
Abstract
Improved population health depends on changing behaviour: of those who are healthy (e.g. stopping smoking), those who are ill (e.g. adhering to health advice) and those delivering health care. To design more effective behaviour change interventions, we need more investment in developing the scientific methods for studying behaviour change. Behavioural science is relevant to all phases of the process of implementing evidence-based health care: developing evidence through primary studies, synthesizing the findings in systematic reviews, translating evidence into guidelines and practice recommendations, and implementing these in practice. ‘Behaviour change: Implementation and Health’, the last research programme to be funded within the MRC HSRC, aimed to develop innovative ways of applying theories and techniques of behaviour change to understand and improve the implementation of evidence-based practice, as a key step to improving health. It focused on four areas of study that apply behaviour change theory:
defining and developing a taxonomy of behaviour change techniques to allow replication of studies and the possibility of accumulating evidence; conducting systematic reviews, by categorizing and synthesizing interventions on the basis of behaviour change theory; investigating the process by which evidence is translated into guideline recommendations for practice; developing a theoretical framework to apply to understanding implementation problems and designing interventions.
This work will contribute to advancing the science of behaviour change by providing tools for conceptualizing and defining intervention content, and linking techniques of behaviour change to their theoretical base.
Introduction
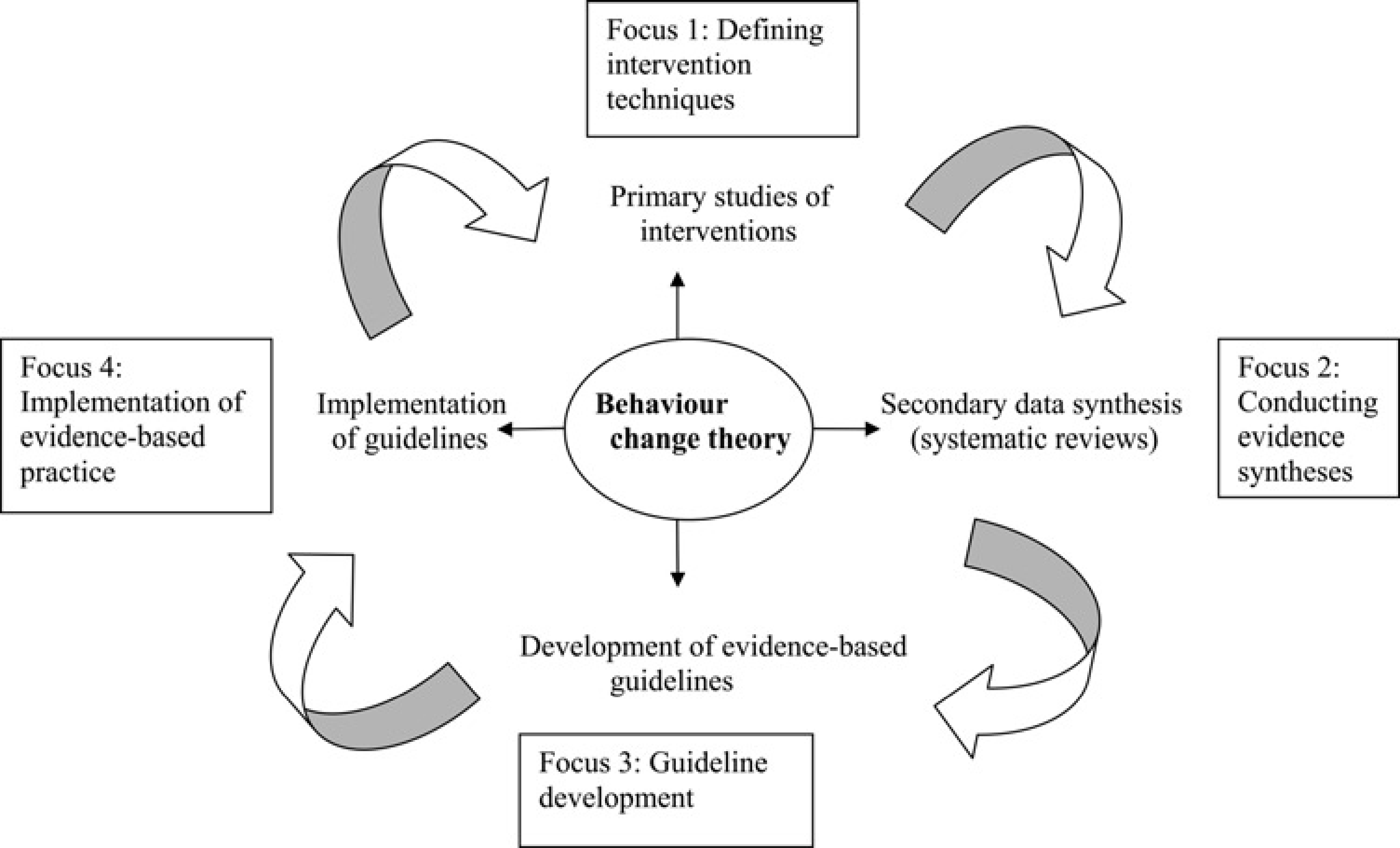
The last research programme to be funded within the MRC HSRC, ‘Behaviour change: Implementation and Health’ aimed to develop innovative ways of applying theories and techniques of behaviour change to understand and improve the implementation of evidence-based practice, as a key step to improving health. Behaviour change theory is applied to advancing methods in intervention and implementation research, with a focus on four areas:
Defining intervention techniques;
Conducting evidence syntheses;
Guideline development;
Implementing evidence-based practice.
Progress in tackling today's major health and health care problems requires changes in behaviour pat-terns.1,2 There are three main groups of people who are targets for behaviour change interventions:
Those who are healthy benefit from reducing behavioural risk factors for ill health (e.g. smoking) and from increasing protective behaviours (e.g. engaging with screening programmes);
Those who are ill benefit from adjusting their behaviour to their circumstances (e.g. keeping active while suffering back pain) or following behavioural advice to prevent deterioration (e.g. taking medication as prescribed);
Health professionals and others responsible for delivering effective, evidence-based health care.
