
Abstract
Objective
To assess workforce and organizational issues in establishing a primary angioplasty service in England.
Methods
Staff associated with the heart attack pathway at seven acute hospitals participating in the National Infarct Angioplasty Project (NIAP) completed a questionnaire, participated in focus groups and interviews, and observations were undertaken in catheter laboratories.
Results
All seven hospitals implemented primary angioplasty though not all provided a 24-hour service. Hospitals varied in size, number of staff involved in the delivery of angioplasty and the volume of cases. Hospitals that developed the service by incremental expansion encountered more problems than hospitals that planned for a full service at the outset. Simple, direct access to a catheter laboratory reduced delays and could be facilitated by an angioplasty gatekeeper. Little attention was paid to later cardiac rehabilitation. Multiskilling and the ability to work across traditional professional boundaries appeared to provide substantial advantages. Building relationships with key staff and auditing the heart attack pathway were critical to successful service development. Differences in remuneration and rest for staff undertaking out-of-hours working threatened sustainability.
Conclusions
Primary angioplasty was feasible in varied settings and generally supported by staff. However, the participating hospitals were selected enthusiasts, only some implemented a 24-hour service and activity levels were relatively low. Organizational and workforce issues need to be addressed to achieve an efficient and sustainable service.
Introduction
Primary angioplasty is an effective 1 and cost-effective 2 treatment for acute ST-elevation myocardial infarction (STEMI), and has the potential to replace thrombolysis as standard treatment. Unlike thrombolysis, angioplasty is a complex intervention requiring the rapid assembly of an expert team with specialist facilities. This presents substantial challenges to deliver care in an efficient and sustainable manner. The clinical effectiveness and cost-effectiveness of primary angioplasty depend on minimizing treatment delay,2,3 so failure to address workforce and organizational issues could lead to ineffective treatment and a waste of health care resources. Previous studies looking at primary angioplasty have focused on clinical benefits and the availability of cardiologists and cardiac nurses.4–6 There has been no work examining the organizational implications of providing this type of service.
This study was located in England where primary angioplasty has not previously been the standard treatment of STEMI. From the late 1980s thrombolytic agents were administered by hospital staff to dissolve blood clots. Clinical trials demonstrated successful treatment was associated with timely restoration of coronary blood flow 3 and a programme of pre-hospital thrombolysis was instigated to deliver earlier administration of drugs by trained paramedics. A national service framework 7 set targets for drug delivery within 60 minutes from a call for help. Between 2001–2003 substantial investment of health resources was made equipping paramedical services. Further, improved provision of thrombolysis in emergency departments helped to reduce time delays. By 2002 several centres in England were investigating the use of primary angioplasty to deliver an emergency treatment of STEMI. In 2003, a review by the Prime Minister's Delivery Unit recommended the Department of Health develop a clear policy for expanding primary angioplasty.
The heart attack pathway sees a patient being bought to hospital by ambulance or self-presenting. The patient can pass through a number of departments for diagnosis and treatment. This is a time-bounded activity of some urgency. Provided there are no complications, a shorter hospital stay follows primary angioplasty than with thrombolysis. 2 The pathway for angioplasty is potentially complex, requiring detailed coordination and cooperation between primary and secondary care services for optimum care. Developing a primary angioplasty service was a radical change for participating hospitals. Most had operated an ‘office hours’ service for angioplasty with prebooked admissions for elective procedures and only occasional emergency work.
The National Infarct Angioplasty Project (NIAP) was established in 2005 to test the feasibility of providing a comprehensive primary angioplasty service at 10 hospitals in England, ranging from a tertiary provider to those that did not have cardiac surgery on site. 8 NIAP aimed to implement a 24-hour primary angioplasty service by 2006. We aimed to evaluate the implementation of these services by describing the processes involved, examining the workforce implications and effects of these provisions upon staff delivering primary angioplasty and related staff.
Methods
We used mixed methods to examine the heart attack pathway. Data collection aimed to: (a) describe implementation and feasibility issues of establishing the service; (b) assess facilitators and barriers to developing the service; (c) measure the effect of providing the service on the team and boundary relationships; and (d) identify the consequences to other services.
Resources permitted the study of only seven of the 10 hospitals included in the NIAP study. We selected seven hospitals that were sufficiently different from each other to represent a wide range of hospital environments: urban and rural, different geographic locations, single and multiple centres, and those that worked in partnership with other hospitals or as regional centres.
