
Abstract
Objectives
To understand the challenges and opportunities associated with the introduction of assistant practitioner (AP) roles supporting the work of ward-based registered nurses (RNs) in National Health Service (NHS) acute hospital trusts in England.
Methods
Three case studies of NHS acute hospital trusts. This paper presents qualitative findings, drawing on documentary data sources and data generated through interviews and focus group discussions.
Results
Introduction of APs into ward-based nursing teams has been variable, and often driven by external pressures rather than perceived organizational need. This, along with little national guidance, has created some confusion about the role, but at the same time has permitted flexible role development through ‘negotiated compromise’ at local level. While there are various areas of potential improvement in policy and practice, APs are generally perceived to have the potential to make a valuable contribution to patient care.
Conclusions
Findings from this study will help policy-makers, organizations and practitioners understand factors that enable and/or inhibit the integration of new assistant roles within existing occupational structures to develop innovative services and enhance patient care. These factors are important when considering how care will be delivered to maximize the skills of the entire nursing workforce.
Introduction
Nursing shortages are an international health policy concern, presenting significant challenges for health care providers. The UK National Health Service (NHS) spends 70% of its funding on staffing 1 and more than £4 billion is spent annually on training. 2 The effectiveness of the service is largely dependent on the effectiveness of the workforce. Over the past decade, the NHS has recognized the need to make improvements in productivity and efficiency. Efforts have focused on making better use of NHS human resources through role expansion and redesign. A significant development for both nursing and allied health professionals has been the emergence of the assistant practitioner (AP) role. APs can potentially contribute to the current Quality, Innovation, Productivity and Prevention (QIPP) initiative 3 which aims to identify how services can be redesigned to improve quality and efficiency.
Development of the AP role has been driven by a series of inter-related health-care policies including: employment policies; workforce restructuring; regulatory frameworks, including professional and support staff regulation; workforce preparation; human resource management, workforce pay and rewards; commissioning of services and financial pressures; changing patient populations; and rising public expectations of care and services.
Roles of assistant staff in the nursing workforce and locating the AP role in the nursing team
The processes by which the nursing workforce is segregated into registered nurses (RNs) and non-registered workers (or assistants) has been well documented. 4 The shape of clinical nursing is the culmination of diverse and complex sociopolitical interactions over time. Despite the introduction of the nursing register in 1919, nursing work has continued to be provided by a variety of workers other than RNs. In 2008, there were over 286,000 assistant staff supporting the medical (n = 133,662) and nursing and midwifery (n = 386,112) workforce. 5
Currently, there are two key areas of concern in relation to the future UK nursing workforce and the potential increasing role for assistants. First, a skills shortage due to retirement of an ageing nursing work-force 6 and second, moves to an all graduate-level registration for nurses. 7 It is inevitable that the roles of assistant staff and their contribution to the delivery of nursing care will rise up the policy agenda due to budgetary constraints and as health-care providers attempt to maximize the contribution of the entire workforce to deliver services.
Despite increasing numbers of assistants, there are still wide ranging debates about role boundaries between RNs and assistant staff. Understanding the AP role within these debates is therefore important.
Defining the AP role and understanding the policy context for the study
APs are ‘higher level’ support workers, who undertake formal training for their role. 8 This training is usually a national vocational qualification (a work-related, competence-based qualification) or foundation degree (a two-year degree level qualification combining academic study with work place learning). They are expected to function at level 4 on the Career Framework 9 (Table 1, available online only at http://www.jhsrp.rsmjournals.com/cgi/content/full/16/suppl_1/50/DC1), and usually banded at level 4 under the NHS Agenda for Change Framework (RNs start at level 5 on this national pay and grading system for all NHS staff). 10 APs are not currently registered or regulated by a professional body, but the future regulation of assistant staff in the UK is being widely debated.7,11
Introducing the AP role is an important UK workforce policy initiative, offering a potentially important career development for assistant workers. There is limited evidence regarding the introduction of AP roles into nursing teams. The focus of research has been the allied health professions,12,13 AP training, 14 or small scale, local evaluations of the role.15,16
Objectives
We aimed to establish: the policy expectations associated with AP roles; and perceptions and experiences of the challenges and opportunities associated with implementation of this policy initiative.
