
Abstract
Objectives
Swiss health care is relatively costly. In order better to understand the drivers of spending, this study analyses geographic variation in per capita consultation costs for ambulatory care.
Methods
Small area and longitudinal analysis of costs of ambulatory services covered by compulsory health insurance, 2003-07.
Results
The results show considerable geographic variation in per capita consultation costs, with higher costs in urban compared to rural areas. Areas with higher availability of care had higher costs, and residents of urban and high income areas used more specialist care and generated higher costs than residents of rural areas.
Conclusions
There are persistent regional differences in the per capita cost of ambulatory care that are not explained by demographic factors, access to care, or needs. It is likely that higher access to care leads to greater inappropriate use, particularly of specialists. Implementing gatekeeping systems and financial incentives that encourage better coordination of primary care may slow growth in costs and improve care.
Introduction
Per capita health care expenditures in Switzerland with average increases of five percent per annum since 2000 are among the highest in Organisation for Economic Co-operation and Development (OECD) member countries. 1 Efforts to slow expenditure growth include the introduction of managed care plans and the legislative restriction of ambulatory health care providers in 2002. 2 Despite these efforts, the steady growth in expenditure continues with health insurance premiums rising by 15–20% in 2010. In addition, cantonal fragmentation of the Swiss health system may be a major factor in regional variation of health care expenditures 3 and of low overall efficiency. 2 To date, research on the drivers of health care costs such as population needs and physician supply has been limited. 4 This study extends this research by analysing the marked geographic variation in per capita consultation costs for ambulatory care in Switzerland with two objectives:
To analyse the extent of need and provider supply side effects on per capita consultation costs; and To differentiate between the effects of the availability of primary and specialist care on per capita consultation costs.
Methods
Data sources
We analysed the complete claims data of compulsory health insurance for ambulatory services, 2003–07 (Santésuisse datapool). The data consisted of all Swiss ambulatory care providers and the consultation costs of patients classified by gender, by 20 age groups and by community of patient residence. Treatment costs were categorized into the costs of the consultation and the drugs prescribed. Ambulatory services are defined as any service provided by physicians and reimbursed by compulsory health insurance in an ambulatory, non-hospital setting.
Statistical analyses
We summarized the data at two geographic levels: utilization-based service areas for primary health care (n = 1034 (2003) – 1023 (2007); 5 and political communities (n = 2721 in 2007). Adjusted total per capita consultation cost for ambulatory care at the community level was the main outcome. We developed hierarchical multilevel linear 6 models to take account of the two-level data structure and used the values predicted by the models as a representation of adjusted per capita cost. Independent analyses for each year were performed because size and location of health service areas changed over time.
Demographic factors and patient need were analyzed at the community level. Socioeconomic characteristics and differential access to care were assessed by including a nine-level classification of communities developed by the Swiss Federal Statistical Office (urban, suburban, high income, peri-urban, tourist, industrial-tertiary, rural-commuter, agricultural-mixed, agricultural rural) in the models. 7 This classification is mainly based on the notion of hierarchic relationships between urban centers and peripheral communities and includes criteria of economic, geographic and social differences together with measures of urbanization and commuting characteristics.
In order to account for the decentralized nature of Swiss health care, we included two variables reflecting specific cantonal attributes. The first classified communities as within cantons that: allow that physicians to dispense drugs directly to their patients (‘self-dispensing’); restrict such direct sales of drugs to emergencies only and patients must get repeat prescription drugs in a pharmacy (‘prescription only’); or allow both channels of dispensation (mixed forms). The second variable adjusted for cantonal differences is the annually negotiated tariff factor (cost weight) for reimbursing physicians' services (TARMED). 8
The following table summarizes the explanatory variables included in the models:
Level I (community attributes n = 2717–2721 depending on year)
Mortality (number of deaths/1000 residents); Gender ratio; Type of dispensing of medication (prescription only, ‘self-dispensing’, mixed forms); Community type (9-levels).
