
Abstract
Objective:
Although over half a million migrants arrive in England each year, information about their use of health services is limited. Our aim was to describe the use of secondary care by international immigrants and compare it to people moving within England.
Methods:
Routine anonymized data were used to identify people who appear as registering with a general practitioner (GP) for the first time in England, yet are aged 15 or over. We assumed that most long-term residents will have registered before the age of 15, and therefore the majority of those registering for the first time later in life will be international immigrants. The study compared hospital admissions among first registrants to the general population of England and to within-England migrants, selected using propensity scoring.
Results:
The first registrants aged 15 or over had around half the rate of hospital admission asthat of the general population of England. They were also less likely to have a hospital admission than a matched group of within-England migrants. The lower admission rates persisted over several years and were consistent in three consecutive cohorts of first registrants (each consisting of over half a million people).
Conclusions:
The assumption that international immigrants use more secondary care than the members of the indigenous population appears to be unfounded.
Introduction
Over half a million international immigrants arrive in the UK each year. International migration is expected to be responsible for almost 70% of population growth (7.3 million people) between now and 2031. 1 The National Health Service (NHS) in the UK is free at the point of care to people who are ‘ordinarily resident’ in the UK. 2 International migrants are entitled to all publicly-funded health care once they become ordinarily resident, and to necessary treatment in an accident and emergency department for certain infectious diseases from the moment they arrive. In addition, the UK has bilateral health-care agreements with some countries. Understanding and catering for the healthcare needs of migrant populations is therefore essential for planning health services.
Although the impact of migration on public services has become a contentious issue in public and political debate, 3 very little information is available about migrants’ use of health services and, in particular, the costly elements of secondary care, especially across the whole population of migrants as opposed to specific sub-groups.4,5 The use of health services by ethnic minorities is better understood 6 but fewer than half of people belonging to an ethnic minority in the UK are migrants.
Studies tend to find that migrant groups have lower mortality than their host populations, despite their lower socioeconomic status. 7 How this translates into health service use is not clear, particularly given reports of high demand for maternity care among migrants. 8 Further, lower mortality is not common to all migrant groups9,10 and aspects of health can begin to deteriorate soon after arrival.11,12 Overall, the relationship between migration and health is complex, with migrants self-selecting on health status, and health being influenced by the process of migration and conditions in the host country as well as the country of origin. Studies are increasingly using longitudinal data sets to understand its dynamic nature. 13 Our aim was to explore a new strategy for measuring international immigrants’ use of secondary care.
Methods
Patient registration data were obtained from the National Strategic Tracing Service (NSTS). The data base contained 131 million records of patient registrations with general practices in England and Wales from January 2000 to October 2008. From these, about 550,000 records per year were selected for people registering with a general practice in England aged 15 or over with no previous registration history.
It was assumed that most English-born people will have registered with a general practice before the age of 15 and that the majority of those registering later than this are international immigrants. This was aimed to exclude from the analysis children born in England and include the vast majority (92%) of international immigrants who are over the age of 15. 14
The numbers of first registrants aged 15 or over were compared to the official estimates for international migration. This was complex since the official estimates are for immigration into the UK, while the first registrants were selected on the basis that they had registered with a practice in England. Some may have moved to England from other parts of the UK. A crude comparison shows that there were more first registrants in England than the officially estimated number of international immigrants to the UK (respectively, 550,000 and 468,000 for 2003; 583,000 and 549,000 for 2004; 625,000 and 537,000 for 2005). 14 Correlations at the local authority level were high (0.94). The Office for National Statistics uses NSTS data to supplement estimates for international immigration. 15
It is recognized that not all first registrants will be international immigrants. Firstly, some English-born people may not be allocated an NHS number until later in life. Though numbers are likely to be small, they may be clustered in certain areas. Secondly, some people will mistakenly be assigned a new NHS number when they register with a general practitioners (GP), even if they had previously been registered elsewhere. Some people reportedly register under a new name in order to increase drug supplies. 16 Thirdly, administrative errors may have meant that some old registrations were not loaded onto NSTS. Conversely, our first registrants might exclude some immigrants potentially of interest. It is not compulsory to register with a GP and some people may not do so. Undocumented immigrants will be excluded, as will immigrants who registered with a GP during a previous stay in England.
Hospital utilization data (Hopsital Episode Statistics) was linked to NSTS data at person level using a pseudonymized NHS number. The proportion of admission episodes that could be linked was high (95.47% for 2004/5; 95.83% for 2005/6; 96.55% for 2006/7).