We examined relationships between both formal policy (espoused strategy) and informal negotiation of policy by staff in practice (emergent strategy). 17
Methods
A multiple-case (embedded) design 18 using sequential quantitative and qualitative methods was employed for the national study. 19 This paper draws on qualitative case study findings from a national study of the AP role. 20 The current analysis aimed to gain in-depth understanding of AP roles within the context of nursing teams, ward speciality and the organizations they were part of, by making comparisons with national policies. Findings from each case study were compared to determine both convergent and divergent findings. This paper uses documentary data sources and data generated through interviews and focus groups.
Sampling of case studies
Preliminary scoping work for this study highlighted wide variation in the introduction of AP roles in acute hospitals across England, as well as a diverse range of interpretations of the AP role. 21 We purposively sampled three NHS acute hospital trusts to include organizations where: the AP role was well established or recently introduced; there was variability between clinical ward in use of APs; differences in AP numbers employed; and variation in geographical characteristics. The case sites are summarized inTable 2.
Summary of case sites
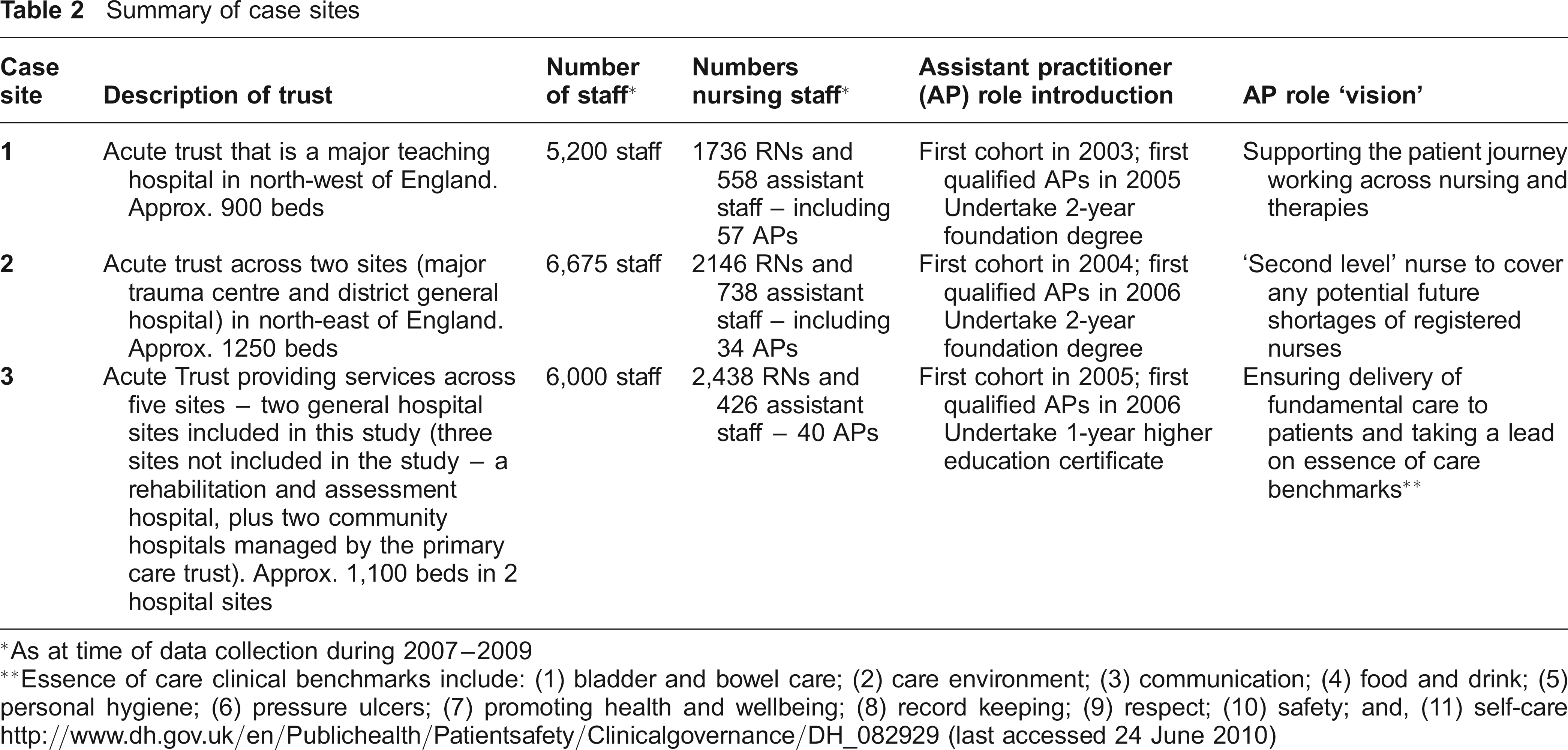
As at time of data collection during 2007-2009
Essence of care clinical benchmarks include: (1) bladder and bowel care; (2) care environment; (3) communication; (4) food and drink; (5) personal hygiene; (6) pressure ulcers; (7) promoting health and wellbeing; (8) record keeping; (9) respect; (10) safety; and, (11) self-care http://www.dh.gov.uk/en/Publichealth/Patientsafety/Clinicalgovernance/DH_082929 (last accessed 24 June 2010)
Data collection
AP job descriptions (n = 22) were collected related specifically to adult clinical areas where APs worked alongside RNs and undertook nursing-related tasks. These included acute general medical, rehabilitation, surgical and high dependency areas. These were used to corroborate and augment data from other sources, as well as prompt further investigation where there were contradictions between data. Detailed analyses of the job descriptions have been presented elsewhere. 22
To explore introduction and development of the AP role, a combination of interviews and focus groups were utilized. These interviews (n = 105) and focus groups (n = 7, with 31 participants) were carried out with a range of staff including APs, RNs, health-care assistants (HCAs), ward managers (with and without APs in their teams), other health-care professionals (such as therapists) and staff from senior nursing management (for example, directors of nursing and divisional managers). All of the interviews and focus groups were audio recorded (with participants’ permission) and transcribed verbatim.
The study was reviewed by a multi-centre research ethics committee (07/MRE04/20) and research governance approval obtained from each participating trust.
Data analysis
Parallel mixed data analysis was undertaken. 23 Job descriptions were analysed for key themes relating to clinical responsibilities of APs and comparisons were made within and across clinical settings in a case site and also across case sites. 22 Qualitative data (from focus groups and interviews) were analysed thematically, 24 initially within each case site and then exploring similarities and differences between the case sites.
Results
External pressure versus perceived organizational need
The extent to which AP roles were introduced into organizations because of perceived local need was questionable, although this did vary across case sites. Senior managers from case sites 1 and 2 described financial support from the Strategic Health Authority as driving introduction of AP roles. There was a suggestion that organizations may not have had the opportunity to fully consider the roles prior to their introduction (Box 1:1). Senior managers from case site 3 indicated that their motivations for introducing the AP role were driven by organizational need, independent of external influence or funds.Table 2 details the organizational ‘visions’ for the AP role, highlighting varied interpretations of the role.
Quotes from participants