Although individual behaviour is the ultimate target for change, effective interventions to change behaviour may be delivered at population, community, organizational or individual levels. 3 For example, effective interventions to tackle the biggest behavioural threat to public health, smoking, range from population-wide mass media to stop smoking courses for individuals. 4
This paper discusses the limitations of current approaches to developing and evaluating behaviour change interventions and the beginnings of a research programme which has sought to achieve a sea change in the way that this is done.
Limitations of current approaches
Studies of behaviour change interventions aimed at self-protective or health enhancing behaviours have so far had mixed results. There is clear evidence for efficacy of some interventions to aid smoking cessation and curb excessive alcohol consumption, such as brief medical advice and telephone counselling. However, in none of these cases is it known what the active ingredients are. In addition, there is quite a high degree of heterogeneity and the effects may well depend on context and mode of delivery. In other cases, such as promoting physical activity, attending screening and adopting a healthier diet, the results of intervention evaluations have been inconsistent. 3
Similarly, despite substantial investment in health research, the implementation of research findings into practice has been slow and haphazard. For example, studies in the United States and the Netherlands, found that 30–40% of patients did not receive evidence-based health care and 20–25% received care that was unnecessary or even harmful.5,6 There have been hundreds of studies of interventions aiming to change health care professionals’ behaviour to bring it into line with evidence-based recommendations. These have found small effects or no effect at all, with no clear pattern of results favouring particular methods. 7
Thus progress in this important field has been slow and in no way reflects the urgency of the need to improve the effectiveness and delivery of behaviour change interventions to prevent suffering and premature death on a massive scale. There have been two reasons for the slow progress. First, the size of the investment has been extremely small in relation to the scale of the problem. Currently, only 0.5% of medical research funding in the UK focuses on behaviour change interventions. Second, intervention development and evaluation appear to be largely based on simple, mostly unstated models of human behaviour or, when interventions are informed by theory, the connection is tenuous and intuitive rather than systematic. 8 This means that each new intervention and each new evaluation occurs in isolation and there is no opportunity to build an incrementally improving technology of behaviour change.
A better approach
If the benefits of current investment in behaviour change interventions are to be realized, it is imperative that scientific knowledge about behaviour and behaviour change be drawn on in designing and evaluating such interventions. This is as true of secondary research as it is of primary research. For example, in order to categorize interventions for evidence syntheses, it is necessary to know the details of the component techniques that comprise interventions and the likely mechanisms by which any effects are achieved.