The population of first registrants over the age of 15 was compared to the general population of England and to a subgroup of within-England migrants. Within-England migrants were defined as those who had changed general practice within the year. It is thought that the majority of these will have changed location and not just doctor, and indeed this assumption underpins national statistics for internal migration within England.
In order to select a subgroup of within-England migrants that was similar to the first registrants, propensity matching was used. 17 This technique uses the propensity score to summarize several underlying characteristics in one number; if comparators are selected to have the same propensity score as the first registrants, their underlying characteristics should also be similar. Balance was sought on age band (5 year bands from age 15 to age 34; 10 year age bands to age 64; 65+), sex, and deprivation decile (based on the Index of Multiple Deprivation 2004, according to an aggregate of the practices population's place of residence). Seperate models were produced for three sets of first registrant cohorts: those registering with a general practice for the first time in 2003/04, 2004/05 and 2005/06. The closeness of the comparators to the first registrants was assessed by the standardized difference, which is defined as the difference in the sample means as a percentage of the square root of the average of the sample variances. While there is no clear consensus on the issue, some researchers have proposed that a standardized difference of greater than 10% denotes meaningful imbalance in the variable. 18
The analysis of hospital utilization was based on the proportion of people who had one or more inpatient admission. We considered trends both between cohorts (migrants arriving in 2003/04, 2005/06 and 2006/07) and within cohorts (how the admission proportion changes with duration of residence). We estimated the proportions admitted for obstetrics and neonatal care using Healthcare Resource Groups. In addition, the use of hospital care was expressed as an indirectly standardized admission ratio, standardized by age and sex to the admission rates of the English population. A rate of 100 means that admissions are at the national average rate for the given age and sex profile.
Results
Compared to within-England migrants, first registrants were younger and were registered with practices in more deprived areas (Table 1). After greedy matching on the estimated propensity scores, the first registrants and matched subgroup of within-England migrants were similar. The standardized difference was less than 2% for all variables.
Comparison of first registrants aged 15+ to all other registrants aged 15+ and the matched comparator subgroup of within-England migrants
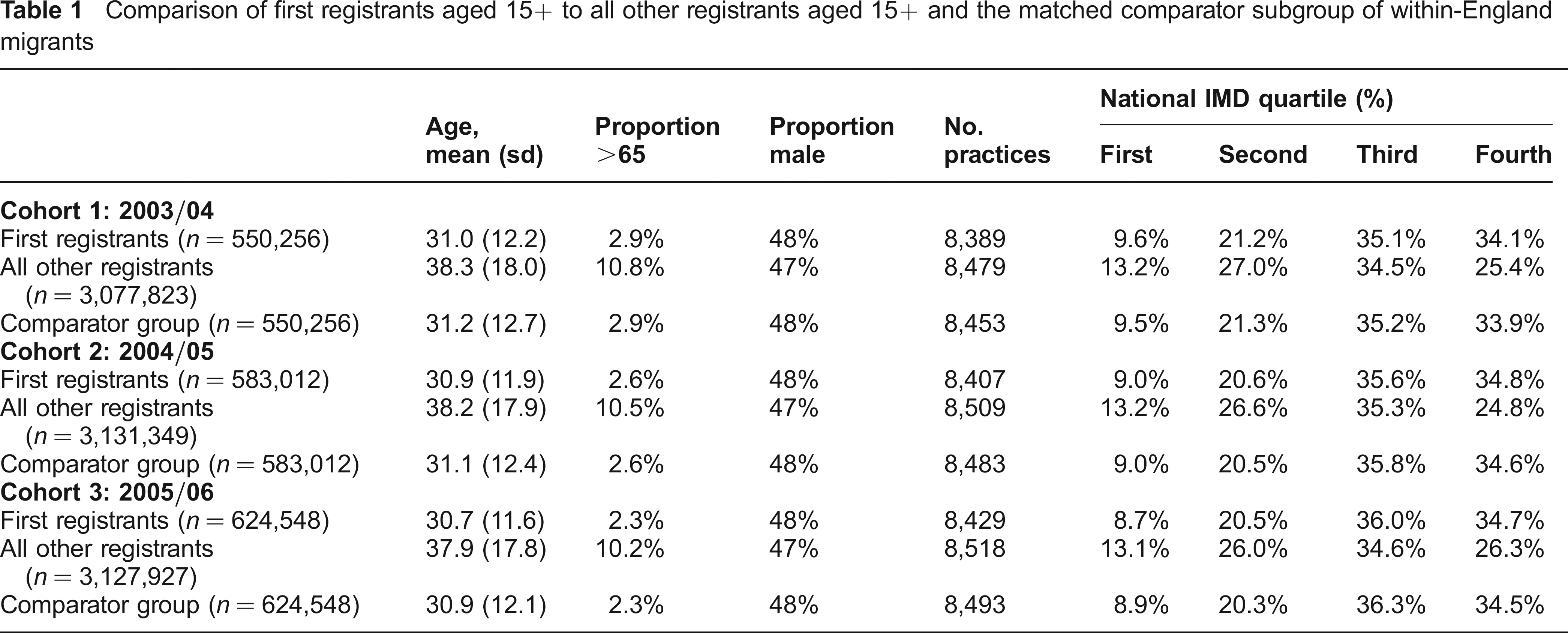
Figure 1 shows the percentage of 2003/04 first registrants who had a hospital admission each month, and the equivalent figures for the corresponding subgroup of within-England migrants. Confidence intervals are not shown because the they are small (+/- 0.03%, n = 550,256). Admission rates fell slightly after an initial peak following registration and first registrants were less likely than their comparators to have an admission, with these differences persisting for several years. Similar observations were found for the 2004/05 and 2005/06 cohorts.
