
Abstract
Objectives
To assess the environment of an emergency department (ED) and its impact on care of adults aged 75 and over, using a ‘senior-friendly’ conceptual framework that included the physical environment, social climate, hospital policies and procedures, and wider health care system.
Methods
In this focused ethnography, we collected and analysed data from the ED of a regional acute care hospital located in Ontario, Canada from October 2007 to January 2008. Data collection included interviews with seniors or their proxy decision-makers, staff and key community informants; on-site observations; a staff survey; and hospital administrative data. Data sets were individually analysed and a synthesis of findings developed to formulate recommendations for policy, practice and education.
Results
Staff expressed their vision of providing senior-friendly care. However, the ED was fast-paced, overcrowded, chaotic and lacked orientation and wayfinding cues, as well as appropriate equipment and furniture, all of which created barriers to providing appropriate care. Seniors' expectations often went unmet and staff expressed moral angst at recognizing unmet needs. Some hospital policies and procedures compounded these difficulties, including hallway practice, lack of off-hour access to multidisciplinary health care professionals, and the inability of patients to access food and drink. Better communication and coordination between the ED and other components of the health care system are needed.
Conclusions
The ED is an important part of seniors' health care. Changes to policy and practices, and enhanced education must occur to better meet the complex health care needs of seniors. This assessment provides a method that can be replicated elsewhere to generate site-specific recommendations and initiate capacity development processes to enhance senior-friendly care.
Introduction
In many countries, seniors represent a growing proportion of the population and their use of acute care services is expected to rise. An emergency department (ED) is a gateway to acute care services, yet little research exists on ED care provided to seniors. 1 Seniors are triaged in EDs at levels requiring significant acute care intervention.2–4 The literature also points to concerns about the negative impact that ED environments have on seniors' physical and mental health,3,5,6 the frequency of preventable adverse events that occur in hospitals, 7 extended bed wait times in EDs for seniors, 8 and need for policy changes. 9 Furthermore, data on alternative level of care (ALC) patients, i.e. those occupying an acute care hospital bed without requiring that intensity of resources/services, indicate they are an older-aged group with more co-morbid conditions, likely to enter hospital through ED services. In Canada, 2007–2008 data indicate that 27% of ALC patients in the province of Ontario discharged home revisited the ED within 30 days. 10
A ‘senior-friendly’ hospital is a relatively new concept and features of such a hospital are variously described.5,11,12 Essentially, there are four interactive dimensions: the physical environment; social climate; hospital policies and procedures; and health care system issues (see Table 1).
Core dimensions of senior-friendly hospitals 18
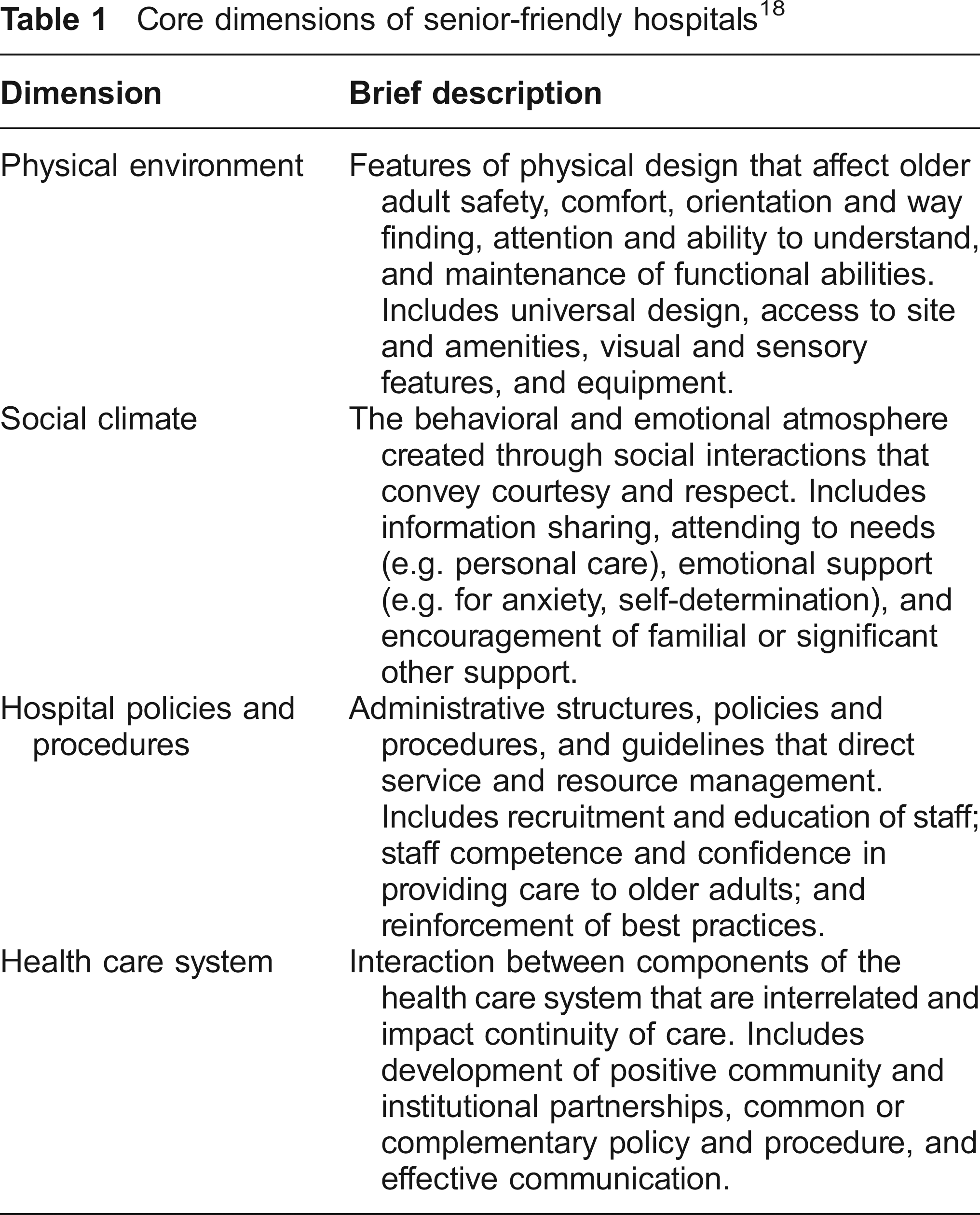