Getting evidence into practice requires translating findings from systematic reviews of evidence into recommendations for practice. This process, key to high quality health care, also depends on the behaviour of individuals, usually as part of guideline development groups. This important part of the implementation process warrants investigation if the aim of effective, evidence-based health care is to be achieved. The final stage, implementing recommendations in practice, also depends on behaviour change. This will allow theoretically grounded methods of categorizing behaviour change interventions in systematic reviews. This, in turn, will foster understanding of how interventions bring about change, the generalizability of the intervention and the design of more effective interventions.
One reason for the infrequent application of behaviour change theories to health and implementation research may be the plethora of potentially relevant theories, many with overlapping constructs, and the lack of guidance as to how to select theories and apply them to intervention development. Work is needed to make behaviour change theory accessible and useable to the range of disciplines involved in designing and evaluating interventions. While there are general laws of human behaviour and of behaviour change, an important area of development for theory is to encapsulate differences between behaviours. This requires conceptualizing behaviour, that is, the key dimensions of differences between behaviours that influence their propensity to change in different contexts. Similarly, while many of the principles of behaviour change apply across groups (e.g. health professionals, general public), there is a need to understand differences between groups and individuals in relation to different types of intervention.
The programme of research
Behavioural science is relevant to all phases of the process of implementing evidence-based health care:
Developing evidence through primary studies;
Synthesizing the findings in systematic reviews;
Translating evidence into guidelines and practice recommendations;
Implementing these in practice.
This programme of research aims to improve the science of behaviour change and its application in four stages of a cycle of evidence production and implementation (Figure 1). It puts theory centre-stage in the cycle, informing ways in which primary data are generated, synthesized into evidence and translated into guidelines to facilitate implementation of evidence-based practice. Experiences of implementation generate further primary studies, hence the cycle. Mapping onto these stages are four areas of study outlined below.
Implementation of evidence-based practice: a virtuous cycle and four areas of research
Behaviour change theory: defining intervention techniques
Scientific knowledge is generated by careful replication of studies and linking empirical facts with explanatory theories. Those studying, designing or delivering complex behavioural interventions seldom describe them in enough detail to replicate, far less to establish, their active ingredients and underlying mechanisms. 9 Advancing the science of behaviour change requires clear definitions of intervention techniques, with labels that are understood across discipline and country. It also requires clear links between defined intervention techniques and theoretical mechanisms of change. This will strengthen the basis for understanding how successful interventions have their effect, that is, what processes are responsible for observed changes in which contexts. This is a prerequisite for primary and secondary research to build the cumulative knowledge base necessary for designing and delivering more effective behaviour change interventions.
Just as medicines are described in detail in the British National Formulary, there is a need for a similar listing, or taxonomy, of behaviour change techniques to improve the reporting and replication of the complex interventions often required to change behaviour. Work has begun to construct such a taxonomy, using inductive and consensus methods to analyse systematic reviews of behaviour change interventions and relevant text books.8,10 This has generated a list of 26 techniques representing different levels of complexity and generality, and demonstrating good inter-rater reliability. 11
Initial data suggest that the need for such a taxonomy is even greater for behavioural interventions than for pharmacological interventions. At a workshop attended by 26 researchers from a variety of disciplines, we assessed the potential added value of using the taxo-nomy. 12 They were less confident about being able to replicate behavioural interventions compared with pharmacological interventions (t = 6.45, p < 0.0001) and judged that they would need more information in order to replicate them (U = 35.5, p = 0.022). Providing doctors and allied health professionals with a more detailed protocol description did not increase confidence, suggesting that more information does not, per se, make intervention descriptions easier to interpret and use for replication. Our draft taxonomy of techniques was seen as an important tool for this purpose (mean rating 4.4 on a scale of 0–5, with 5 most relevant to needs).
An example of applying this taxonomy comes from a review of interventions to increase physical activity and healthy eating in the general population. 10 The interventions were primarily aimed at improving self-regulation skills using behavioural and/or cognitive techniques, some in combination with social and/or environmental and policy change strategies. Overall, the 84 comparisons had an effect size of 0.37, with substantial heterogeneity between individual studies. The interventions comprised, on average, six techniques (ranging from 1 to 14). When the effects of individual techniques were investigated by meta-regression, studies that included the technique of self-monitoring were found to have a large effect size of 0.57, in contrast to those that did not (effect size of 0.25). Without this fine-grained taxonomy-based analysis, this review would not have been able to shed light on the effective components within these mainly multi-faceted interventions.