We examined the planned change in the organization of work 9 using a questionnaire, interviews, focus groups and observations involving the different staff groups along the heart attack pathway (Table 1). We tested these methods in one hospital over a four-day site visit in November 2006.
Methods of data collection

Prior to each hospital visit a research coordinator (usually a specialist nurse) was appointed and worked closely with the occupational psychologist managing the study. The coordinator was asked to identify the group of people who delivered primary angioplasty, to give the group a name, to describe the people who worked closely with and supported this group (such as the coronary care unit or emergency department) and to describe the out-of-hours team (the previous group being the in-hours team). If primary care staff were not mentioned then links with primary care were actively sought. Over a period of several weeks individual team members' names and job roles were identified aiming to gain an understanding of everyone who was involved in primary angioplasty either as part of the delivery group or who had boundary relations. Self-completion questionnaires were sent to those in the delivery group around the time of qualitative data collection so data were collected concurrently. Staff with boundary relations (such as specialists, research nurses, ambulance coordinators, service and bed managers) were invited to be interviewed.
Analysis of the pilot data revealed considerable overlap suggesting we could interview slightly fewer secondary care staff and instead interview staff on the primary care boundary, thus reducing each hospital visit to two days. Most of the staff involved in the trial visit were enthusiastic about primary angioplasty so at subsequent hospitals we actively sought views from those who were less positive by recruiting people to the study who we anticipated might have alternative views. The remaining hospitals were visited in quick succession to gain an accurate picture of the development of angioplasty, in June and August 2007. At one hospital it was not possible to conduct interviews and focus groups so staff only participated in the questionnaire survey. Hence, staff at a total of seven hospitals contributed questionnaire data and staff at six hospitals took part in interviews, focus groups and ethnographic observation.
At interview participants' comments were summarized and fed back to validate emerging themes. 10 We analysed qualitative data by constructing templates from research questions (thematic analysis 11 ) and deriving themes directly from the data in an inductive approach. Each hospital was considered a case study and for each we constructed a template. A second researcher conducted a comparison coding exercise (for inter-rater agreement); and agreed in approximately 90% of cases. In order to gain multiple perspectives three researchers (previously involved in data collection) undertook analyses, using the initial template as a broad guide. Once each template was produced comparisons were made of similarities and disparities in themes across the hospitals. The quantitative data were analysed using tests of difference and association and data on the number of primary angioplasty events that occurred in the month of study were collected.
Results
Participation
Two hundred and two staff from seven hospitals completed the questionnaires (66% were women, 47% had children living at home, 80% were born in Britain, 82% were white). Response rates varied from 25% in the largest team (n = 114) to 59% in one of the medium-sized teams (n = 59). One hundred and forty-four staff from six hospitals participated in the interviews or focus groups. All staff were actively involved in primary angioplasty or working on the boundary.
Qualitative data were obtained from interviews, focus groups and free-text contributions to the questionnaire survey. Comments were considered salient if they were reported by participants from more than one staff group; these are described as themes. Themes may be common to a particular hospital or agreed across a number of hospitals, either describing specific experiences of interest or common experiences of people undertaking primary angioplasty. Differences in the experience of working on primary angioplasty compared with other types of cardiology work from the questionnaire were examined along with qualitative themes from the interviews and focus groups. Bringing these aspects together we found that seven key themes emerged (Box 1).
Specific themes
The mode of implementation of primary angioplasty varied between sites;
Primary angioplasty required simple direct access for patients and good teamworking across professional boundaries;
Development of primary angioplasty may have been associated with knock-on effects upon elective services and particularly upon rehabilitation;
Building and maintaining relationships with key stakeholders was critical to service development and sustainability;
Regular audit of the heart attack pathway can identify blockages limiting the capacity of the system;
Staff needed to work in a flexible, multiskilled manner across traditional task boundaries;
Failure to harmonize staff pay and conditions before commencing the service meant inequity of reward and rest after out-of-hours working.
Implementation
All seven hospitals implemented primary angioplasty but the service provided varied. The number of people in the primary angioplasty delivery group varied from 37 to 114 staff and, with the exception of one hospital seeing 65 cases in the month of study, most hospitals saw less than 20 cases per month (Table 2). Three hospitals implemented a 24-hour service at the outset while four hospitals began on a smaller scale and grew their service. Staff from five of the six hospitals, with the benefit of hindsight, felt that it would have been better (or agreed it was better) to commence the service with 24-hour working rather than by slowly increasing the length of the working day. Incremental expansion led to a progressive burden being placed on staff, often without a clear strategy for a sustainable service being developed.
