission reduction policies remain poorly coordinated between primary and hospital care providers. The English NHS pays hospitals per case treated, an incentive to hospitals to increase admissions which appears to conflict with the aims of case management. Case management had the paradoxical effect of increasing patients’ independence in the sense of capacity to continue living in their own homes while increasing their practical and psychological dependence on their case manager, shown by their reluctance to leave the scheme when their health improved. These findings raise questions about the purposes of case management. Future research and implementation resources should focus on comparing how different professions function as case managers, refining patient risk profiling tools, 21 exploring different ways of providing care in the community and strengthening care coordination between primary and secondary care so as to avoid unnecessary admissions. A high priority must also be to strengthen PCT information systems so that they can more readily support routine evaluations of this type of innovation.
Footnotes
Acknowledgement
The study was funded from the Department of Health core grant to the National Primary Care Research and Development Centre. The views stated above are the authors’ own and not necessarily those of the Department of Health.