
Abstract
Objective
To study changes in health services consumption following substantial reduction in the availability of local emergency services in a small municipality population.
Method
A dynamic cohort (21,000 residents of Viborg County, Denmark, of which 2,300 from Morsø municipality) was followed, 1997-2003. Data were extracted from administrative registries including information on individual use of emergency services and other hospital care, contact with GPs and socioeconomic background. Health services' use by the Morsø population was measured before reduction in emergency room opening hours, during a period of reduced opening hours and after closure, compared with the rest of Viborg County.
Results
Emergency service use did not change among Morsø municipality residents compared to other Viborg County residents. Compared to men in other parts of the county, Morsø men did not change their use of substitute health services. By contrast, Morsø women compared to the rest of Viborg county reduced their use of GP services in terms of face-to-face visits (β= -0.08, P = 0.020), telephone consultations (β= -0.11, P = 0.007), home visits (β= -0.48, P = 0.009), and their inpatient hospital utilization (β= -0.12, P = 0.022) during the period when emergeny services were only available in the daytime.
Conclusions
Emergency services at neighbouring hospitals (40 kilometres distance) were able to compensate, in part, for the decreased local emergency service provision. Concurrent changes in health care utilization patterns were observed among local residents that varied by gender.
Introduction
There is a trend throughout the world to reduce the supply of emergency services in small hospitals and to concentrate such services in larger hospitals in order to increase efficiency of resource use.1–3 Because of the greater distance to neighbouring emergency services and/or a reduction in opening hours of local services, the result will be reduced access to emergency services for the population in the catchment area of the closed emergency room.
Among the potential consequences for patients are delays in contact with an emergency department (ED) and, possibly, with medical personnel at large. Patients' options include contacting an alternative provider, such as a general practitioner (GP), a practice nurse or a pharmacy, depending on the type of problem; visiting another, possibly distant, ED; and not using health services at all, relying on family or self-care.
Studies on the appropriateness of ED use suggest that a substantial proportion of visits are based on non-urgent or minor conditions,4,5 so that many visits could be simply omitted or substituted by visits to GPs, for example.4,6 Thus, emergency facilities to some extent may function as substitutes for GPs out-of-office hours. 7
The amount of published research on the consequences of closing or restructuring EDs is scant and studies have produced very varied findings in terms of the consequences of ED closure.8–11 More studies have been published on the consequences of closing or downsizing entire hospitals, and most of these have identified a subsequent decreased use of hospital services by the local target population.2,12,13,14,15 Contrasting this, other authors have found no or little reduction in hospital use in the population of the catchment areas of closed smaller hospitals.16,17,18 Following change in access, inpatient use has been found to be replaced to some extent by utilization of other services, such as outpatient services and nursing homes, 19 day surgery, 13 and GP visits. 18
Our aim was to estimate the impact of a reduction in a municipal population's access to local emergency services on the use of other local services (e.g. contacts with general practice, short hospital stays, and visits to EDs situated farther away).
Methods
Setting
The study focuses on changes in health services consumption associated with closure of emergency services in Morsø, a small municipality (population, 23,000 in 2003 20 ) in Viborg County (population, 234,000 in 2003 20 ), Mid-Jutland, Denmark. The local population is served by Nykøbing Hospital, which is situated in the urban part of the municipality. In 1998, 63% of ED visits by Morsø residents were to Nykøbing Hospital; 83% of ED patients in Nykøbing Hospital were Morsø residents. Until the end of 1999, the hospital operated a 24-hour emergency department, which was reduced to a day time emergency clinic in 2000. In September 2002, the daytime emergency clinic was closed. The nearest hospitals with emergency departments (Skive and Thisted hospitals) are both 30 kilometres from Nykøbing. During 2000–2002, Thisted and Nykøbing hospitals joined administratively to form a single unit for the provision of emergency room services.
In Denmark, all primary and secondary services are free of charge to the consumer and financed from taxation. Thus, there is no financial obstacle to health services' use.
