
Abstract
Objectives
To evaluate the impact of critical care outreach services on the delivery and organization of hospital care from the perspective of staff working in acute hospitals.
Methods
One hundred semi-structured interviews were undertaken with hospital staff who were either members of, or who came into contact with, the outreach service in eight hospitals in England.
Results
Outreach services had two main impacts on the delivery and organization of hospital care, reflecting the organizational and educational aims of the policy. First, on the organization of patient care: it was suggested that care was more timely, there were fewer referrals to the intensive care unit (ICU) and ICUs felt more able to discharge patients to hospital wards. There were also perceived to be improved links between ward nurses and medical teams and improved morale among ICU nurses. Second, on the confidence and skills of ward staff (nurses and junior doctors): increased contact on the wards resulted in more opportunities to share critical care skills. However, there remained concerns about the sustainability of improved skills and some respondents felt that junior doctors were becoming de-skilled.
Conclusion
Critical care outreach services have had a positive impact on the delivery and organization of hospital care. In attempting to share critical care skills, however, these services can experience a tension between the aims of service delivery and education - a tension which is partly resolved by sharing skills in the clinical and organizational context of direct patient care.
Introduction
This paper aims to contribute to our understanding of organizational interventions through analysis of the impact of critical care outreach services on the delivery and organization of hospital care. Outreach services are usually composed of teams of nurses trained in critical care who are available to provide clinical support or advice on hospital wards when the health of a patient is deteriorating (or at risk of deteriorating). Their establishment in the NHS in England and Wales was heralded in May 2001 with the publication of Comprehensive Critical Care, 1 which identified three essential objectives: first, to avert admissions to critical care units; second, to enable discharges from critical care units; and third, to share critical care skills with ward staff. While there is some overlap between these objectives, the first two are primarily organizational and the third primarily educational.
Documents that accompanied the publication of Comprehensive Critical Care promised an additional £150 million, with the expectation that this money would fund approximately 250 extra intensive care beds and 50 outreach services. 2 Several factors (over the short and long term) had combined to make this significant investment a political necessity. Over the long term, intensive care doctors were concerned that the labour-intensive, highly technical and expensive service of intensive care was being excessively rationed,3,4 and were therefore beginning to ask questions about the most effective and efficient ways of organizing intensive care. 5 Outreach services appeared to offer a way of providing critical care which was more cost-effective than extra intensive care beds. 6
In the shorter term, in the late 1990s, a problem of ‘suboptimal care’ on hospital wards was reported, 7 which formed an important part of the background for the media reaction to the ‘winter crisis’ of 1999– 2000. During that Christmas and New Year period a shortage of intensive care unit (ICU) beds in England was widely reported and criticized in the national press; 8 at one point only 11 intensive care beds were available for new patients. 9 The press noted that Britain had fewer beds per head of population than other developed countries. Within a few months further scientific evidence had been published highlighting the pressure on ICUs: premature discharges from ICUs were causing excess mortality. 10 The announcement of extra funding for intensive care beds and outreach services followed within a few months.
Outreach services were seen as particularly able to solve the problem of ‘suboptimal care’ following reports of Medical Emergency Teams 11 and Patient At-Risk Teams. 12 These early models of critical care outreach aimed to identify patients at risk of developing critical illness and initiate early intervention where necessary. The concept of outreach services was supported by the Department of Health, 2 the Intensive Care Society, 13 the Royal College of Physicians14,15 and the Audit Commission. 6 However, no documentation specified a model for critical care outreach and as a result there has been considerable variation in how such services have been developed in NHS hospitals.16,17
The substantial financial investment in the development of outreach services necessitates not only evaluation in terms of patient outcomes18,19 but also from the perspective of hospital staff who have encountered the service – especially since outreach services are an intervention with likely impacts at organizational levels as well as on patient care. A few studies have evaluated outreach services from the perspective of hospital staff, although these have focused exclusively on nurses and have been conducted at only one or two sites.20–22 In this paper we draw on qualitative interviews data from hospital staff in eight English hospitals to evaluate the impact of outreach services on the organization of patient care (i.e. the original policy's organizational objectives) and on the skills and confidence of ward staff (i.e. the original policy's educational objective).