Characteristics of participating hospitals
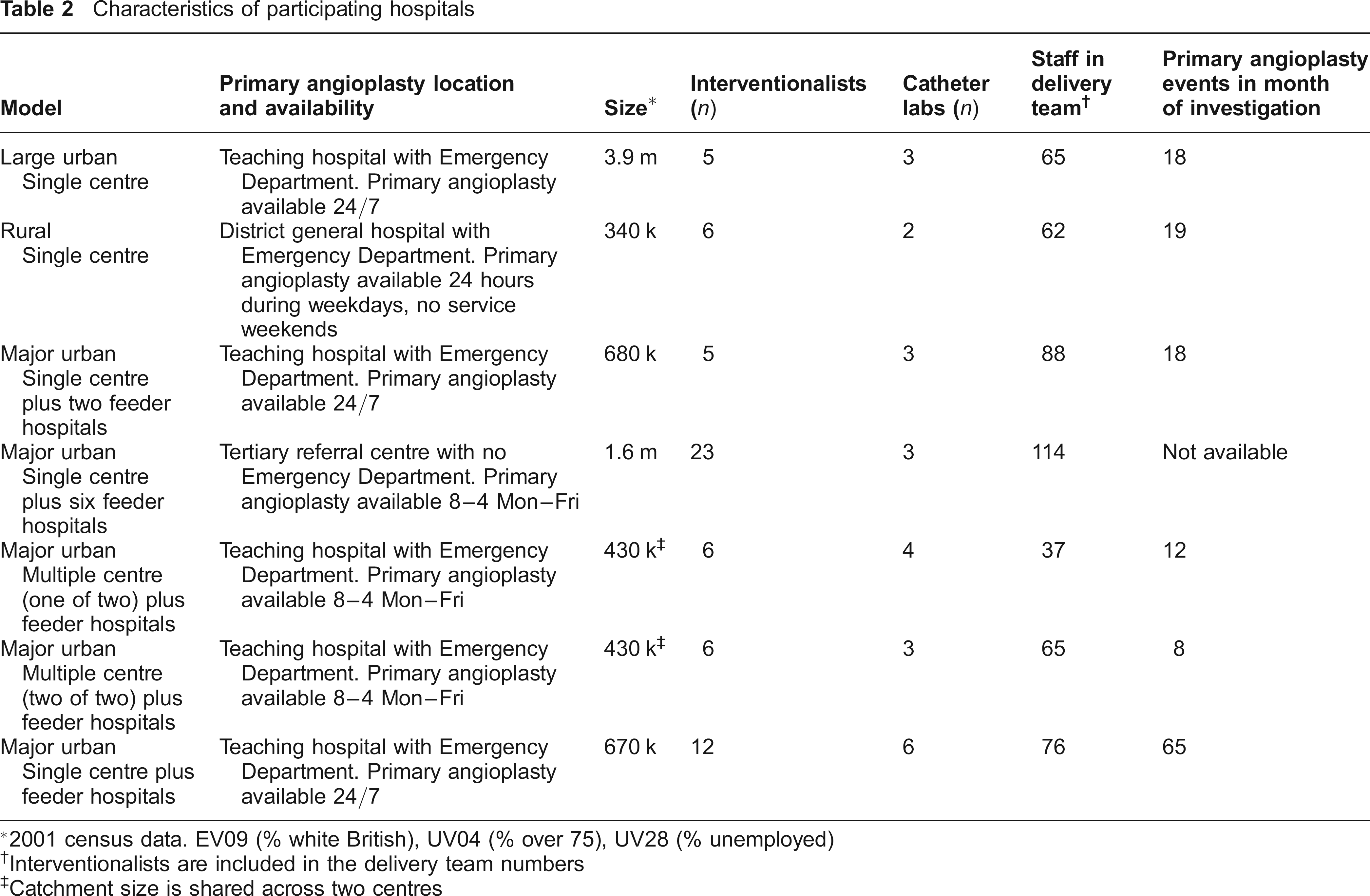
2001 census data. EV09 (% white British), UV04 (% over 75), UV28 (% unemployed)
Interventionalists are included in the delivery team numbers
Catchment size is shared across two centres
Staff voiced pride and ownership of the service. Staff from six of the seven hospitals completing the questionnaire expressed job satisfaction of doing work that makes people better and saving lives as the most important rewards from their work. However, the challenge was working with acutely ill and unstable patients some of whom may die despite the best efforts of those involved (see Box 2 for other areas of satisfaction and challenge associated with primary angioplasty). Staff also reported, on average, slightly higher levels of enthusiasm when working on primary angioplasty cases (mean = 3.93) compared to other cardiological work (mean = 3.83; P < 0.02). However, a cardiology registrar noted that ‘keeping up the enthusiasm gets difficult after a while’. Staff at all hospitals described difficulties expanding the service over a 24-hour period (such as maintaining adequate staffing in the multidisciplinary team, working with inexperienced staff or those unable or unwilling to multitask, and slowing work in catheter laboratories at critical moments).