Level II (service area attributes, n = 1034–1023 depending on year)
Area code of the service area (clustering variable); Number of primary care physicians per 10,000 inhabitants (GP density); Number of community-based consultants, i.e. non-primary care physicians per 10,000 inhabitants (specialist density) Presence of a hospital providing ambulatory services (coded as a binary variable with 0 for no hospital and 1 for at least one hospital); Annual TARMED reimbursement factor.
Presence of hospitals, drug dispensation, and community type were treated as classification variables. Continuous explanatory variables were centered to facilitate parameter interpretation. Results for classified data were interpreted as least-square means (LS Means) with 95% confidence intervals (95% CI). Variance components were additionally calculated. Model fit indicated no violation of basic assumptions for linear models. The level of significance was set at 0.05 (two-sided) and monetary data are given in Swiss Francs (CHF).
Results
Characteristics of communities and health service areas
Consultations per capita showed a 1.3 fold variation between urban centres and agricultural rural communities, and a 1.6 fold variation between high income and agricultural rural communities (Table 1). The proportion of per capita costs accounted for by GP consultations was 1.5 times higher in agricultural rural communities than in high income communities. High proportions of GP costs are found in rural and alpine areas of central and southern Switzerland, whereas low GP-cost proportions are seen in urban centres around Zürich, Basel, Lausanne, Geneva, and in southern parts of the country around the cities of Locarno and Lugano.
Characteristics of political communities, averages 2003–07 with interquartile ranges
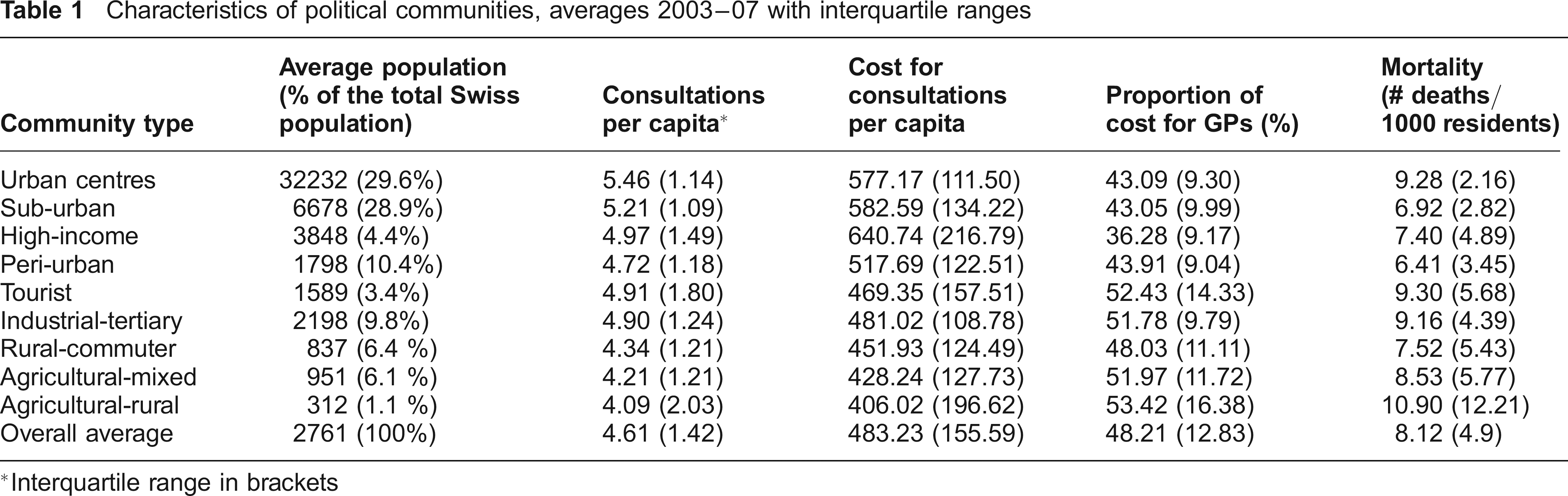
Interquartile range in brackets
The average physician density at the level of health service areas was 8.3 GPs and 3.9 specialists per 10,000 inhabitants (Table 2). Hospitals providing ambulatory care were present in 22% of service areas. Between 2003 and 2007, GP supply decreased by 0.8%, whereas specialist supply increased by 8.3% and the proportion of service areas with ambulatory hospital departments decreased from 24% to 19%. The proportion of GPs among all ambulatory physicians was 80% and remained almost stable in the period 2003– 07. There were regional differences with average proportions of GPs in urban health services areas of 77% and 95% in rural areas.
