
Abstract
Objective
The World Health Organization (WHO) recommends shifting tasks from physicians to lower cadres for the delivery of antiretroviral treatment (ART) for countries short of physicians. Our objective was to evaluate the effectiveness and acceptability of ART delivery by health officers and nurses in Ethiopia.
Methods
A retrospective cohort study to evaluate outcomes of ART services in 25 health centresstaffed with health officers and/or nurses and 30 hospitals staffed with physicians in 2009. Median CD4-cell counts, mortality, loss to follow-up and retention were the primary outcomes. Interviews and focus group discussions were conducted with people living with HIV/AIDS, AIDS programme managers and health care providers to identify the types and acceptability of the tasks conducted by the health officers, nurses and community health workers.
Results
Health officers and nurses were providing ART, including ART prescription, for non-severe cases. The management of severe cases was exclusively the task of physicians. Community health workers were involved in adherence counselling and defaulter tracing. The baseline median CD4-cell counts per micro-liter of blood were 117 (interquartiles [IQ] 64,188) and 119 (IQ 67,190) at health centres and hospitals respectively. After 24 months on ART, the median CD4-cell counts per micro-literof blood increased to 321 (IQ 242, 414) and 301 (IQ 217, 411) at health centres and hospitals respectively. Retention in care was higher in health centres (76%, 95% confidence interval [CI] [73%-79%]) than hospitals (67%, 95% CI [66%-68%]). This difference is mainly due to the higher loss to follow-up rate in hospitals (25% versus 13%). Mortality was higher in health centres than hospitals (11% versus 8%), but the difference is not statistically significant. Service delivery by non-physicians was accepted by patients, health care providers and programme managers. However, the absence of a regulatory framework for task shifting, the lack of extra remuneration for the additional roles assumed by nurses and health officers, and the high cost for training and mentorship were identified as weaknesses.
Conclusion
ART delivery in health centres, based on health officers and nurses is feasible, effective and acceptable in Ethiopia. However, issues related to regulation, remuneration and cost need to be addressed for the sustainable implementation of these delivery models.
Introduction
Many countries have made significant progress towards the goal of universal access to antiretroviral treatment (ART). 1 However, major barriers must still be overcome if universal access is to be realized. 2 One of the major barriers, particularly in sub-Saharan Africa, has been a shortage of staff.3–6 Conventional ART delivery by physicians is recognized as an impediment to the rollout of ART in resource constrained settings.7,8 It is, therefore, recommended that alternative delivery models based on the public health approach with a redistribution of tasks among available staff are used to reduce dependence on physicians and expand the health workforce.7–11
The WHO launched the ‘treat, train and retain initiative’ with task shifting as a strategy to increase the pool of staff who can provide ART services.12,13 This initiative is based on reviews of the experience with alternative models of health services in low-income countries.14,15 The use of mid-and low-level cadres as substitutes for physicians improves access to and sustainability of health services in rural and peri-urban communities.14,15
Many countries have been using new delivery models for delivering ART since the guidelines and recommendations for task shifting was launched in 2008 13 and are able to expand access to ART services.1,9,10 The few studies which had evaluated the acceptability and effectiveness of these new delivery models were based on a small number of health facilities and patients.16,17 Hence, there is a need to evaluate the acceptability and effectiveness of new ART delivery models at a national level.
Our aim was to evaluate health officers' (HOs) and nurses' delivery of ART in Ethiopia which started in 2006. 18 We hypothesized that outcomes of ART services in health centres (based on HOs and nurses) would be the same as outcomes in hospitals (based on physicians), and that service delivery by HOs, nurses and community health workers (CHWs) would be acceptable.
Methods
A retrospective cohort study was conducted in 2009 based on 30 hospitals and 25 health centres providing ART for more than 200 patients. A list of facilities that were providing ART services was used as a sampling frame from which at least 15% of the health facilities in each region of the country were selected, including large (more than 1000 patients on ART), medium (500–1000 patients on ART) and small (200–500 patients on ART) facilities.