Together these core elements affect the vulnerabilities of seniors. 13 Provision of ‘senior-friendly’ acute care has implications for patient safety and, potentially, affects staff's ability to reduce adverse outcomes associated with hospitalization of older people. 6
The purpose of this study was to assess the environment and care provided to adults aged 75 and over in the ED of a regional acute care hospital. The aim was to identify gaps between current practices and known ‘senior–friendly’ practices to formulate recommendations for policy, clinical practice and education based on evidence. The research question was: how do the physical environment, social climate, hospital policies and procedures, and health care system promote or impede the capacity of the hospital to provide ‘senior-friendly’ care in the ED? The study was conducted in partnership with the hospital administration that recognized its importance for achieving their goals of patient-centered care and patient safety while maximizing the effectiveness and efficiency of resource use in the ED.
Method
Study design
Focused ethnography was used to explore and understand the physical environment, social climate, policies and procedures, and health care system influences on ED operations in the provision of care to adults aged 75 and over. This method involves intensive data collection in a compressed time frame using multiple methods to capture complex dynamics.14,15 Ethical approvals were received from the university Research Ethics Board and the Research Ethics Board of the hospital.
Location
The study site was the ED of a regional acute care hospital in Ontario, Canada. The census metropolitan area served had a population of 122,907; median age 41.8 years and population density 48.2 per square kilo-meter. 16 The hospital had 375 beds and established partnerships with regional health care providers. In 2007, 95,000 visits were made by people of all ages to this ED and it is ranked one of the busiest EDs in the country. 17
Data collection
Seven data sets were generated for analysis (see Table 2). Hospital administrative data were routinely collected by the hospital. On-site data collection (interviews and observations) took place for four hours daily over a three week period; week one, 0900–1300; week two, 1300–1700; and week three, 1700–2100. These hours were chosen in consultation with ED staff to maximize data collection opportunities and simulate a full week. Although night hours were not included, overnight experiences of seniors and staff were captured during interviews. Interviews followed a semi-structured guide and were audio-taped with participant permission. Seniors aged 75 and over or their proxy decision-makers presenting at the ED were invited to participate in on-site interviews. Proxies were approached as an alternative when ED staff judged a senior's health status or cognitive capacity impeded participation. All participation was voluntary and consent forms signed by participants. Those who consented to follow up also had post-discharge telephone interviews. Code Plus 18 was used to examine the physical features of the ED. Researchers' observations in the ED were generated using a guide based on the dimensions of senior-friendly hospitals developed from previous research (see Table 1). 19 The staff survey provided supplementary data to staff interviews and an alternative method to maximize staff participation. It gathered staff perspectives on strengths, barriers and vision for change in the provision of care to seniors.