It was something that, as a trust, we were being involved in. The Strategic Health Authority were pushing it as a workforce issue… There won't be enough trained nurses, so we're going to have to think of alternative… I'm not sure that the ward managers, and even the matrons and possibly directorate managers, I don't think they were quite sold on why we were doing it. (1: divisional manager 2)
[Ward Managers] kept seeing it that you're basically trading a band 5 nurse, you're losing a band 5 and replacing with a band 4. But I didn't see it like that… I saw it as gaining – changing a band 2 to a band 4. I didn't see it as one of my members of staff in the skill mix stepping down. I saw it as one of them stepping up. (3: surgical ward: ward manager 32)
But because there's not a [clear] job description and the job description that we've got is such a wide, and it covers everything, it's left up to yourself to develop your job description or up to the line manager to tell you what to do. (1: medical ward: assistant practitioner [AP] 61)
We have an ongoing, I wouldn't say battle, awareness of AP giving handovers which we're saying no; it needs to be the registered nurse. But the registered nurses argue back the AP is looking after the patients and therefore are the best person to give the handover report. That's a huge concern to me because what I'll say to the registered nurses [is] ‘well, why do we need you?’ If you are saying that the assistant practitioner can completely manage total patient care, what is the role of the registered nurse? So I am very concerned when I hear that, very concerned. (1: organizational manager 8)
I mean when you've maybe only got one AP on a ward I don't think that's really viable, you know, that poor AP is not going to make a great difference… I just think when there's one AP in an area, I just don't think, personally, I don't think it particularly works. (1: organizational manager 1)
Maybe a lot of it is around risk. You start going to a busy medical ward and you add an AP responsible for a group of eight patients and then you think, ah, I'm not quite sure whether I like that because you're not a nurse, you haven't got all that skill and knowledge. And we don't necessarily need all your therapy stuff here; what we need is nursing skills, assessment skills. And that's not what the [AP] role was designed to do – assessing. It was about delivering, assessed and planned care as far as I was aware. And that made me feel quite comfortable. (1: divisional manager 2)
At the time we were struggling to recruit people into rehab… you either love it or hate it. So we were struggling actually to recruit [RNs]. So if we had [APs] on board who were enthusiastic and wanted to progress and wanted to enhance their skills that seemed like a good idea. (1: medical ward: ward manager 47)
We have appointed because we wanted to reward people rather than appointing the person who wanted to take on that role… You don't choose a person because they've been in a place for a long time and, you know, they're quite good and we'll pat them on the head. You want somebody who really wants, is hungry for that role… So it's maybe that my disappointment is because it's the wrong person in the job… From what I've seen it's been a reward for long service or because they're a nice person or whatever, rather than what their motivation is for wanting to do it and are they strong enough to do it? (3: divisional manager 19)
I was aware that they had these two years and it was really intense and everybody was looking at them and reports were being filled in and then they finished and that was it… They felt like it'd just died a bit of death at the end of it. There wasn't anything. What next? (1: divisional manager 2)
Regardless of the perceived drivers for introduction of the AP role, the role had not been adopted in the majority of wards within these organizations. Actual numbers were relatively small in each of the case sites: APs comprised 10% of the assistant workforce in case site 1, 5% in case site 2 and 9% in case site 3. Reasons provided for resistance included: lack of suitability for the clinical speciality and patient population; lack of requirement for a role crossing professional boundaries; lack of distinction between senior health-care assistant (HCA) and AP role descriptions; reluctance to replace RNs with APs; and financial restraints. However, when introduced, most ward managers emphasized the gains associated with the role (Box 1, comment 2).