A database of ART patients was introduced in September 2006. Data were collected from routine patient registries, a hybrid of electronic and paper based patient management system, for mortality, loss to follow-up and retention. The study included patients who started ART in the 55 health facilities between September 2006 and August 2008. The study period ended in March 2009 so that the minimum follow-up period was six months and the maximum was 24 months. Mortality, loss to follow-up, retention and median CD4-cell counts were primary outcomes, and were determined at six, 12 and 24 months after starting ART.
A Ministry of Health study, conducted in 2007–08, estimated that 37% of hospital patients and 53% of health centre patients reported lost to follow-up, after 24 months on ART, had died. 19 We used these findings to adjust and estimate the mortality of patients reported as lost to follow-up after 24 months of ART in this study.
We also analysed the trend in median (and interquartile range [IQR]) of CD4-cell counts for patients. Samples of 150 and 200 patient charts at each health centre and hospital, respectively, were selected randomly. CD4-cell counts at baseline, six, 12 and 24 months of treatment were identified for each patient.
A qualitative study using semi-structured interviews and focus group discussions was conducted. Semi-structured interviews were conducted in 2009 and early 2010 in all 55 health facilities to identify the role of HOs, nurses and CHWs for ART delivery. The questionnaire was completed by the head of the HIV clinic.
Exit interviews were also conducted with up to 30 patients on ART in each of the 55 health facilities to assess their satisfaction with the service they received. A semi-structured questionnaire in local language was developed and used as an interview-guide after pretesting in two health centres and one hospital in Addis Ababa, Ethiopia. Patients were randomly selected for interview until no new relevant information was being obtained. The interview was conducted by a physician from the FHAPCO. All study participants voluntarily gave informed consent.
Eight focus groups including a total of 57 patients on ART (seven groups with seven patients, one group with eight patients), were held to assess their attitude towards the services provided by HOs, nurses and CHWs. We also had one focus group with 11 programme managers and another with 10 health care providers on the new ART delivery model. Participants were selected on the basis that they were thought to have the potential to provide rich, relevant and diverse information pertinent to task shifting and ART delivery. A topic list was developed on the basis of the experience of the researchers in the field of ART delivery. The focus groups met for an average of two hours in the FHAPCO's meeting hall. The discussions were only partially audio-recorded (because of a problem with the tape recorder) after consent was received from the participants.
All the focus groups were led by an experienced moderator (YA), and attended by an observer who took notes on the discussions. Thematic analysis of the field notes and transcripts of the audio-recordings was based on the topic list used during the interviews and focus group discussions.
Results
ART delivery models and its scale-up
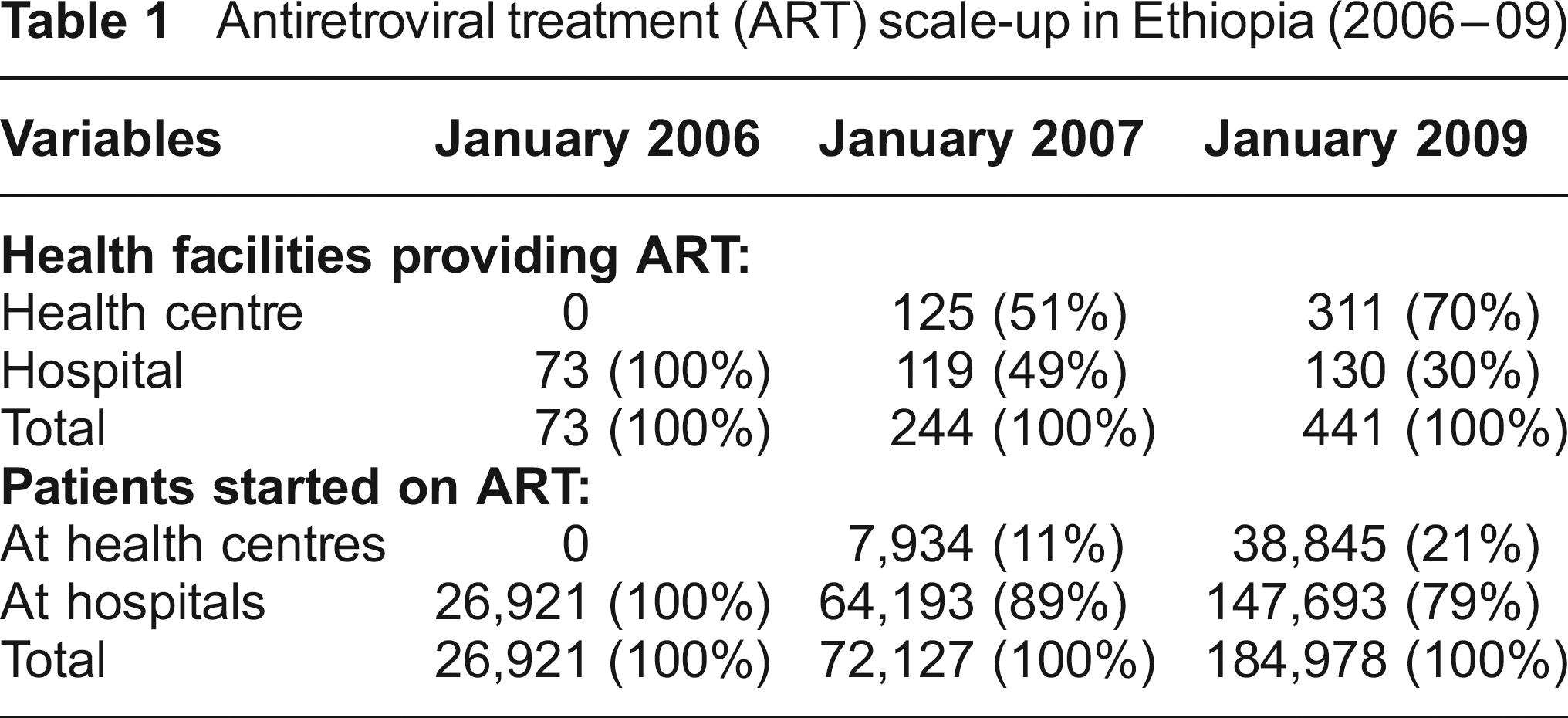