Seven sources of data in the Emergency Department (ED)

Data analysis
Hospital administrative data underwent descriptive and inferential statistical analysis. The standards of coding and a systematic process of analytic induction 20 were applied to qualitative data sets (i.e. interviews, observations, survey). Each data set was analysed independently by a member of the research team. Preliminary results of the analyses were presented by that researcher to the team and the research assistants who collected the data. Interpretations and conclusions were discussed, defended with raw data, and consensus achieved on all conclusions. Two sub-reports were developed related to the physical features and administrative data. All findings were then integrated and a synthesis developed to identify gaps between current practices and known best practices in ‘senior-friendly’ care, with corresponding recommendations for quality improvement.
Results
Seniors' utilization of the ED
In 2007, 11% of the total visits to this ED were made by seniors aged 75 and over; 5,019 seniors made 10,412 visits to the ED. The seniors' median age was 82 years. Almost 60% were female, 95% local residents, and 90% had a family physician. The seniors' living arrangements were predominately with family (45%) or unpaid non-family (44%). The analysis also indicated that:
70% of seniors visited the ED four times or less and 25% made one visit. 30% (1,500 people) of seniors visited more than four times. 32% of seniors arrived by ambulance.
Eighty-five per cent of visits by seniors were assigned emergency or urgent triage levels, with 12% of visits less urgent as determined by the Canadian Emergency Department Triage and Acuity Scale (C-TAS). 21
Staff Survey–vision for seniors' care
Staff perceived that they provided compassionate care within limits imposed by the environment: low staffing levels; the high complexity of care required; and lack of skill and knowledge in geriatric care. Their vision for the ED encompassed an ability to provide for seniors' privacy, comfort, and quality patient-centred care. Family presence would be encouraged and accommodated. Policies and procedures would facilitate ease of access and timely attention to the physical, emotional and social needs of seniors.
Physical environment
The physical space of the ED was problematic and participants noted overcrowding, noise and limited space. Problems consistently revolved around promoting safe and independent function, and having appropriate equipment and furniture for comfort and ease of work. Orientation and wayfinding cues, and access to the ED (e.g. parking, bus stop) and amenities (e.g. bathrooms, walk-ways and distance to other areas) presented challenges. Staff, seniors, seniors' proxies and community informants all described troublesome aspects of the physical environment. For example, ‘… a senior with a walking impairment or mobility problem, they're having problems in there trying to get around' (Community Informant). Seniors specifically spoke about being cold, hungry, thirsty and experiencing noise, lack of privacy and interrupted sleep; ‘[staff] took me out of the cubicle and stuck me out in the hall and had me and everybody else using the same washroom'’ (Senior). These problems for seniors were affirmed in comments made by ED staff and the seniors' proxies. For example, ‘… she didn't get fed. If I wasn't there I think she would have been pretty hungry' (Senior's proxy).
Social climate
Participants described the ED as ‘busy’ and ‘chaotic’. Seniors reported coming to the ED because they believed their needs would be met quickly. Some were fearful and sought reassurance. Seniors' expectations, however, were inconsistently met. A bad visit was described as ‘being moved around a lot’ and as a lack of one or more of: physical comfort; emotional attention; information; or family reassurance. In contrast, a good experience was exemplified as being pain free, having questions answered, being reassured, being able to sleep, having food and drink, and family satisfaction.
Staff and community informants recognized that work with seniors takes more time; seniors present with complex medical conditions. They also indicated that seniors' needs may be unmet, dependent on how busy the ED was at any given time. These unmet needs included physical needs such as nutrition, hydration, toileting, mobility, sensory and medication as well as social-emotional needs including privacy, mental health, and explanations of treatment or other hospital processes. An unaccompanied senior presented particular challenges such as: difficulties confirming needs; history; medications; and or providing assistance, especially if cognitively impaired or extremely frail. ‘When I go into the ED with the senior, usually I find that they receive faster care, and faster results, everything is done a lot quicker&; when they're with somebody' (Community Informant). Staff also perceived family involvement can be critical to a successful visit to the ED.