The phrase ‘critical care without walls’ 23 has achieved widespread use subsequent to the original policy, reflecting the idea that the clinical skills and expertise of critical care nurses should not be geographically restricted to ICUs. Our analysis also demonstrates the social and organizational aspects of this phrase: outreach services act as a crucial link between ICUs and hospital wards, and between staff on hospital wards and medical teams.
Methods
The principal data collection method was semi-structured interviews, 24 conducted in eight hospitals, with key stakeholders from different locales and occupations. A two-stage sampling process selected, first, hospitals and second, an appropriate range of interviewees. The hospitals were selected following a national survey of critical care outreach services. 17 The survey results described the population of outreach services and enabled a sampling frame to be derived such that differing types of outreach service could be selected. The selection of hospitals is discussed in more detail in the project report. 18 Briefly, we aimed to achieve maximum variation 25 on various dimensions of outreach service, such as relative prioritization given to service aims, whether the service was nursing or medical led, its size and operating hours, and the size or teaching status of the hospital in which it operated. For the key impacts reported in this paper, there were few site-related differences and where they have occurred they are highlighted. Multicentre Research Ethics Committee approval was granted, as was NHS Trust R&D approval at each site prior to data collection.
In each hospital short periods of non-participant observation enabled a stratified purposeful sample 24 of interviewees to be selected on the basis of contact with the outreach service. Interviewees were fully informed of the purpose of the study, provided with information sheets and given time to consider whether they wished to participate. All interviewees completed consent forms.
The semi-structured interviews followed a topic guide, the final version of which can be seen in Box 1. The topic guide was originally derived from the project brief; some questions elicited little data and so were excluded from later interviews in order to focus progressively the data collection and analysis on the salient themes. It should also be noted that the interviews were conversational in style and interviewees often volunteered other information. Interviews were audio-recorded and transcribed. Transcriptions were checked for accuracy and then analysed using qualitative analysis software (QSR N6), initially coding the data (inductively) to derive thematic categories. These categories were then inspected in order to combine, compare and link categories where appropriate. This paper reports the analysis derived from the semi-structured interviews conducted with 100 health care workers (Table 1).