The number of health facilities providing ART and the number of patients receiving ART increased between 2006 and 2009 (Table 1). The ART delivery model in health centres was based on HOs and nurses who were responsible for the delivery of ART-related tasks. Severe cases and treatment failures were managed at hospitals by physicians: HOs and nurses in health centres referred patients with severe manifestations to physicians at hospitals level. CHWs performed tasks such as adherence counselling, referral and linkage between health facilities and care and support institutions, and defaulter tracing (Table 2).
Antiretroviral treatment (ART) scale-up in Ethiopia (2006-09)
Antiretroviral treatment (ART) related tasks performed by different staff in Ethiopia (2009-10)
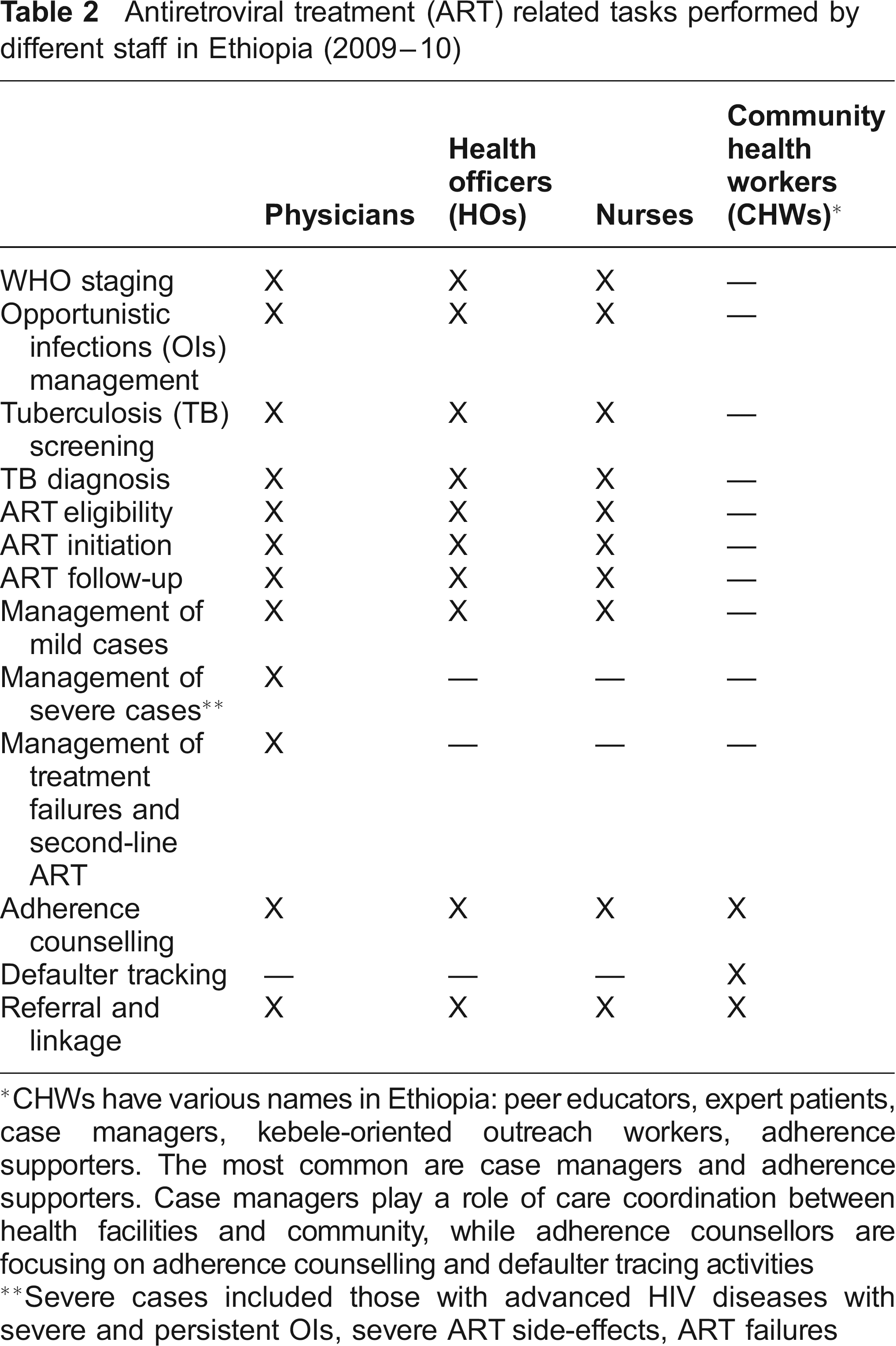
CHWs have various names in Ethiopia: peer educators, expert patients, case managers, kebele-oriented outreach workers, adherence supporters. The most common are case managers and adherence supporters. Case managers play a role of care coordination between health facilities and community while adherence counsellors are focusing on adherence counselling and defaulter tracing activities
Severe cases included those with advanced HIV diseases with severe and persistent Ols, severe ART side-effects, ART failures
ART outcomes at health centres and hospitals
Table 3 indicates that retention in care was similar at health centres and hospitals after six months on ART (82% v 75%), and after 12 months (79% v 74%), but was significantly higher after 24 months on ART (76% v 67%). This was mainly due to the difference in loss to follow-up (13% at health centres, 25% at hospitals).