Characteristics of health service areas 2003–07
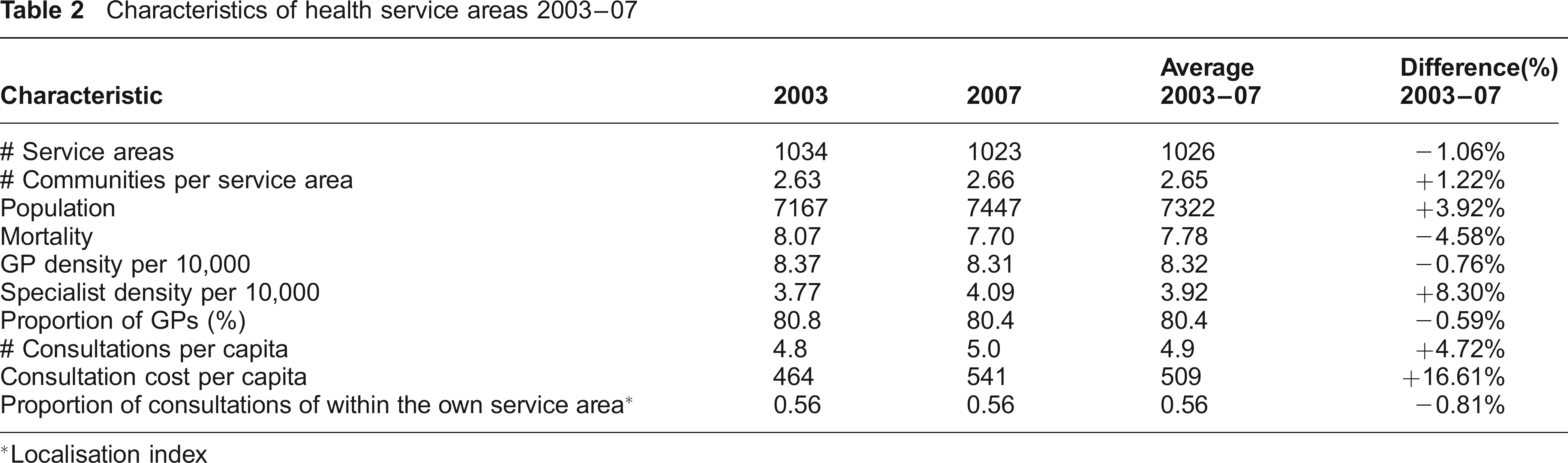
Localisation index
There was an average of 4.9 consultations per capita per year with an ambulatory care provider (5% increase for 2003–07). Average unadjusted per capita consultation costs at the service area level were 509.1 CHF and increased by 17% in the period.
There was a moderate positive correlation between the supply of GPs and specialists across service areas. (Spearman correlation coefficients P = 0.22). GP supply was weakly correlated with per capita consultation frequencies and cost (P < 0.2). A stronger correlation was present between specialist supply and number of consultations (P = 0.24) and consultation cost per capita (P = 0.40). In contrast, areas with a higher proportion of GPs among all ambulatory care physicians had lower consultation frequencies (P = -0.17) and lower per capita costs (P = -0.32).