Next steps in this area of work are to validate and refine the list and identify underlying theoretical principles to produce a taxonomy with a hierarchically organized internal structure. There is increasing recognition that behaviour change interventions should be based on theories of behaviour and behaviour change. The UK Medical Research Council's framework for developing and evaluating complex interventions placed theory at the beginning of this process. 13 However, neither theory nor intervention research frameworks such as this give guidance as to how to use theory to design interventions, nor how to use evaluations of behaviour change interventions to test theory. 14 Crucial to both exercises is to develop methods for mapping theory to techniques in this area. Increased specification of the links between theoretical constructs and change mechanisms, and behaviour change techniques will allow us to use theory more precisely in designing interventions and draw more precise theoretical conclusions from evaluations of intervention. We are beginning this work using consensus methods;8,15 however, there is a need for considerable methodological development in this area.
Behaviour change theory: conducting evidence syntheses
Systematic reviews of interventions to improve implementation seldom categorize interventions on the basis of relevant theory, and seldom produce a clear pattern of results. These two observations may be related. Our second focus was to develop methods for evidence syntheses of behaviour change interventions, based on description by component techniques and theoretically informed categorizations of interventions.
As an exemplar study, we are re-analysing a Cochrane review of audit and feedback interventions to change professional behaviour. 16 The original review categorized interventions into three levels of intensity. No rationale was provided for this categorization and there was no clear association between intervention intensity and behaviour change. We re-categorized the interventions and re-analysed the data on the basis of a relevant behaviour change theory, self-regulation theory. 17 The essence of this theory is that behaviour is goal-driven and people change their behaviour if they receive feedback that there is a discrepancy between their target and current behaviour, and they have strategies they can implement to reduce this discrepancy. Categorizing the interventions according to whether they included targets and/or action plans, in addition to feedback, gave a theoretically-based rather than ad hoc categorization. As predicted by this theoretical approach, we found an association between the number of theoretically-based intervention components and behaviour change.
We have also conducted a more fine-grained analysis of the intervention, documenting the variety of ways in which targets were set, feedback was given and action plans developed. In conjunction with relevant behaviour change theory and evidence, we developed a reliable method of coding 40 intervention characteristics predicted to influence outcome. This illustrates the potential complexity of such interventions, even in the case of an intervention, such as audit and feedback, that is considered relatively simple.
Since few interventions were reported in sufficient detail to code them accurately, we contacted authors of 59 papers for the full intervention protocols, obtaining additional material from only 18 of them. The main reasons for not providing material were that data were not kept or that archived data were too difficult to obtain. Since advancing science requires replication and building on previous research, advancing the science of behaviour change requires detailed descriptions of intervention content, mode of delivery, source, et cetera. 18 With the increase of electronic publishing and use of the World Wide Web, access to detailed intervention descriptions is improving rapidly. One welcome development is the adoption by scientific journals of policies to publish behaviour change intervention studies only if full intervention protocols are publicly available (for example, Implementation Science, Addiction and the International Journal of Behavioral Nutrition and Physical Activity).
Combining methods for reliably reporting interventions in terms of behaviour change techniques with methods for using behaviour change theory to categorize interventions has the potential to substantially improve methods for evidence synthesis. A small amount of additional behavioural science input into the systematic reviewing process is likely to lead to substantial increases in useful evidence.
Behaviour change theory: guideline development
There are well developed fields of study investigating methods of improving evidence synthesis and implementation; however, there is little study of how synthesized evidence is translated into guideline recommendations for practice. Thus, the crucial work of guideline development groups remains a black box.
Formulating evidence-based recommendations is a complex process, with many influences on communication and decision-making including methods of evidence presentation, perceptions of evidence and of the purposes of recommendations, practical/resource constraints, individual values, professional and scientific interests, social and psychological processes. As a first step to making this process more transparent and potentially effective, we need to understand these influences. Psychological theories of decision-making, social influence and shared representations are among those providing a framework for investigation.