Satisfaction and challenges of undertaking primary angioplasty
The survey asked staff what they enjoyed about primary angioplasty work:
Intrinsic job satisfaction of doing work that makes people better and saving lives were the most important rewards from their work (a common theme from staff of six out of the seven hospitals surveyed 6/7);
Working as part of a strong, competent team (6/7);
Challenge, excitement and unpredictability of the work (4/7);
Opportunity to develop new skills (4/7).
The challenges of primary angioplasty work:
Working with unstable patients (such as the need to use multiple drugs and treatments with acutely ill patients, the stress of working with very ill patients and people dying despite best efforts of staff 6/7);
Trying to maintain achievements while consistently achieving high standards of care with minimal disruption to other services (2/7);
Difficulties in coordinating resources after out-of-hours working and elective patients being delayed by emergencies (1/7);
Difficulties maintaining work–life balance after long hours of work and inadequate rest after on-call while still being able to maintain their concentration at work the next day (1/7);
Inequalities of pay and conditions of service across the out-of-hours teams (1/7).
Staff at all hospitals emphasized the need for effective management of the service. Staff described several problems related to being managed in a fair and equitable manner (such as frequent undesirable shifts and inadequate rest periods after out-of-hours working). While several departments had a catheter laboratory manager (or coordinator) this was usually a senior nurse with either catheter laboratory or other specialist responsibilities who found it difficult to find time for managerial activities. Only one hospital had a dedicated manager whose role was to manage and coordinate medical and non-medical staff and to balance the elective and emergency schedules.
Simple direct access and good teamworking across boundaries
The experience of staff from four of the six hospitals led them to report that the best entry to the system is a simple pathway going straight from the ambulance to the catheter laboratory avoiding the emergency department. Even with a single pathway, managing the admission process required not only good teamwork in the cardiology unit but excellent cross-boundary working with ambulance personnel (ensuring an adequate history is taken and electrocardiograph transmitted) and other staff (such as anaesthetists who may not understand the time urgency of their attendance in catheter laboratory if called to provide assistance). Entrance to the pathway could be better managed through a gatekeeper (mentioned by staff from five of the six hospitals). A gatekeeper system was operating in three hospitals, the gatekeeper being a senior cardiology nurse or doctor. Gatekeeper roles varied depending on the location of the ambulance entrance and the catheter laboratory. Roles included: liaison with ambulance personnel about the electrocardiograph; coordination with cardiologists about the diagnosis; and meeting the ambulance, clerking and preparing the patient as they were being transferred to the department. Hospitals operating a gatekeeper role both in-hours and out-of-hours managed the system more effectively.
Knock-on effects to elective working and rehabilitation
Staff at four of the six hospitals described incidences of emergency patients disrupting outpatient clinics and delaying elective cases. This was either because of the arrival of an emergency or a knock-on effect of out-of-hours working reducing staff available for next day working (particularly noticeable with cardiology technicians who undertake a variety of roles in catheter laboratories and clinics).
Relationships with staff in cardiology were well developed and described by staff in four of the six hospitals. However, relationships with staff in the more distal parts of the pathway such as those involved in rehabilitation after discharge from hospital were less well developed (only mentioned by staff in one of the six hospitals). Difficulties providing rehabilitation were described by staff at all hospitals visited (often due to the rapid discharge of patients and limited resources) along with accessing community rehabilitation. Staff noted that limited post-procedural information reached primary care (mentioned by staff at two of the six hospitals). Exit from the acute pathway was often delayed (waiting for drugs or future appointments) limiting the capacity for further emergencies (described by staff from two of the six hospitals). An innovative response to this problem from these two hospitals was to develop acardiac pharmacy post to dispense drugs from the cardiac ward.