Outcomes of cohorts of patients treated at health centres and hospitals in Ethiopia (2009)
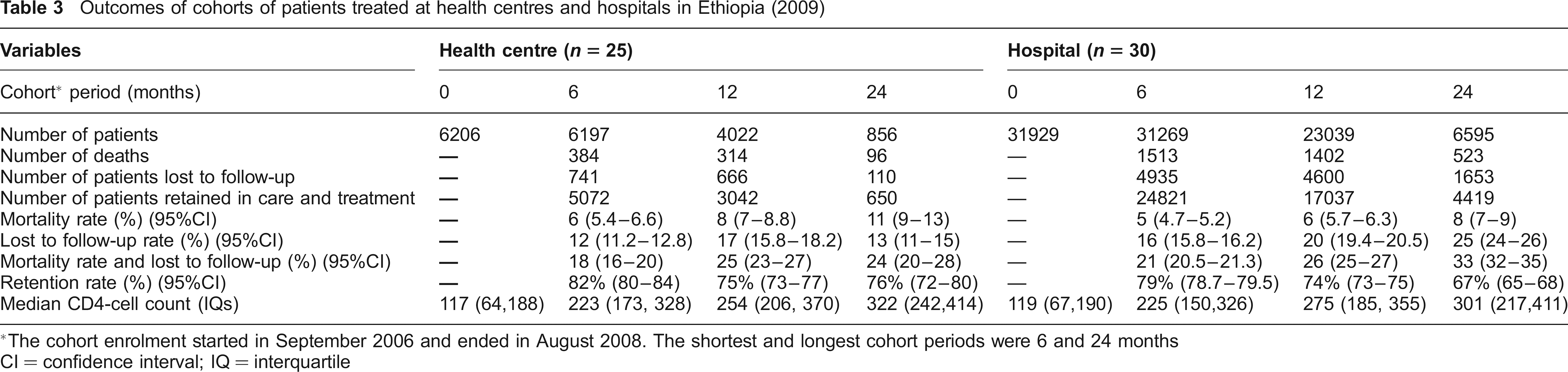
The cohort enrolment started in September 2006 and ended in August 2008. The shortest and longest cohort periods were 6 and 24 months
CI = confidence interval; IQ = interquartile
Mortality was higher at health centres (11%) than at hospitals (8%), but this difference is not statistically significant. When we adjusted for the loss to follow-up based on the findings from a previous study conducted in Ethiopia, loss to follow-up and mortality were estimated to be 16% and 18% at hospitals, and 6% and 18% at health centres.
The proportions of patients in whom CD4-cell counts were documented were similar at health centres and hospitals: 89%, 54%, 51% and 51% of patients at baseline and after 6, 12 and 24 months on ART. The median CD4-cell counts among patients at health centres and hospitals were similar at all time points.
Attitude of stakeholders towards new ART delivery models
Focus group discussions with patients elucidated that nurse and HO services were generally well-accepted, and that it had reduced the waiting time. Patients revealed that they were more comfortable with nurses than with physicians because nurses were friendlier and more supportive. They emphasized that HOs and nurses spent more time with them discussing their medical problems and took sufficient time examining them.
Patients identified three additional benefits of being involved in ART delivery: their life experience helped them provide appropriate counselling; it helped combat stigma and discrimination in society; and it provided them with an opportunity for employment.
Focus groups with AIDS programme managers and health care providers indicated that the new ART delivery model was unanimously accepted as a timely solution in the Ethiopian context. They also indicated that HOs, nurses and CHWs can provide high quality services if they are well trained, mentored and supervised regularly. One of the programme managers said: ‘it wouldn't have been possible to increase access to ART without the engagement of HOs and nurses in ART-related service delivery'. A hospital physician said: ‘HOs and nurses are able to stage patients based on the WHO criteria and initiate them on ART accordingly’. He added that task shifting is the right choice at the right time when there are a lot of patients waiting for treatment while the treatment is available free of charge.
Enablers and barriers to the new ART delivery models
Four enabling conditions were identified by the programme managers, for the smooth implementation of the new ART delivery models: the relatively high number of nurses in the country; the adoption of the public health approach to ART scale-up by the National AIDS Program; the large scale training of nurses and HOs on ART by the National AIDS Program and partners like PEPFAR and WHO; and the mentorship both in hospitals and health centres.
They highlighted that there are many more nurses than physicians in the country providing an opportunity if nurses are trained properly. They added that the public health approach had been beneficial and training and mentorship had facilitated task-shifting and ART scale-up. Mentorship had been organized in such a way that hospital physicians visit health centres for consultations on a regular basis to check how nurses and HOs are performing their task, and also to provide support for difficult cases. HOs with two years experience of managing patients are also providing mentorship to nurses in other health centres. Nurses and HOs can also solicit support from physicians by phone.