We are conducting a longitudinal study of NICE guideline development groups, covering acute health care, public health and mental health by recording and transcribing all meetings of three groups and interviewing members at the beginning and towards the end of the process. 19 Using a critical incidents technique, data are selected for detailed analysis if they refer to evidence or recommendations, or reflect dilemmas, conflicts, uncertainty or turning points in the discussion. Data are analysed thematically and by content analysis, drawing on relevant psychological theories. The findings will potentially inform the further evolution of guideline development group methods, such as choice of members and procedures for presenting evidence, conducting discussion and formulating recommendations.
Behaviour change theory: implementing evidence-based practice
A range of implementation scientists advocate greater use of explicit theory in health services research, as it offers a generalizable framework, gives the possibility of understanding why interventions do, or do not, work, and facilitates the accumulation of knowledge. Despite this, theory is seldom used in implementation research. A theoretical framework for implementation research 20 is currently being used by several international research teams to design interventions to improve implementation (e.g. GP management of chronic back pain). We are currently validating this framework in relation to both implementation and population health behaviours to make the framework more useable for large-scale studies. Future research will develop the current theory-linked interview questions into a psychometrically robust questionnaire measure.
Key points and future directions
Improved population health needs more effective behaviour change interventions that, in turn, need more investment in developing the scientific methods for studying behaviour change. Immediate targets are to advance:
The selection and application of theories to designing behaviour change interventions;
The reporting of such interventions;
Methods for synthesizing evidence of behaviour change intervention effectiveness;
Conceptualization of the behaviours we are trying to change.
Since sustained behaviour change is likely to require interventions at different levels (e.g. individual, group, environment), there may be value in identifying theories of behaviour change from sociology, anthropology and organizational psychology. Their infrequent use in implementation research and population health sciences may reflect difficulties in operationalizing these theories or the theories may not be about behaviour change. An ongoing study is systematically searching a wide spectrum of literature, under the guidance of an expert group representing many disciplines, to identify relevant theories that are useable, or could be made useable. The resulting best theory or theories will be used to design and evaluate an implementation or public health intervention. This work will aim to elaborate the MRC framework for developing and evaluating complex interventions by demonstrating methods for applying theory to intervention development.
Many interventions are said to be theory-based, and considered to be more effective than those not explicitly based on theory. 21 However, we lack hard evidence and, indeed, a method for defining what evidence-based means. A reliable method for coding the extent to which interventions are theoretically based is currently being developed. Application of theory to the development and evaluation of interventions is indicated by a 17-item measure, with good inter-rater reliability for all items (kappa of at least 0.70). We are using this, in conjunction with our reliable taxonomy of behaviour change techniques, 11 to analyse a series of systematic reviews of behaviour change interventions. We are assessing the associations between the stated theoretical base of the intervention, degree of theoretical application, intervention content (techniques) and behavioural outcome.
In conclusion, this programme of research aims to sharpen the tools of behaviour change research. One such tool is defining behaviour change interventions and targeted behaviours with sufficient precision to allow replication and the possibility of accumulating evidence. A second tool is to develop links between intervention techniques and causal mechanisms. These tools are necessary if we are to build evidence about behaviour change theories from evaluating interventions and to apply theories to designing more effective interventions.
Footnotes
Acknowledgements
This work was carried out or written up during the first 18 months of a three-year secondment to the MRC HSRC. Additional research funding was awarded by MRC's Population Health Sciences Research Network, the National Institute for Health and Clinical Excellence, the Department of Health and Diabetes UK. I am immensely grateful to the HSRC's Director, Professor Paul Dieppe, for giving me this opportunity to do some innovative methodological research, for creating an intellectually stimulating and supportive environment at the HSRC and for providing an inspirational model of academic leadership.
My thanks also to enjoyable and productive collaborations with Marie Johnston, Charles Abraham, Jill Francis, Wendy Hardeman and Martin Eccles (Focus 1); Martin Eccles, Tess Moore, Tony Ades, Craig Whittington, John McAteer and Charles Abraham (Focus 2); Gene Feder, Paul Dieppe, Stephen Pilling, Rosalind Raine, Francoise Cluzeau, Phil Alderson and Simon Ellis (Focus 3); and Marie Johnston, Martin Eccles, Rebecca Lawton and Daniel Wight (Focus 4).
An earlier draft was improved by helpful comments from Marie Johnston and Robert West: thank you both.