Building and maintaining effective relationships along the heart attack pathway
Staff at all hospitals stressed a crucial element to managing development of primary angioplasty was to encourage those involved that change was not unusual but a normal part of service development. Further, staff at all hospitals described taking time to appreciate others' perspectives was helpful in getting people to work together. The value of listening to the experiences of various staff at different points in the pathway and examining how the emergency situation affected the work in different departments was emphasized by staff at all hospitals. In addition, staff at three hospitals described the value of having an internal champion promoting the case for primary angioplasty with senior managers. Developing relationships with the ambulance service, other hospitals not providing angioplasty, general practitioners and service development forums were frequently mentioned but it was less usual to describe building relationships with senior management of the trust (only described by staff at two of the six hospitals). Indeed, these staff criticized the lack of support offered by their managers to develop the service, citing long decisionmaking processes and competition for resources as barriers to service development.
Regular Audit to Identify Blockages in the System
Staff at five hospitals described instigating processes to review and develop the service while acknowledging threats to service development (Box 3). Multidisciplinary groups met on a weekly or fortnightly basis during the NIAP period to identify solutions. Most of these meetings ceased at the end of the NIAP.
Examples of processes audited
Quality and speed of service (staff from two of the six hospitals who contributed to interviews and focus groups described this theme 2/6);
Time of day STEMI patients present (1/6);
Patient and carer experience (4/6);
Changes in the big picture of cardiac care (2/6);
Efficiency of transfers to district general hospitals (1/6).
Work roles
On average, staff spent 22% of their time (with only 15% spending more than half their time) on primary angioplasty. Those who see primary angioplasty as their main work reported, on average, higher levels of role clarity, receiving more feedback on work performance and slightly higher levels of anxiety when doing primary angioplasty (anxiety–contentment was lower; mean = 3.63) compared to doing other cardiology work (mean = 3.89). However, the enthusiasm of all staff was significantly higher when working on primary angioplasty (mean =3.93) than on other work (3.83, P < 0.02).
Staff reported that the key to successful development of primary angioplasty was an experienced team, whose members were flexible and able to multitask (blurring the boundaries between communicating with the patient, giving drugs and monitoring the patient). However, this way of working was not for everyone; some staff (in varying roles) did not want to take on others' roles because they felt this was not the job they had trained for or that it constituted extra work.
Inequity of reward and rest after out-of-hours working
Staff at five of the six hospitals described poor working conditions. For some this was the heavy nature of catheter laboratory work (wearing lead aprons, maintaining a high degree of concentration); for others the intense nature of the work. Work became difficult with more patients, more frequent out-of-hours working and inadequate rest. Differences in on-call pay and conditions between the staff groups became more salient with increased activity. For example, non-medical staff at some hospitals described difficulty parking and gaining entry to the hospital at night, a problem that medical staff did not face. Staff were prepared to tolerate these differences when setting up the service but once the frequency of primary angioplasty increased the lack of harmonization of pay and conditions become an issue. The survey confirmed that on average working on primary angioplasty will have a significantly greater impact on home life (t = 2.00, n = 168, P < 0.05) than when doing other work, but only for those who do a substantial amount of primary angioplasty work. This negative impact is especially likely to occur for people who have children or a dependent at home, regardless of their sex.
Staff at four of the seven hospitals stated that the service was running on their good will and that it was not sustainable. Examples of breaches of good will were repeatedly being asked to work extra hours without pay and frequently having shorter rest periods after out-of-hours working to maintain adequate service delivery the following day.
Discussion
Primary angioplasty can be implemented in the NHS. As a consequence the Department of Health in England is promoting development of a national primary angioplasty service. However, some of the hospitals participating in the NIAP were operating at relatively low activity levels and had not achieved a 24-hour service. As activity increased workforce and organizational considerations become more salient and these may present significant barriers to development. We identified four areas as central to the successful development of this service.
Plan for a 24-hour service at the outset
Establishing the 24-hour primary angioplasty service from the start appeared to work better than incremental expansion. While primary angioplasty was in an experimental phase with only a few cases per month, few difficulties were seen. However, problems emerged as the number of emergency patients increased. The ‘big bang’ approach fundamentally changed the way people worked rather than incrementally developing the new service on existing ways of working. Staff appeared to be more willing to take on new roles in these circumstances, particularly if there was a dedicated role to manage the resource.