Blurred vision: tensions between organizational vision and practice realities
Despite a managerial vision for the AP role, it was apparent that ward staff perceived the AP role to be poorly articulated and communicated. The lack of clear job descriptions further reinforced these perceptions. Our analysis of job descriptions 22 revealed confused interpretations: in particular the extent to which APs were proposed as an ‘assistant’ or ‘substitute’ for RNs. AP roles were perceived as not being clearly guided by the job descriptions (Box 1:4).
Staff (organizational and ward level) from across organizations recognized there were confused messages about the role. This created uncertainty for ward staff, confusion for APs undertaking training and misguided expectations for HCAs who wanted to become APs. Upon qualification, this led to decreased role satisfaction for some APs. A number of tensions arose due to inconsistencies in AP roles both within and across organizations. This was often because of a lack of transparency of decision-making about the remit of APs. There were perceptions among ward-based staff that APs were being prevented from developing areas of practice that were sometimes undertaken by more junior HCAs, technicians or student nurses (for example, intravenous cannulation, catheterization and wound care). Discussions between managers about the role were rare.
Few senior managers were charged with responsibility for promoting and engaging staff with the role. Many senior managers were keen to highlight the lack of national policy guidance for developing AP roles. This had affected whether organizations adopted these higher-level assistant positions or not. Operationalization of the AP role within organizations was not well understood by ward managers. The AP role was largely defined and negotiated in practice; this is fundamental for understanding the development of the AP role.
Establishing role boundaries for APs
Across all case sites, the AP role was largely recognized and established through negotiation and socialization while the person was in post. There was widespread recognition that the AP role had largely developed in an ad hoc way. So, it was unsurprising that there were variations in the APs’ roles dependent on their specialities. However, this led to frustrations for APs both within and across organizations.
Establishing an acceptable role for APs had created challenges for the practice boundaries of existing staff, in particular RNs. Across organizations, a number of activities and areas of practice were highlighted by senior managers and RNs as ‘inappropriate’ for APs (Box 2). The AP role was overwhelmingly described in terms of what they should not do. This approach was exacerbated by the lack of clear job descriptions and the extent to which clinical activities were regarded as legitimate activities for the APs. Even though some activities were defined as ‘inappropriate’ for APs, the situation was not clear-cut. APs sometimes encroached on these disputed activities and areas (Box 1:4).
Activities and areas of practice that assistant practitioners (APs) should not do
Medicine's administration
Catheterization
Wound care and wound dressings
Bed management
Assessment of patients
Planning of patient care
Discharge of patients
Care of acute highly dependent patients
Nursing assessment and diagnosis
Ultimate responsibility and accountability for patient care
Communication of tests results to patients
Communication of patient information at nursing shift handover
Referral for medical attention
Co-ordination of ward activity and care
Staffing, and in particular RN availability, were an important influence on AP activities. In addition, relationships and levels of trust between the AP and other staff members often determined AP activities. Interestingly, APs highlighted that relationships in the ward team were a key influence on the work of all assistant staff. Upon completion of training, APs recognized that they had often undertaken delegated duties as HCAs because they were trusted by RNs, when they had no understanding of the implications of their actions. AP training was perceived as developing AP confidence to know and accept the boundaries of their assistant practice and promote patient safety.