Interview sample
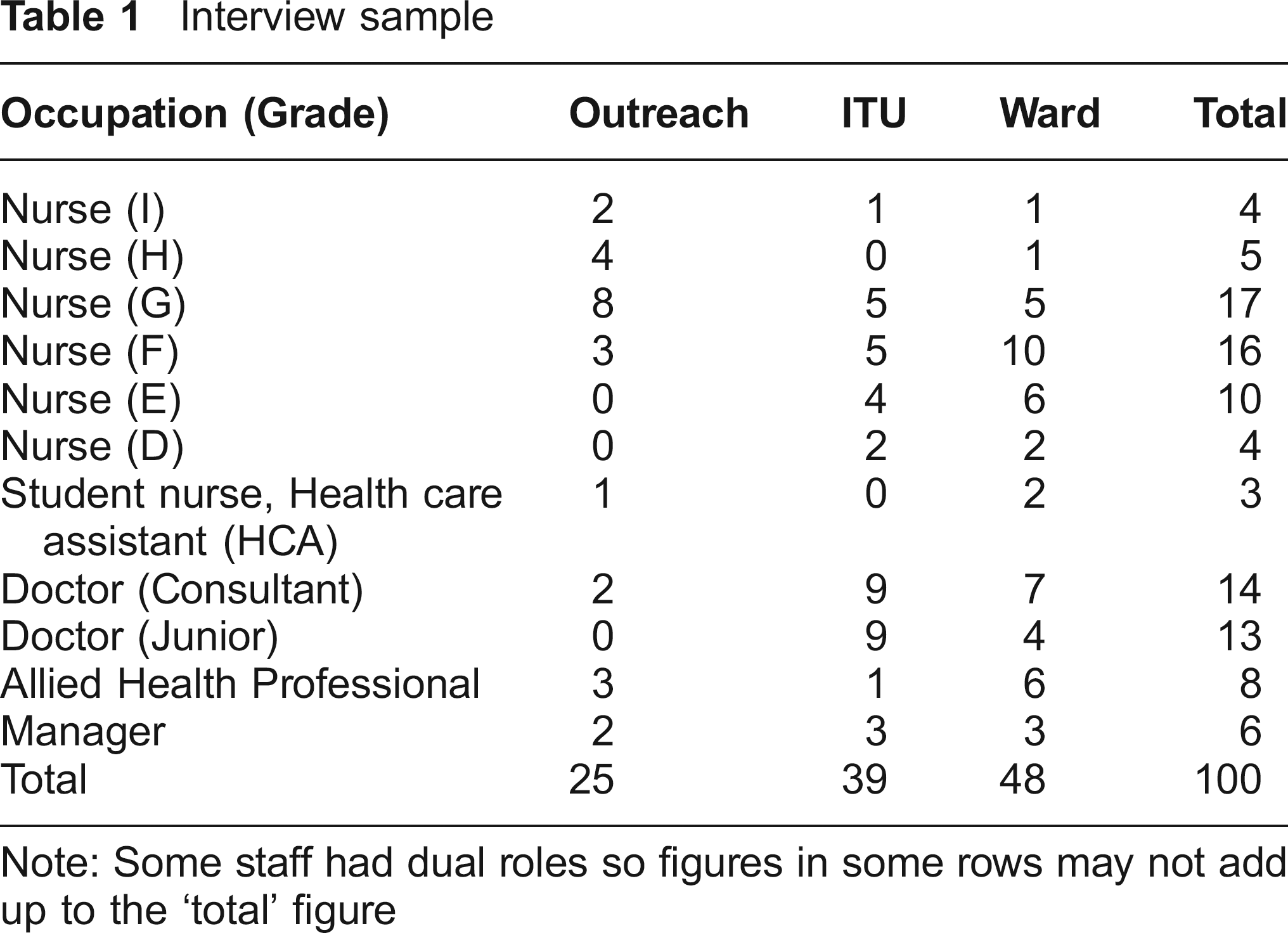
Note: Some staff had dual roles so figures in some rows may not add up to the ‘total’ figure
Results
Impact on the organization of patient care
The principal contributions of outreach services to patient care can be seen in the following comments of a ward nurse:
They're looking at that patient and… they assess them with you, and then what often happens is they'll get on the phone to their registrar, which of course is not our job as nurses to do. Our doctors have to feel the element of urgency in order to contact the ICU registrar themselves… But the outreach nurses can do that… So what could take 24 hours potentially in a poorly handled situation, only takes four or five. (E Grade Nurse, Ward)
Summary of topics discussed in interview
Whether the training and sharing of critical care skills was implicit or explicit
Whether outreach staff and ward staff felt appropriately trained and educated in caring for critically ill patients
In what ways gathering information from the ward may have contributed to improved critical care services
Staffing issues (on critical care outreach service)
Impact on other hospital services and community services
Perceived effectiveness of outreach services on: – sharing skills;
improving communication and teamwork;
enhancing training opportunities;
improving critical care services
By this account, the particular advantage of outreach nurses is that they can communicate directly with ICU doctors, facilitating speedier patient assessment and more timely admission to the ICU. (The comments also show how they cross organizational and professional boundaries, which is something to which we return at the end of this section).
From the point of view of the ICU, outreach had fulfilled the first organizational objective of the policy, and averted inappropriate admissions to ICU:
I think this is one of [outreach's] strengths. I think it's hard to sort out patients that are deemed not appropriate to admit [to ICU], you know, patients that are end-stage lung disease or renal disease… I think [outreach nurses] often… try and get the teams to decide… what is most appropriate… for the patient… Making a decision about not resuscitating or making a decision about limits of critical care. (G grade nurse, ICU)
So in some instances outreach nurses had a role in clinical decision-making (e.g. ‘Do Not Attempt Resuscitation’ orders); the extra knowledge, which outreach nurses can confidently assert, is that intensive care may not always be in a patient's best interests. They can be seen, then, to encourage doctors to make timely and appropriate decisions.