The literature 9 supports the importance of acknowledging new ways of working as completely different work roles. In particular, staff described the need to set up new contracts of work with different expectations of working hours at the introduction of primary angioplasty. In this way the new way of working would then not violate previous norms and ‘extra hours’ of work would be considered the norm and appropriately rewarded.
Key to the effective delivery of primary angioplasty is the ability to maintain access to a catheter laboratory over a 24-hour period, 365 days a year. The challenge is to be able to accommodate additional, unplanned cases without adverse impact on the elective workload without displacement or cancellation of such cases. Displacement of planned work is distressing for both staff and patients alike and may undermine the quality of care. It is important that trusts and policy-makers appreciate the scale of investment required to deliver such a service.
Have a simple pathway direct to catheter laboratory facilitated by a gatekeeper
A simple, direct pathway is the preferred service model delivering the patient to a catheter laboratory with the minimum of delay. Having a gatekeeper working throughout the 24-hour period could reduce the risk of false alarms activating the system inappropriately. In addition, the gatekeeper becomes the recognizable outward-facing role of the catheter laboratory and able to ease the emergency patient through potential hold-ups. We recommend policy-makers and trusts implement gatekeepers both in and out-of-hours.
Build and maintain relationships along the pathway and monitor efficiency
Building and maintaining relationships with staff along the heart attack pathway and conducting regular audits are critical to service development and sustainability. Engaging senior managers and having a visible champion of primary angioplasty can be valuable in the development of the service. Auditing exits from the acute pathway should enable more new emergency patients to enter the system. Moreover, reflection encourages an understanding of the bigger picture of cardiac care that extends across primary and secondary care. The distal end of the heart attack pathway (rehabilitation and communication with general practitioners) would appear to be the most neglected part of this service.
Staff were aware of the benefits of understanding others' perspectives of service provision and working together to develop an effective heart attack pathway. They gain others' perspectives in conversations and multidisciplinary staff meetings which gave them opportunity to reflect on the issues that occur when an emergency patient enters the system. However, most of these activities stopped once NIAP support ended. These strategies are essential both in the start-up phases and to enable the system to be sustained. We recommend policy-makers include these activities in their guidelines 8 and hospitals implementing primary angioplasty fund their operation.
Harmonize staff pay and conditions across the out-of-hours team at the outset
Doctors, nurses, technicians and radiographers in the angioplasty delivery team are rewarded differently for their work. Initially, differences in pay appear to be tolerated, but as the frequency of out-of-hours working increases such differences for on-call working and variation in the amount of statutory rest become more salient and may adversely affect staff motivation. Some harmonization of pay and conditions is necessary, particularly for non-medical staff undertaking on-call working, for effective teamworking to be sustained in the longer term. Again we recommend policy-makers and those implementing new primary angioplasty services to consider issues of differences in pay, rest and access to resources.
Strengths and limitations of the study
There are several limitations to this study, most notably that of a small sample who volunteered to be involved and may not be representative. The selection process for the NIAP study involved hospitals putting themselves forward and demonstrating that they would be capable of pioneering the service. It is therefore likely that the participating centres were at least led, if not staffed, by enthusiasts and those who were keen to embrace change. However, active steps were taken in the evaluation study to hear less enthusiastic voices and a number of limitations have been identified.
At the time of study there were less than 10 hospitals providing a comprehensive primary angioplasty service in England, and of those a majority took part in this study. That the study included such a limited number of sites does not cast doubt upon the validity of the findings of our research, but it would be reasonable to speculate that less enthusiastic sites might identify other or more severe barriers to operation.
Conclusions
Failure to address workforce and organizational issues could result in failure to develop effective and cost-effective primary angioplasty, and be detrimental to other cardiac services. The effectiveness of primary angioplasty depends upon reducing time delay to treatment to a minimum. Failure to maintain efficient working practices will increase delays and reduce effectiveness. If staff concerns regarding onerous duties, poor out-of-hours rewards and lack of sustainability of the service are not addressed then this could lead to staff being lost to other parts of the health service or a general deterioration in the care provided in angioplasty centres.
Footnotes
Acknowledgements
We thank the NIAP Steering Committee, participating hospitals and the research participants for their time and honesty and participating organizations for their support and cooperation in this project.