A highly contested area of practice was development of the AP role in administration of medicines. APs expressed frustration that they could not administer medications, while RNs described this as creating an extra burden for them. However, there were split opinions on whether APs should ever be able to administer medications. Most senior managers and RNs felt this was a step too far, while a smaller number conceded that a limited formulary of medications for APs to administer was inevitable. The expansion of APs’ activities was perceived by some RNs as a potential threat. For others it was a way of reducing staff costs and providing ‘cheap labour'.
An in-between role: more than an assistant, but not registered
APs were not registered and this made it difficult for many APs to make visible their change in status and activities from their role as HCAs. APs felt they were being pulled in many directions. APs felt they were expected to continue to complete work they had undertaken as HCAs, making it difficult for them to embrace their new roles and for staff to change their expectations of the role-holder. A key point of discussion was whether APs were ‘trained’ or ‘untrained’ staff members. In the main, these staff were viewed as part of the assistant establishment in staffing rotas.
There were small numbers of APs in the case study wards (between one and five). Even where there were larger numbers, APs described feeling isolated because they often worked on different shifts to their AP colleague(s). Colleagues indicated that the small number of APs meant that they were limited in their ability to influence ward teams and to ensure maximum impact on patient care (Box 1:5).
AP accountability was a major point of discussion and concern for RNs at ward and senior management level because APs were perceived to be performing some ‘advanced’ technical activities while unregistered (Box 1, comment 6). However, APs viewed RNs as being ultimately responsible for of patient care and felt that certain aspects of their role should be more closely supervised by RNs, for example, admission assessments and care planning. Registration was discussed in all case sites to varying extents. Registration was suggested by a variety of participants as offering a way of: protecting the APs; promoting role clarity; increasing role recognition; clarifying lines of accountability; protecting patients; and promoting responsibility among APs. Nonetheless, not all staff (representatives from ward and management staff groups) felt that the AP role should be registered and the means by which registration and regulation would be achieved were not at all clear. In case site 1, this was further complicated by the APs working across professional boundaries.
AP role: a role for assistant staff to aspire to
Assistant staff were usually nominated by their ward manager to undertake training for, and promotion to, the role of AP. APs tended to be white British females in their mid-forties, who had considerable previous experience of the NHS (many working for over ten years as HCAs). Once nominated for training, many were guaranteed AP posts following course completion (case site 1 and 3). In case site 2, despite promises of an AP position, the APs had to apply for a job and not all were successful. No APs had been appointed from outside these organizations to work within ward-based nursing teams. The role was viewed as an opportunity for ward managers to retain and reward assistants who had worked in the organization for a number of years (‘home-grown’) and were recognized as ‘stars'. It was also used as a means of retaining and promoting assistant staff in clinical areas where it was sometimes considered difficult to recruit RNs (Box 1, comment 7).
The processes for AP nomination had potential to generate inequities. Since significant numbers of wards had resisted introducing APs, this could potentially disadvantage some HCAs in terms of their career progression. Divisional managers reported a lack of any strategic approach to identifying assistant staff who demonstrated sufficient potential to develop into the AP role. Whilst the AP position provided a significant progression for assistant staff, there were indications that rewarding long-standing staff may not always be the most appropriate selection criterion for the AP role. It was suggested by both senior and ward managers that, in some cases, people appointed to the role had become complacent and continued to function as HCAs rather than embracing the opportunities and challenges of the new roles (Box 1, comment 8).
Managers had conflicting views about who should become an AP. Some senior managers in case site 1 and 3 suggested that an assistant who planned to go on to be a registered practitioner should not do AP training. This was viewed as a waste of organizational resources and time for the individual. In case site 2, there appeared to be greater understanding of the AP role as a route towards registered practitioner training. However, other managers in sites 1 and 3 indicated that it was only when undertaking AP training that some assistant staff developed confidence and recognized their abilities. Therefore, excluding APs from undertaking registered practitioner training was perceived as creating inequity.