Study population
A 10% sample (approximately 21,000 individuals) of the population of Viborg County, including Morsø municipality, was followed from 1997 to 2003. Based on the individual person identification number assigned to all Danish residents, the sample was drawn from the National Person Registry based on 37 randomly selected dates of birth among the 365 possible dates of the year. The sample was updated on 1 January for each of the study years, 1997–2003, to include newborns and immigrants and to exclude deceased persons and emigrants. The number of study participants over the study period was 1,457 males and 1,366 females in Nykøbing municipality and 13,028 males and 12,878 females from other parts of Viborg County. The population sample number varied from year to year, but on average 2,300 sample members were from Morsø municipality and 19,100 sample members from other parts of Viborg County, yielding a total of 106,240 observation years, of which 16,100 years were by Morsø inhabitants.
Data
Data were obtained from public administrative population registers, run by Statistics Denmark (www.dst.dk/HomeUK.aspx), which ensured that there were no missing individuals or missing information. The individual sample resident's record, consisting of a number of linked variables, formed the basic data structure. Besides information on residence, the individual record included age, sex, cohabitation, education, family income and use of health services (i.e. the annual number of ED visits; contacts with general practice [in-person face-to-face, telephone consultations, and home visits]; all admissions to hospital and one-day stays; and inpatient days). Status variables, such as age and residence, were updated on 1 January each year, whereas flow variables, including health service use, were cumulated for the calendar year. No data were collected for the current analysis on morbidity or mortality.
Design
Two quasi-experimental designs were used: a before-and-after study comparing health services' consumption by the population samples of Morsø municipality before (1997–1999), during (2000–2002) and after (2003) the reduction in emergency room opening hours and staffing (day time clinic), and its subsequent closure; and a comparative analysis, 1997– 2003, of health services' use by the population samples from Morsø municipality compared with the rest of Viborg County.
Analysis
Since the utilization rate (UR) was approximately Poisson-distributed, Poisson regression was employed with the UR as the dependent variable and explanatory dichotomous variables of calendar period (2000–2002 versus 1997–1999 and 2003 versus 1997–1999), residence (Morsø versus other parts of Viborg County) and their mutual interactions. However, to avoid distributional assumptions about means and coefficients from the regression analyses, non-parametric bootstrap techniques were applied (1500 replications) to estimate standard errors and confidence intervals. 23
The significance of the mutual interaction term indicates the change in health services' use specifically by Morsø citizens when ED supply changed at Nykøbing Hospital. A positive interaction parameter indicates increased utilization specifically by Morsø residents; i.e. exceeding the increase in the rest of the county population during the same time. A negative interaction parameter denotes decreased utilization specifically among Morsø residents.
All analyses were conducted separately for each gender and regression coefficients were adjusted for the covariates of age, cohabitation, educational level and family income as well as the yearly trend to control for pre-existing trends in the use of health services.
As an interaction term was included, its component variables were retained in the model. For simplicity, only the coefficients on the interaction terms themselves are shown. P ≤ 0.05 was applied as a general significance level. The Pseudo R2 Statistic21,22 was used as a measure of goodness of fit.
Results
ED visits
Among Morsø municipality residents, the rate of male ED visits was significantly lower in 2003 than in 2000– 2002, but not lower than in 1997–1999 (Table 1). Among females, the rate did not vary significantly over the study period. Among Viborg County residents (excluding Morsø), the mean ED UR was the same in the three periods for males, while the ED UR among females was lower in 2003 than in 1997–2002 (Table 1).
Utilization rates (UR, year 1, with bootstrapped 95% confidence intervals [CIs]) of health services, by period indicating local (Morsø) emergency department (ED) functioning and by gender, among 1457 male and 1366 female residents of Morsø municipality and among 13,028 male and 12,878 female residents of the rest of Viborg County, Denmark, 1997–2003

GP = general practitioner
Use of substitute services
Among Morsø males, the rates of in-person GPs consultation in the two periods, 2000–2002 and 2003, were higher than in 1997–1999, and the rate of telephone GP consultations increased between 1997–1999 and 2003, and between 2000–2002 and 2003 (Table 1). Among females, the rate of in-person GP consultations was higher in 2003 than in 1997–1999, while the frequency of home visits decreased between 1997–1999 and 2000– 2003. Hospital admissions and hospital one-day admissions increased between 1997–2002 and 2003.