At most study sites referrals to ICU from the outreach service were regarded as appropriate and it was felt that outreach nurses’ judgement was trustworthy. It was commented that outreach nurses made good use of high dependency areas, for example admitting patients for a short period rather than transferring them to the ICU. (A minority of doctors held a dissenting view that there had been an unwarranted increase in critical care use, with over-cautious outreach nurses referring patients who would not benefit critical care).
Care after discharge from ICU was the second of the original policy objectives. It was felt that outreach services made it safer to discharge some patients from intensive care:
It's like a proper finish, a proper end to the care that we started on ICU really, instead of just leaving the ward staff to deal with still poorly patients who not only have got physical problems but they're confused and agitated… At least, with outreach input there's been the support (Nurse, ICU follow-up)
This was felt to be especially true for patients with a tra-cheostemy, which according to one medical consultant ‘frighten’ ward nurses. A large proportion of ward nurses recognized that patients discharged from ICU have particular problems, and they valued the follow-up provided by outreach nurses who could answer queries and detect common problems. This extra support also meant that ICU nurses could reassure patients and relatives before their transfer to the ward:
Patients [are]… used to such high one-to-one nursing care where everything is done… for them… they're worried what's going to happen [when transferred to the ward]… We can actually reassure them just to say ‘you've still got the ICU link coming to see you, you're getting better’, and give that reassurance. (H grade nurse, outreach)
An indirect benefit of outreach services was that information about the progress of former intensive care patients could be communicated back to ICU nurses (formerly, there could be little news about a patient once they had left the unit). This contributed towards an improvement in morale (not anticipated, or at least not mentioned, in the original policy):
[ICU nurses] love the follow-up, they're always asking us who's doing what, how's the patient getting on, if they can come out with us and see how they are, so the follow-up aspect of it's really good. (G grade nurse, outreach)
Furthermore, ICU nurses were also more aware of the situation of ward staff, as outreach nurses could convey to ICU staff some of the difficulties experienced by ward nurses. (Some ICU nurses even commented that this information had made them appreciate ‘how lucky they were’ to work in the ICU.) For their part, some ward staff also stated they were now less afraid to contact ICU (although some did remain intimidated by the idea of ICU). The reality of patients’ experiences of intensive care was also becoming clearer to staff on the wards.
The introduction of outreach services also provided a crucial link from ward nurses to medical teams. Ward nurses described outreach as invaluable in contacting doctors. This was thought to be because they had more authority and experience with critically ill patients than ward nurses:
Having that force behind you of somebody who, yes they are a nurse but they're a specialist nurse, standing there and saying well, what the heck do you think you're doing, get someone in here, put a line in, we need access, we need blood gases… It just gives you that extra weight because although you think you know what needs to be done, sometimes it's very, very difficult to push the urgency… When someone's really acutely unwell they really pitch in… (E grade nurse, ward)
The physical metaphors (‘force’, ‘extra weight’, ‘push the urgency’) are indicative of a sense of inertia in certain aspects of hospital care, which outreach nurses are able to overcome through their enhanced authority. They can, then, bridge gaps between the medical staff and ward nurses. (An added advantage of doctor-led services – usually led by a senior ICU consultant – was that they were better able to communicate with other ICU doctors and initiate consultant-to-consultant referrals.)
Another aspect to outreach's contribution is that ‘outsiders’ can help to protect the working relationship between ward nurses and doctors:
I've had [outreach] come over and tell the doctor what needs to be done… [which] stops that breakdown in your relationship with your medical team. Sometimes somebody from outside that's quite objective… saying, ‘well, no, the nurse is right’ stops you getting into a loggerhead situation… (F grade nurse, ward)
A more problematic aspect of outreach services was related to patient ownership. It was reported that medical or surgical teams could at times be unwilling to relinquish responsibility for their patients (one doctor characterized outreach as the ‘critical interference team’). The changes to cross-professional relations were not universally welcomed by intensive care doctors, either:
In the past, where we would get the call ourselves directly from the medical consultant or surgical consultant, we now get calls from outreach… I would prefer the referral to have been from consultant to consultant… Now it tends to be… junior trainees calling the outreach team, outreach getting involved and they call us without the consultant knowing about the case… I don't think that's how it should be. (Consultant anaesthetist, ICU)
Overall, though, outreach services were felt to improve interprofessional relations, principally by being a communication link between ward nurses and medical staff of all grades.