Five barriers were also highlighted. First, a lack of a regulatory framework with no legislation that allows nurses to perform certain tasks such as ART prescription. Second, nurses complained that they were not remunerated for the additional clinical tasks they were performing. Third, CHWs were either voluntary workers or contract workers but none were permanent employees in the formal health system. Fourth, the high cost associated with training and mentorship was a concern. Fifth, and most importantly, all respondents expressed their concern that the workload of ART, both in training and service delivery, had diverted many staff away from the general health services.
Discussion
Main findings
After 24 months on ART, retention of patients in care is significantly higher at health centres than at hospitals, and the difference was mainly due to the higher loss to follow-up at hospitals. Median CD4-cell counts at health centres and hospitals are similar. Service delivery by HOs, nurses and CHWs is accepted by patients, service providers and programme managers.
ART programmes in many countries have already begun reassigning tasks to low- and mid-level health workers to overcome the shortage of physicians. This includes the involvement of nurses in the evaluation of patients eligibility for ART, ART prescription for uncomplicated cases and trained CHWs including patients, providing adherence counselling.20,21 Task-shifting in Ethiopia concurs with the experiences of other countries which have instituted delegation of ART-related tasks.14,22,23
The quality of care delivered by mid-and low-level health workers has long been a contentious issue. Our study showed that patient outcomes in terms of mortality were comparable with physicians' care after 24 months on ART. Patients at health centres and hospitals had similar baseline median CD4-cell counts. Moreover, the loss to follow-up rate was significantly lower at health centres (13%) than at hospitals (25%). As a result, overall retention was better at health centres (76% versus 67%). Similar results were reported from other sub-Saharan African countries where patient outcomes were similar in sites with and without physicians.17,24–26
Patients on ART welcomed services provided by nurses and HOs with some patients preferring them to physicians. Similarly, reports in South Africa show that nurse-led ART care models were feasible and acceptable to patients. 27 Reports from countries such as the USA, the UK and Australia indicate that the quality of care and patients' satisfaction are similar in nurse- and physician-based services. 28 As a result, there is a growing interest in the use of physician assistants and nurse practitioners in these high-income countries. 29
Strengths and limitations
Our study has several strengths and weaknesses. On the positive side, it included many health facilities and patients on ART and used both processes and outcomes to evaluate the acceptability and effectiveness of task-shifting. The study was based on data from a programme setting; hence, it is likely to reflect the reality on the ground. The study also analysed both the enabling conditions and gaps that might affect the sustainable implementation of the new ART delivery models in Ethiopia.
The study has three limitations. First, the facilities were not selected randomly but on the basis of number of patients receiving treatment in the facility and regional representation. However, all regions of the country were represented, the facilities included in the study were composed of large, medium and small hospitals and health centres, and the majority of patients started on ART were getting services from these health facilities. Hence, the findings from this study can be generalized to other facilities in the country. The second limitation is that we did not investigate the outcome of patients who were lost to follow-up, but instead used the findings from a previous study to adjust our results. We believe that the findings from the previous nationwide study can be applied to our current study as it is a big nationwide study that represents all health facilities providing ART in the country. The third limitation is that the CD4-cell counts were not documented for all patients and those without CD4-cell counts might have differed in terms of baseline characteristics and outcomes.
Implications
This study has indicated that ART delivery in health centres, based on HOs and nurses, is effective and acceptable in Ethiopia. It is important that the country capitalizes on the enabling conditions and addresses the weaknesses, such as lack of appropriate regulatory mechanism, inadequate financial incentives and career structure for low- and mid-level health workers, and the need for training and mentorship.
We recommend the following for future research: a cost-effectiveness analysis of ART delivery models with different degrees of task-shifting, including drug dispensing by CHWs; and the effect of ART training and services on general health services. New ART delivery models should not be viewed as a panacea but as a part of an overall comprehensive strategy that includes the production, deployment and retention of health workers.
Footnotes
Acknowledgement
The study was made possible thanks to a grant from the framework agreement between the Belgian Directorate General for Development Cooperation and the Institute of Tropical Medicine, Antwerp, Belgium.