Many staff also acknowledged the fundamental role performed by support workers in meeting seniors' needs (e.g. toileting, dressing, feeding) although these staff were responsible for many other duties (e.g. restocking supplies, assisting with critical care). Furthermore, moral angst was expressed by staff. Many spoke about the need to improve care and some felt distressed when they were unable to respond to recognized care needs. ‘You hear an elderly person, you tend to walk by a lot… hear some elderly patients call out “help, help, help” [they're] scared. End up conditioning yourself, get so used to hearing it' (Staff).
Staff expressed views such as, ‘Every step along the way, you see where elders lose and lose and lose’. However, seniors expressed acceptance and understanding of the busy chaotic atmosphere and appreciated the assistance they received. One senior explained it this way, ‘Sometimes you have to wait because they are busy, but it's not like they don't care, they are trying but they are so busy' (Senior). All agreed that if help was needed quickly it was received; ‘they take you right away, no sitting around when you say you have heart problems’ (Senior) or ‘when you can't breathe' (Senior).
The need for enhanced communication was both expressed by participants and observed by the researchers. Staff name tags were often not legible and clothing did not distinguish between roles and responsibilities, making it difficult to know who to ask for help. A need to use plain language and to take more time to ensure understanding of process and the care plan by seniors and families was also acknowledged. ‘I'm not sure we explain properly to patients. “You have to wait for the next set of enzymes.” If you're 87, what does that mean?' (Staff). Communication issues sometimes affected discharge. Plans were not always understood by seniors and/or communicated with family and others (e.g. community services).
Hospital policies and procedures
All participants viewed the ED as ‘under-staffed’ and staff as ‘overworked’. Staff expressed concerns about the care of seniors; ‘We're scrambling right now. We don't see them [seniors] as a special population… with special needs' (Staff). Seniors expressed reluctance to use ED services even when they were encouraged by others to visit.
In the ED, patients were often placed in hallways to await tests, treatment or admission and this was referred to by all participants negatively. ‘I had to wait five hours in the hallway, that doesn't help. Then finally… they gave me extra Tylenol for the pain' (Senior). Patients in hallways also compounded congestion and impeded traffic flow in the ED. Difficulties accessing and ensuring adequate nutrition and hydration during wait times included time delays between meal requests and delivery to the ED (staff are busy and forget); food trays sitting in ED before delivery to the patient (food safety issue); food unsuitable for complex needs (e.g. swallowing problems); difficulty managing plastic cutlery and paper cups; and lack of assistance to help with eating. Staff also noted access to other health professionals such as discharge planners and social workers was limited to day shifts, Monday to Friday, with a need for access beyond these hours.
The need for education and training on a wide range of topics was noted by staff. Topics included common health problems associated with ageing, communication with seniors and families, community services, elder abuse, and cultural and ethnic-sensitive care practices. Many staff also identified difficulty in providing ED care to seniors with dementia and responding to symptoms such as confusion, agitation and aggression. Both staff and community informants identified a need to educate seniors and their families on topics such as hospital and community services, and advance care directives.
Health care system
A number of system problems outside the realm of the ED negatively affected services and their ability to meet the needs of seniors. Some staff perceived that seniors visit the ED as a way to access community or home care services because of problems accessing such services. Staff and community informants also identified communication problems between health care professionals when a senior moved between services. ‘What happened, did they have an X-ray, were they put on new medications&; It's also on our end too, are we sending adequate information that they're able to care for the resident, are we sending too much that they don't have time to review it?' (Community Informant).
Some staff wondered about the appropriateness of nursing home referrals and whether or not the presenting problem could be dealt without transfer to the ED. On the other hand, a few staff indicated that nursing homes occasionally wait too long before sending a senior (e.g. ‘on death's door') and an earlier arrival at the ED would be preferable. It was also evident that, overall, staff were unfamiliar with community and other specialized geriatric services. This unfamiliarity with various services, their mandate, availability, and contact information had an impact on staff time required to make plans and appropriate referrals.