Impact on ward staff
The predominant theme in interviews with ward staff was confidence, related to reassurance and a sense of empowerment. Reassurance was said to derive from the support of accessible critical care trained nurses:
Knowing that there's somebody on the end of the phone that will come and help if you need them, knowing that person's there just makes all the difference. (F grade nurse, ward and outreach)
Many interviewees gave examples of outreach nurses’ ‘professional and calm’ approach: obviously a great reassurance when a ward nurse is facing a critically ill or rapidly deteriorating patient. A sense of empowerment was thought to derive from enhanced knowledge through education and training:
I think I'm more skilled because I'm more educated as to what's going on. Like the other day - they anaesthetized and intubated somebody on the ward… the [outreach nurse] was explaining everything, each step of the way. I felt better for it, I felt more educated, more enlightened and I was more aware of what was going on. (E grade nurse, ward)
Formal education and training sessions often encompassed the principles and practice of physiological track and trigger scores. These scores, usually based on sets of physiological parameters, are intended to detect patients at risk of deteriorating. 26 However, as several staff suggested, knowing how to accurately derive and interpret a score is not the same as actually doing it:
A lot of people still don't do respiration rate which is one of the first signs… They can't stand there for a minute to count someone's [respiratory rate]… (Health care assistant, ward)
Some outreach staff interviewed felt that apathy on the part of ward nurses was responsible for the apparent lack of success of this kind of training. Other issues were also mentioned, for example, staff needing to develop enough confidence to use and practice their new knowledge.
The great advantage of a score is that it provides objective, quantifiable information which can easily be passed on to others. However, organizational deficiencies were mentioned which can prevent the successful implementation of track and trigger systems on patient care. For example, one consultant described communication breakdown within the medical teams,
It goes up through the chain of command within the medical team that's responsible for patient care but we find that it gets blocked at a fairly low, junior level… Some junior doctors are afraid to call a consultant, or the consultant's away, and cross-cover consultant responsibility falls apart. (Consultant, outreach)
The overall picture is one of moderate success in enhancing the basic knowledge of ward-based staff. This enhanced knowledge was on occasion dissipated by allegedly dysfunctional hospital organization, particularly among medical teams.
Moving from education in basic knowledge to training for practical skills, more sceptical views were expressed:
‘Critical care without walls’ sounds great but to install the skills into individuals, yes you can do that but to maintain it is very difficult and how you maintain those skills in ward nurses, I don't think it's possible at all, to make ward nurses critical care nurses… (I grade nurse, ward)
I'm not sure I honestly believe that you can give ward nurses HDU skills in one study day. (H grade nurse, outreach)
This suggests that improvements in certain kinds of ‘critical care skills’ on the wards may not be sustainable. A similar comment, reflecting an understanding of the situation of ward staff, was provided by one nurse consultant:
They've got ten other patients to look after or they've got to do the drug round, they've got this, that or the other to do but then they don't learn the skills. (Nurse consultant, outreach)
By contrast, informal training at the patients’ beside, while directly implementing interventions for critically ill (or deteriorating) patients, offered contextualized opportunities for outreach nurses to explain their actions. On these occasions, outreach nurses could encourage interested ward staff to develop and practise relevant skills. This was particularly the case for junior doctors, many of whom stated that the outreach service was invaluable in helping them acquire specialist skills (e.g. blood gas analysis, monitoring patients, setting up specialist equipment) and increase their knowledge and confidence.
That said, however, some junior doctors could feel sidelined by outreach nurses, and some more senior medical staff felt that the presence of outreach services ‘de-skilled’ junior doctors.