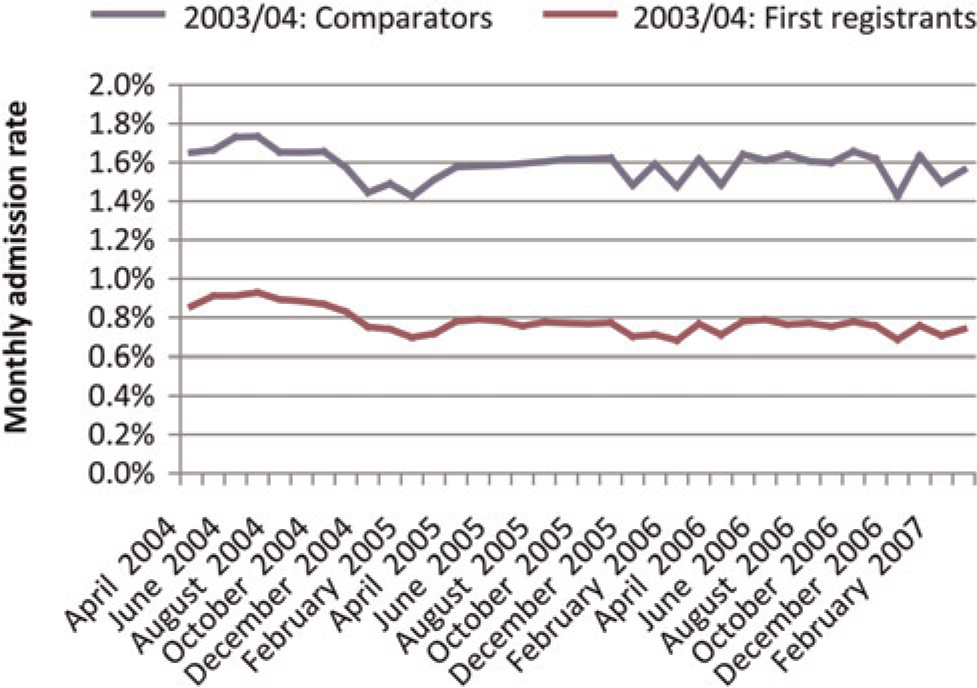
Proportion of first registrants aged 15+ years and matched comparator group being admitted to hospital (2003/04)
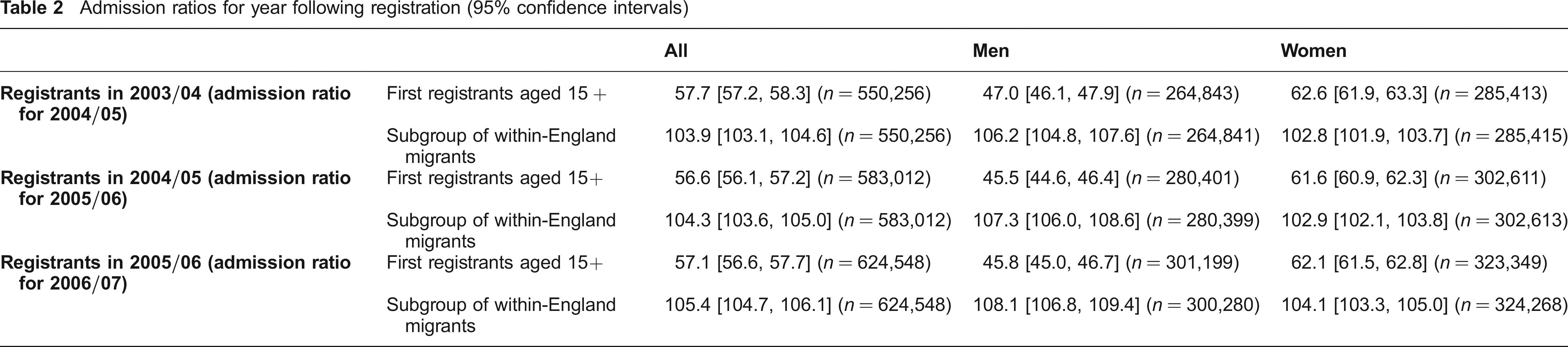
Table 2 shows indirectly standardized admission ratio for the first registrants and the matched subgroups of within-England migrants. The first registrants’ admission ratios (56–57) were about half the national rate (100). The first registrants also had lower admission ratios than the corresponding matched subgroups of within-England migrants (103–105). Analysis by age showed that the standardized admission ratios were lowest for first registrants aged 15–24 (53–56) but that differences from national ratios existed for all age bands and across all cohorts. 3.3% of the first registrants had an admission for obstetrics and neonatal care, compared to 3.6% of the matched subgroups of within-England migrants.
Admission ratios for year following registration (95% confidence intervals)
Discussion
Main findings
First registrants aged 15 or over were about half as likely to have an admission as the general population of England, after standardizing for age and sex. They were also less likely to have an admission than within-England migrants of similar age, sex and area of social deprivation. Compared to the within-England migrants, the lower admission ratios for first registrants persisted over several years. These patterns were observed for three consecutive cohorts of first registrants, including those who arrived before and after the accession of eight central and eastern European countries to the European Union in May 2004. Rates of hospital admisson for obstetrics and neonatal care, which includes childbirth, were lower for first registrants than for the matched subgroup of within-England migrants. This finding raises a number of questions about international immigrants’ use of health services, assuming first registrants aged 15 or over are an adequate proxy for such people.
Limitations
We cannot monitor the emigration of people who have migrated to the UK. This will lead to an underestimate of admission rates. When surveyed on arrival, around 45% of international immigrants indicated that they intended to stay in the UK for less than two years. This fell to under 20% for those aged 45 and over. 19 Though it is possible that some immigrants will have left the UK, hospitalization rates appear to have remained consistently lower over time.