A comparable trend in both types of GP consultations was found among males in other parts of Viborg County (Table 1). In addition, the rate of home visits decreased between 1997–1999 and 2000–2003, while one-day admissions increased between 1997–1999 and 2000– 2003. The mean number of inpatient days was lower in 2003 than in 1997–1999. Among Morsø females, in-person and telephone GP consultations and also one-day admission rates were higher in 2003 than in 1997–2002. Hospital admission rates and the mean number of inpatient days were both lower in 2003 than in 2000–2002 (Table 1).
Morsø residency and change in ED visits and in substitute service use
No significant interaction between Morsø residence (compared to residence in other parts of the county) and period (indicating varying levels of ED provision in Morsø municipality) was found in either gender with respect to ED use (Table 2). For Morsø males, there were no significant changes in use of substitute health services. For Morsø females compared to other females in the county, there were significant decreases in telephone consultations with GPs and home visits by GPs, and for in-person GP consultations in 2003 and hospital admissions in 2000–2002.
Interaction estimates # : Health services utilization in Morsø residents by level of local emergency service supply and gender, adjusted for utilization pattern trends in rest of Viborg County. Based on 14,485 male and 14,244 female residents of Viborg County, Denmark 1997–2003
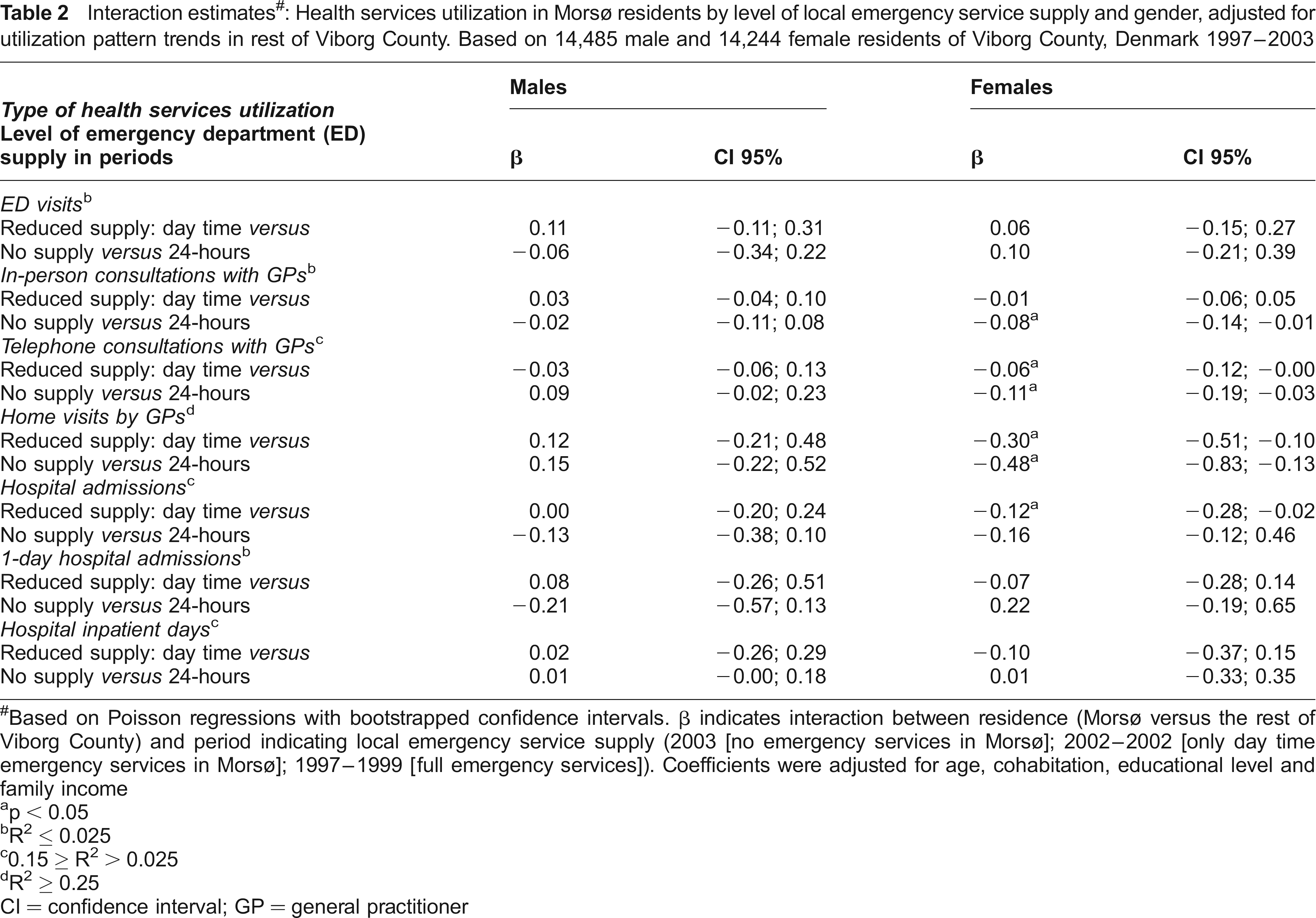
Based on Poisson regressions with bootstrapped confidence intervals. β indicates interaction between residence (Morsø versus the rest of Viborg County) and period indicating local emergency service supply (2003 [no emergency services in Morsø]; 2002-2002 [only day time emergency services in Morsø]; 1997-1999 [full emergency services]). Coefficients were adjusted for age, cohabitation, educational level and family income
p < 0.05
R2 ≤ 0.025
0.15 ≥ R2 > 0.025
R2 ≥ 0.25
CI = confidence interval; GP =general practitioner
Discussion
We found that the Morsø population's ED UR was maintained and was comparable with ED utilization in other parts of the county after closure of the local ED. Use of the local ED was substituted by use of services in neighbouring EDs. The only significant changes in health care utilization were moderate changes in primary health service consumption in females.
One of the methodological strengths of the present study is its completeness based on the availability of continuously updated, individual health care use data in combination with, likewise updated, individual demographic and socioeconomic information. This implies that, irrespective of socioeconomic and other background conditions, all residents contributed fully to the dataset.