Need and provider effects
Models of per capita consultation costs showed consistent and significant effects for regional mortality, for the proportion of women and for community-typology, irrespective of year. Adjusted consultation costs increased by 2.2–2.8 CHF for each additional death per 1000 residents and an additional percent of women in the population resulted in an increase of 121.6–192.4 CHF (Table 3).
Effect estimates in Swiss Francs on per capita consultation costs by year

Costs for each additional death per 1000 residents
Costs for each additional percent of women in the population
Costs per additional GP or specialist in a population of 10,000 residents
Costs for each additional percent of the TARMED reimbursing factor
P-values in brackets
Analyses showed significant and positive effects for GP and specialist density on per capita consultation costs. Depending on year, the following effect estimates were obtained: costs were higher by 2.9–4.4 CHF for each additional GP in a population of 10,000 and by 1.0– 1.8 CHF for each additional specialist, respectively (Table 3). In 2003–07, areas without ambulatory hospital departments had significantly higher per capita costs for ambulatory consultations (plus 18–31 CHF or 4–6%) (Table 4).
Regional and temporal variation of adjusted per capita costs
Per capita consultation costs adjusted for all explanatory factors (predicted values) showed comparable patterns over the period 2003–07. Adjusted costs varied 3.3– 4.6 fold across all Swiss communities, 2003–07, and costs were highest in urban, densely populated areas and lowest in remote and rural areas. Differences of LS means indicate 1.4–1.5 fold higher cost estimates in high income communities compared to agricultural rural communities (Table 4).
Least square means for per capita consultation cost in Swiss Francs of categorized variables by year

During 2003–07, costs in urban, sub-urban and in high income communities increased by 14–17% and by 18–26% in rural and agricultural communities (Table 4). Cost estimates were significantly different between cantons with mixed drug dispensing and other forms of dispensing drugs for 2004–07, but not for 2003. Differences between ‘prescription only’ cantons and ‘self-dispensing’ were statistically significant for 2003 and 2004. Estimated consultation cost increased during 2003–07 by 14% in ‘prescription only’ cantons and by 21% in cantons with both other forms of drug dispensing.
Variance components indicate that, depending on year, models account for 24–27% of the variance of consultation costs: 4–9% and 4–11% of the service area level variations was explained by GP and specialist density, respectively. Mortality accounts for 5–8% of the explainable variation between communities and the respective proportion for the nine-level community typology ranged from 10–13%.
Discussion
Results from this study provide a unique view of variation in utilization and costs of physician services during a period of growth in health care expenditures. Costs per capita grew faster than consultations per capita implying a remarkable increase in prices and/or quantity of services provided per consultation. Our results indicate that much of this variation cannot solely be explained by patient need and that supply factors appear to be major driving forces. The results also show that the physician supply predicts costs. Allocating ambulatory health care resources based on principles of need, equitable access and efficiency remains, therefore, a major challenge for Swiss health policy. Recent policy decisions in Swiss ambulatory care to contain cost tend to focus on payment reform and on restricting the accreditation of physicians. Not surprisingly, these legislative sanctions are controversial reflecting the tension between the principles of (regulated) competition and tighter governmental control.
Demand effects
Substantial cost differences were observed between urban/metropolitan and rural areas after adjusting for supply side factors, regional mortality and socioeconomic characteristics. Residents of urban and high income areas used more specialist care and generated higher costs than residents of rural areas. Such patterns can be interpreted as inadequate access to care with implicit rationing of specialist care in rural areas. But these inequalities may diminish in the future as growth of costs was more pronounced in rural than urban areas.
Our analysis controlled for socioeconomic and other community-level factors. It can be assumed that the use of health care is not only influenced by access to care and socioeconomic factors, but also by behavioural characteristics of patients such as personal preferences, cognition and beliefs9,10 not accounted for by our model. Such preference-sensitive characteristics may additionally be facilitated by a health system that provides comprehensive insurance coverage and guarantees virtually free choice of providers. Our findings are consistent with a well established theoretical framework for understanding determinants of health care use 11 and may thus provide further evidence that demand side-effects may result in unnecessary medical requests and increasing cost. Strengthening mechanisms at the health system level that improve patient involvement and promote value-based decisions in terms of outcome and functional status may be helpful to prevent overuse of services.