Matching rates between the registration data and Hospital Episode Statistics were very high, with over 95% of hospital attendances being matched to the registration data, but it is possible that the admissions that could not be matched represented a disproportionately high number of immigrants. A proportion of immigrants will also arrive at accident and emergency departments (A&E) without previously registering with a GP. Indeed, there have been reports of immigrant women presenting very late in pregnancy not having had a routine medical examination, and so presumably not having been registered with a GP. 20 Both of these scenarios could mean that the admission rates underestimate the true rate for immigrants. Propensity score matching can account only for variables that were observed and not for any characteristics of first registrants that could not be observed, including ethnicity.
Implication
This analysis provides strong evidence, at a national level, that international immigrants arriving between April 2003 and March 2006 are likely to have used secondary care considerably less than established residents and within-England migrants. This has implications for local planning of services. It is in line with the the ‘healthy migrant effect’ reported in the literature 21 though there are a number of other possible explanations. These include differences in access to primary care, different thresholds for referral to secondary care, and other barriers to acccess. Some studies have shown that barriers associated with ethnicity and communication problems may exist in service providers. 22 Another possibility is that some international immigrants might return to their country of origin for hospital treatment. Such a phenomenon has been posited as an explanation for the lower mortality of migrant groups. 23
Footnotes
Acknowledgements
The authors acknowledge support from Jennifer Dixon, Colin Sanderson and two referees, who provided comments. This paper describes analysis that formed part of a wider DH-funded project ‘Developing a person-based resource allocation formula for allocations to general practices in England’ to which a team of individuals contributed from the following centres: The Nuffield Trust; Centre for Health Economics, University of York; Health Dialog, Portland Maine; Graduate School of Public Service, New York University; Department of Health Services Research and Policy, London School of Hygiene and Tropical Medicine. The full copy of the report of the project can be found at ![]() .
.