Discussion
Recommendations and the way forward
A series of site-specific recommendations for quality improvement were made based on the findings of the study, organized in terms of physical environment, social climate, hospital policies and procedure, and health care system. These were presented to the hospital management committee, ED staff and leadership team, and community health services that interact with the ED. Table 3 illustrates a sample of the recommendations.
Examples of site-specific recommendations
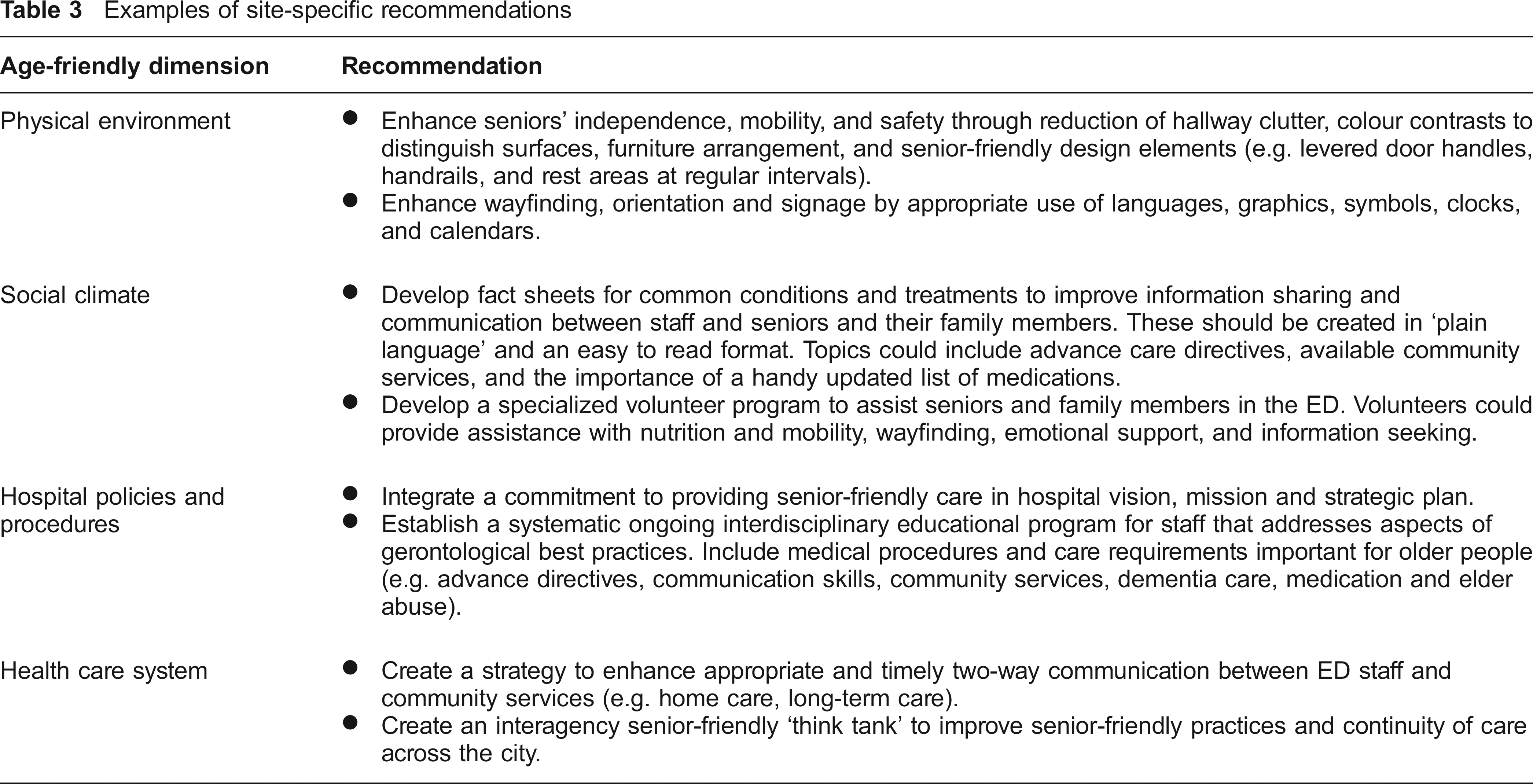
Some recommendations could be expected to have an immediate impact on service delivery such as incorporating way-finding cues and other changes to the physical environment. Other recommendations addressed longer term organizational strategies to begin a systematic approach to the realignment of resources, introduction of new care protocols, staff education, and creation of strategic linkages within the health care community. Longer term strategies included examining the possibility of developing a specialized program and dedicated space for seniors with non-emergency care needs.