Concern was also expressed about the lack of continuing professional development (CPD) opportunities for APs when compared to opportunities for other staff (Box 1, comment 9). There was recognition that not all APs were receiving opportunities for an appraisal of their work. Additionally, APs reported lack of mentor-ship upon qualification and a lack of guidance about future opportunities. Yet, APs were taking on appraisal of their HCA colleagues and expected to provide support, training and mentorship to such staff.
Discussion
The analysis portrays the realities of introducing ward-based APs in acute hospitals. It has generated themes similar to the findings of other studies that have explored the introduction of new health-care roles. 25 However, this paper contributes specifically to debates concerning the introduction of new assistant roles, providing examples from practice of both the challenges and opportunities associated with higher-level assistant roles in nursing. Such roles are likely to have greater future policy significance as health-care providers decide how to ensure delivery of quality care within finite financial resources. Recent government policy has emphasized productivity, efficiency and quality and the contribution of assistant staff to this agenda is crucial to ensure that the skills of the entire workforce are used. Within the nursing workforce, assistant roles (and, in particular, APs) are likely to make an increasing contribution to care due to projected future shortages of RNs in the workforce.
RNs are shifting their work boundaries both upwards (by taking on increasingly complex medical tasks) and downwards (by redistributing some of their work to assistants). Through ‘vertical substitution', 26 APs are taking on roles and activities previously only undertaken by registered practitioners. A major consequence of vertical substitution is the potential for role conflict, role confusion and professional disputes. 27 The ways in which these manifest in practice have been highlighted by this study.
The chronological development of the AP role played an important part in shaping AP roles. In at least two case sites, there was initial confusion about the role of APs and identifying the organizational need for the role. The apparent lack of focus on resolving these issues at an early stage, highlighted by poor articulation of the role through job descriptions, played some part in the continued confusion and lack of preparedness of staff to manage the introduction and integration of APs into their ward nursing teams. Not all clinical specialities embraced the AP role. There were noticeable differences between the accounts of senior managers with a vision for the AP role and ward-based nursing staff who would have to work alongside the APs in practice.
The accounts of various participants highlighted disputes surrounding the boundaries of the AP role and that the role was largely negotiated in practice. This led to opportunistic development of the AP role, including APs themselves. Importantly, organizations established AP roles in terms of what they should not do rather than considering activities and scope of practice for these staff and clearly articulating these in job descriptions. The value of the AP role is that it can be responsive to local service needs and developed to support care delivery to patients. However, the notion that APs were a ‘flexible pair of hands’ was largely dictated by ward staffing levels and individual relationships. Facilitating APs to make the transition into their new role from their previous ones as HCAs was recognized as difficult. However, success in transition of these roles had the potential to enable organizations to maximize the skills and knowledge capabilities of assistant staff. If this is to be achieved, ward nursing teams need to discuss issues of accountability to ensure that all nursing staff are aware of, and comfortable with, the renegotiated boundaries and professional responsibilities.
We have highlighted ways in which the AP role complemented the work of ward-based teams. We would argue that future developments for this role largely depend on the resolution of a number of issues both locally and nationally. These include decisions regarding registration and regulation of the AP role, and opportunities for career development and progression through transferable skills and knowledge that are nationally recognized, as well as appropriate mentorship and CPD.
Conclusion
Any new role takes time to establish itself and, in all three sites, both APs and their organizations were struggling to find an appropriate role definition. Learning from these struggles is likely to be valuable for other trusts. The study also highlights a range of organizational and individual tensions raised by the introduction of the AP role. How these are resolved, whether through implementation of formal policy initiatives from central government or through more local policy initiatives sensitive to specific contexts, will mediate the definition and development of the AP role. Much of this has yet to be worked through. We have described possible ways in which the role impacts on processes of care, service delivery and nursing teamwork. As the AP role develops and becomes more established it will be possible to investigate these important issues and to study the cost effectiveness of these roles in future studies.
Footnotes
Acknowledgements
We would like to acknowledge the acute trusts which hosted the case studies and the study participants. We acknowledge the contribution of Lucy Stuttard and Gunilla Borglin to data collection and thank the following colleagues: Carl Thompson, Sandi Newby, Michael West, Keith Hurst, Sue Cooper and Alan Maynard. We also thank our research advisory group for their invaluable guidance and support. This paper presents findings from research commissioned by the NIHR Serivce Delivery and Organisation (SDO) Programme. The views expressed are those of the authors and not necessarily those of the NHS, the NIHR or the Department of Health. The NIHR SDO programme is funded by the Department of Health.