I do quite strongly feel that [outreach] is de-skilling [junior doctors]… As it is, an awful lot of these acutely ill patients are swept up by the outreach staff and [junior doctors] don't see them so much… I think it's fantastic for patient care and I think it facilitates the whole kind of transfer ICU/ward to ward/ICU but somewhere in the back of my mind is that junior doctors should be doing a bit more of this role and they're not. (Junior doctor, ICU)
The ambivalence here (the respondent acknowledges that outreach is ‘fantastic for patient care’) highlights the tension between the educational and service delivery objectives of outreach services. The blame for the alleged loss of skills by junior doctors cannot be placed entirely on outreach services. It is, after all, current health policy to promote flexibility among the health care workforce,27,28 and many other skills are being ‘lost’ by junior doctors (e.g. inserting cannulas, taking bloods). But additionally, as one junior doctor candidly admitted, ward nurses and doctors sometimes called the outreach service without considering other options:
Sometimes before thinking things through yourself, you can pick up the phone… If you'd actually looked… instead of panicking… and spoken to your senior rather than calling critical outreach team, it might have saved some time and you might have learnt something more yourself! (Junior doctor, ward)
Discussion
This study has identified two main areas where outreach services have had an impact on the service delivery and organization of hospital care. With regard to the organization of patient care, positive impacts of outreach services were that they provided timely input into decisions regarding optimal care; there seemed to be fewer ICU referrals and ICU staff had more confidence to discharge patients to the ward. An unanticipated impact of the outreach service was that informal communication about former intensive care patients led to improved morale for ICU nurses. The second main impact of outreach services was to reassure and empower ward staff. The perceived empowerment of junior staff was attributed to increased education and training. Some problems, though, were highlighted: outreach services were accused of de-skilling junior doctors, and there seemed to be little sustained improvement in clinical skills. These aspects of the educational objective of outreach services require further comment.
It appears that while outreach services could be said to be meeting some of their educational objectives, several factors have hampered the implementation of this learning in routine clinical practice: a lack of confidence on the part of ward nurses; lack of opportunity to use skills; pressure of other work on the ward; poor organizational or medical communication. Overall, the benefit of learning advanced clinical skills is dependent on whether ward-based staff have opportunities to continue to use these skills routinely.
Outreach services face the classic conundrum of a tension between service delivery and education. On the one hand, training which enhances clinical skills is seen as a long-term benefit. On the other hand, treatment for the sickest patients needs to be provided. The logic of education and training – that as skill levels are raised on wards the pressure on ICUs and outreach services will reduce – is persuasive. It does, though, need to be recognized that the expert skill of outreach nurses is founded on, and enhanced by, daily practical experience of treating critically ill patients. It is unreasonable to expect ward nurses to attain a similar level of expertise and critical care skills when they do not have these daily practical experiences. ‘Critical care without walls’ 23 suggests that the clinical skills and expertise of critical care nurses and doctors should not be geographically restricted to ICUs. The question, left open by the original objectives of Comprehensive Critical Care, 1 is whether operationally these skills are retained in the ICU-trained individuals of the outreach service, or transferred to ward staff. We suggest that whereas the wholesale transfer of skills may not be possible, the enhancement of a limited set of skills of ward staff will be more successful in situations where it occurs in the context of direct patient care rather than in separate, formal study sessions.
To conclude, we suggest two general lessons. First, the findings suggest that in many instances an enhanced role for nursing is of general benefit to service delivery, not least in terms of the improved links between different teams and locations within the hospital. Second, we note that the effect of formal training sessions were not felt to be as long-lasting as the sense of empowerment, greater understanding and practical skills learnt in the immediate context of patient care. Thus the sustainability of educational interventions in health care is dependent on the clinical and organizational context; where educational and organizational interventions are highly coupled the benefit is more likely to be longer lasting.
Footnotes
Acknowledgements
We are grateful to our interviewees for their generosity, to two reviewers for their helpful comments, and to the following for their advice and support: Sheila Harvey, Kathy Rowan, Ann McDonnell, Gareth Parry and Carol Ball. The research was funded by the NHS R&D Service Delivery & Organisation Programme (Grant Number SDO/74/2004).