We considered a 10% population sample as sufficient (with more than 106,000 observation years) to be able to detect changes in health services utilization, if they were not of negligible size. Infrequent, specialized unmet needs could not be detected, but are arguably less important in policy terms than overall population effects.
The majority of the regression models only captured a relatively small fraction of the variation in use as reflected by the low pseudo R2 found (Table 2). This suggests that factors other than the variables included in the models were also influencing health services' utilization.
The relatively small numbers of health service consultations per person per year mean that there are intrinsic limitations on the ability of this type of analysis to detect some types of changes in use. Thus, in 2003, the annual number of female face-to-face consultations with GPs was about four (telephone consultations: 3.6) contrasted with 0.06–0.08 emergency visits. Even if face-to-face consultations with GPs had been substituted for all emergency visits in 2003, this would not have produced a significant change in the level of face-to-face GP consultations. Moreover, due to delays in data reporting the follow-up period after ED closure was limited to one year. With a longer follow-up after ED closure, Morsø residents might have been shown to have changed their behaviour.
There is a striking contrast between the widespread interest in concentrating emergency services and the sparse empirical literature on subsequent changes in utilization and costs. In the Morsø case, residents sought emergency care at relatively close hospitals (maximum 40 kilometres distance), so that their ED UR remained unchanged irrespective of their reduced access to the local ED. Since ambulance services are free-of-charge and most Danish families own at least one car, distance does not seem to have presented a serious obstacle to ED service utilization in this case. Increases in use of substitute services were moderate and limited to female members of the affected population (Table 1).
We did not asses how the individual resident's health service utilization depended on the interaction between their socioeconomic characteristics and the changing provision of local emergency services. How residents with varying background coped with what they experienced as emergency situations during years of changing emergency service provision will be considered in future analyses.
Conclusions
In a western European national health system with free access to services, including hospital emergency services located no more than 40 kilometres away, the closure of a local, hospital emergency service brought about a modest reduction in health services' use in women and no significant change in men's use of services.
Footnotes
Acknowledgements
The research was supported by The Danish Health Research Council (grant no. 2028-00-0013), Sygekassernes Helsefond, grant no. 2005B083), and The Aarhus University Research Foundation (grant no. S-2005-SUN1-63).