Supply side effects
The density of GPs and specialists explained 15–19% of the variance in per capita consultation costs and higher supply was associated with higher utilization irrespective of socioeconomic characteristics of populations and regional mortality (as a proxy for need). Structural aspects of supply – in addition to density per se – are also key factors in regional differences in per capita consultation cost. The linear association between high per capita cost and more use of specialist care is certainly not confined to Switzerland 12 and likely reflects the effects of a provider-driven health system together with free choice of care providers for almost everyone.
Previous studies demonstrate that better health system performance is not associated with high levels of spending, 13 high density of supply,14,15 high intensity of care 16 on higher levels of specialist care. 17 Our findings, therefore, are suggestive of resource overuse or misuse within the Swiss health system and supply-sensitive care may be an important component in this context. 18 Measures such as strengthening gatekeeping or the co-ordinating function of GPs and promoting practice styles that induce fewer discretionary interventions 19 may be important.
Other structural factors that influence per capita consultation costs are the availability of ambulatory hospital supply and the distribution channels of prescription drugs. Not surprisingly, areas with ambulatory hospital departments had significantly lower per capita costs for ambulatory consultations as ambulatory hospital departments substitute for some ambulatory health care services 20 which are not included in our data. It appears also that costs were highest in areas with mixed forms of dispensing drugs. The rise of costs 2003–07 was 7% higher in areas with mixed or self-dispensing than in ‘prescription only’ areas. An explanation may be different and changing priorities of physicians in patient scheduling 18 and/or differences in patient expectations of receiving medication when deciding to consult a physician.
Limitations
The most important limitation of this study is that information about the health care needs of populations is not available at small area level in Switzerland. Cantonal health data such as the Swiss Health Survey 21 cannot be used in a study based on small are patterns of utilization. We therefore used raw mortality rates as estimates of need which are currently the only non-utilization based measures of population health available at small area level. The use of mortality rates as a representation of need may be in adequate in an ambulatory care setting. Endogeneity bias (i.e. an association between the level of expenditures and mortality in the sense that areas with higher mortality may attract more physicians) may also have affected our results.
It can also be argued that age should be included in the analysis, though proximity to death is a far more important predictor of expenditure than age. 22 The analysis would be improved greatly with valid information about regional age structures and the related health care needs of populations.
Conclusion
Our data show persistent regional differences in per capita utilisation of ambulatory care that cannot be explained by demographic factors, access to care, or regional mortality rates as a proxy for need. Supply factors such as GP and specialist density were associated with increased utilization, and the obvious higher share of costs generated by specialists in high spending areas provides evidence that unrestricted access to specialists may be an important factor in health care expenditure growth. This calls into question the equity and efficiency of Swiss health care, and implies that there are effectively transfer payments from low to high spending areas within cantonal boundaries.
Aligning consultations with patients' needs and wants will require strengthening value-based decisions by patients and changing the organization of care, for example, by promoting gatekeeping systems and by setting financial incentives that discourage direct access to specialists by patients. On the supply side, there is a need for better monitoring of the referral process from primary to specialist care.
The continued growth in costs will remain a top concern of Swiss and other health care systems. In particular, the USA shares several similarities with the Swiss system, including fee-for-service payment, physician-owned practices and considerable fragmentation. Swiss health care can, therefore, be seen as an example of a delivery system that provides both useful and wasteful care, while ignoring unmet needs and rising expenditure. Improvements in effectiveness and efficiency will require greater care integration and the reform of reimbursement systems.
Footnotes
Acknowledgements
The study was exclusively funded by resources of the Institute for Evaluative Research in Medicine of the University Bern. By contractual agreement, Santésuisse - the owner of the data - had no involvement in the preparation of the present manuscript.