In moving forward, a comprehensive community capacity development approach was also recommended to guide and evaluate a multi-year strategy to provide the highest quality patient-centered care to seniors. Central to this approach is building on existing knowledge, skills and relationships among staff in a way that fully engages them to work towards a vision to which they are committed, without imposing change from outside the ED. 22
The recommendations are made in the spirit of building on hospital strengths to further develop capacity for senior-friendly care in the ED. Staff had expressed a desire to offer senior-friendly care and many possessed knowledge, values and skills consistent with such approaches. As potential leaders and role models, they are a tremendous resource to draw upon to build stronger collaborative relationships amongst staff, provide sufficient and appropriate human resources and equipment, and nurture a sense of empowerment through strong management support and organizational commitment. Linking the initiative to the hospital's strategic plan with accountability for progress the responsibility of the senior management team and the Board would strengthen the change process.
Study limitations
Gathering data from very busy staff and very sick patients in an ED is extremely challenging. On-site interviews generally lacked privacy, which may have influenced interviewees' comments. However, the diversity of participants and variety of methods of data collection allowed for triangulation of findings and provide confidence that the story was fully told. While the study inclusion criterion was all seniors aged 75 and over, a limitation was that not everyone identified as a potential participant was interviewed. Some individuals declined participation and, as required by the Research Ethics Board, some seniors were not approached if nursing staff judged them incapable (i.e. gravely ill or cognitively impaired) and, therefore, their direct experience was not captured. Seniors' proxies were approached for an interview if the senior was deemed incapable; however, it cannot be assumed that proxies accurately represent patient experience. People with cognitive impairment also represent a special population because of consent issues and approaches to data collection. Future studies are needed to explore the ED experience of this group. While there is a possibility of systematic bias in the sample towards those who may have had a positive ED experience or fewer concerns as a result of screening participants by nursing staff, the negative opinions expressed by many patients and proxies suggests otherwise. Finally, the study was of a single ED, so care should be taken in generalizing the quality of the environment for seniors to all EDs in Ontario or beyond. However, the views and experiences reported resonate with much that is known about ED care elsewhere.
Conclusion
We examined an ED environment as it relates to care provided to seniors aged 75 and over, and found it to be fast-paced and chaotic, making effective communication, timely attention to seniors' physical, social and emotional needs, meaningful family involvement, and teamwork an overwhelming challenge. The findings concur with much of the literature that points to the challenges facing ED services in provision of care to seniors.1,3,23–28 As a group, seniors appear to access ED services appropriately, present with more complex physical and social needs, and take more staff time and ED resources to manage. While adverse consequences for seniors (e.g. increased risk of harm, delays in care, compromised privacy and confidentiality) occur with frequent overcrowding and delays in EDs, 29 the current study also identifies the moral angst of staff specifically related to the quality of care they provide to seniors. 1
The study makes a distinctive contribution to research on ED care of seniors since it examined perspectives held by seniors and their proxy decision-makers as they experienced an ED, including their post-discharge reflections, and included the views of multidisciplinary staff and community informants from related services. The four core dimensions associated with senior-friendly hospitals were found to be useful to identify targets for change that could improve care and to generate site-specific recommendations. This study provides a comprehensive, senior-friendly, conceptual framework and method to assess the environment of other EDs and, indeed, other hospital departments (e.g. diagnostics).
Senior-friendly ED care has potential to improve clinical care, patient and family satisfaction, increase job satisfaction for staff, reduce costs and inappropriate use of resources, and enhance accreditation processes. 5 The impact of providing senior-friendly ED care on outcomes for seniors, staff and hospitals, however, needs to be evaluated. Economic analyses are also needed to examine the implications for health care costs. Knowledge generated through this and future research associated with senior-friendly acute care will contribute to evidence needed by health care systems and organizations to meet the call for a global mandate to become ‘elder essential’. 30
Footnotes
Acknowledgements
Our special thanks to the seniors, their families and hospital staff who participated or otherwise supported this project. The full report of the emergency department environmental scan is available from the authors.