
Abstract
Objectives
To determine the extent to which primary care trusts (PCTs) in England employed processes associated with quality commissioning and to assess whether changes occurred in these processes during a policy drive to improve commissioning.
Methods
Telephone surveys of PCT managers leading commissioning for diabetes, chronic obstructive pulmonary disease (COPD), coronary heart disease (CHD), and emergency and urgent care in all 152 PCTs in both 2009 and 2010.
Results
The response rate was 51% (77/152) of PCTs in 2009 and 60% (91/152) in 2010. Two-thirds of commissioners had commissioned initiatives starting in the previous financial year. Over half of initiatives starting in 2008/09 had been instigated by the PCT alone. This reduced to a third in 2010, showing a shift towards partnership working. Commissioners reported that a large proportion of initiatives had been developed and shaped with the involvement of general practitioners (GPs) with direct links to the PCT and of specialist clinicians (70%), but that a lower proportion of initiatives had involvement from other GPs (40%). Patients or the public were less likely to be involved in initiatives than clinicians, but there was evidence of increasing involvement over the two years from 35% (52/149) to 51% (67/132) of initiatives. There was no evidence of changes in whether needs assessment was undertaken, how evidence was used or how initiatives were led and performance managed.
Conclusions
PCT commissioners reported clinical engagement in the majority of commissioning initiatives, a shift towards partnership commissioning, and increased involvement of patients and public in the development of initiatives. The new model of commissioning in England through clinical commissioning groups will need to improve on these processes if it is to demonstrate a higher quality approach to commissioning.
Background
There has been increasing interest in the commissioning of health care internationally as different countries reform the role of commissioning or the relationship between commissioners and providers. 1 Approaches to commissioning vary in terms of the types of organizations that commission, and their funding sources. In addition, terms used to describe commissioning vary by country and include ‘purchasing’ and ‘managed care’. Despite these differences, evidence relating to commissioning models in one country can inform health care management or structural changes in another. Policy-makers in England have introduced a number of new models of commissioning in health care in recent years as well as promoting improvements to existing models.
Commissioning in the National Health Service (NHS) in England has been defined as ‘the process of specifying, securing and monitoring services to meet individuals’ needs at a strategic level'. 2 The introduction of the internal market in the early 1990s led to the separation of commissioning from the provision of health care in common with other countries with similar models of health care. 1 Since then, NHS commissioning has undergone a series of reforms, including the introduction of general practitioner (GP) fundholding and total purchasing. 3 Since 1997, commissioning budgets have been largely held by primary care trusts (PCTs) (formerly health authorities then primary care groups) which work on behalf of their local populations. In 2004, an increased role in commissioning for GPs was advocated through the introduction of practice-based commissioning (PBC). The aim was to encourage general practices and other front line primary care professionals to become more engaged in the commissioning of health services. 4 Practices were given ‘indicative budgets’ to commission services for their patients and expected to redesign services to provide better experiences for patients and improve efficiency. 5 The latest policy plans to move the commissioning function from PCTs to clinical commissioning groups involving general practitioners and other health professionals running alongside a national commissioning board, with an enhanced role for local government and greater emphasis on patient choice and competition. 6
In recent years the quality of commissioning in England has been scrutinized. In 2006, the Department of Health set out a framework to strengthen commissioning in order to drive health reform, improve health, improve health care and improve the financial health of the NHS. 7 This was initially developed through ‘World Class Commissioning’ which was a statement of intent designed to improve commissioning capability and enable commissioners to demonstrate better outcomes. 8 This was formalized in 2007 as a set of ten organizational competencies that included clinician and patient engagement, collaborative working with community partners, needs assessment and performance management, and prioritizing investment, 9 with an additional competency relating to efficiency and effectiveness of spend added in 2008. PCTs were assessed against these competencies in 2009 and 2010 with the expectation that the quality of commissioning would improve between these two time periods. This policy aimed to change the focus of PCT commissioners from passive contractors of services to proactive commissioners in order to secure the best quality and value care for their populations whilst improving population health outcomes. 10
Defining and measuring the quality of commissioning is important if we are to see whether commissioning quality improves over time. However, there is no accepted definition of quality commissioning. In England, World Class Commissioning was introduced in response to concerns about the low quality of commissioning and therefore could be considered to encapsulate some aspects of quality commissioning, This is supported by the views that these competencies are likely to be the foundations for the next model of commissioning.11,12 Other aspects of quality are evident in evaluations of commissioning models both within the NHS and worldwide that have identified processes of commissioning associated with desired outcomes.1,3,13
The aim of our repeated cross sectional survey study was to determine the extent to which PCTs in England employed processes associated with quality commissioning and to assess whether changes occurred in these processes during a policy drive to improve commissioning.
Methods
Recruitment
We undertook a telephone survey of commissioning managers in all 152 PCTs in England in 2009 and again in 2010. We focused on four commissioning areas: diabetes, coronary heart disease (CHD), chronic obstructive pulmonary disease (COPD) and emergency and urgent care. The long-term conditions were selected because practice-based commissioners were known to be actively commissioning in these areas. Emergency and urgent care was selected in order to include the commissioning of services as well as for health conditions. We invited PCTs to participate and asked the chief executive or director of commissioning in each PCT to identify the commissioning manager with responsibility for each of the four chosen areas. We undertook up to four telephone interviews in each participating PCT in 2009 and again in 2010. In 2010, we approached those PCTs that had declined to participate in the 2009 survey and obtained additional participants. The two sets of telephone interviews were undertaken between April and October 2009 and between April and August 2010.
Questionnaire development
We defined a set of commissioning processes associated with quality and relevant to the commissioning of individual initiatives. These were based on a subset of the World Class Commissioning competencies 9 and processes shown to be important in previous commissioning models. 3 The key processes grouped into the following five domains: clinical engagement, 9 public and patient involvement, 9 evidence and needs assessment, 9 leadership and management,9,3 and a focus on outcomes. 9 The questions we asked are detailed within Tables 3–6 below.
Data collection
For each of our four areas of interest we used a structured questionnaire to obtain information about proactive changes made by commissioners in the previous financial year. We recognized that commissioners undertook many functions including implementing national policies, reacting to problems occurring in their locality and maintaining service provision. However we were interested in their commissioning initiatives: the planned changes they had made to local health care provision. We asked commissioners to identify the largest initiative that had been commissioned by the PCT (that is, investment of new money or reconfiguration or disinvestment of services) and that had started in the previous financial year (2008/09 and 2009/10 respectively). In the 2009 survey we also asked if a larger initiative had occurred in the previous three-year period because we were keen to identify the largest initiatives for a related wider study.
Commissioners were then asked to describe the largest initiative, specifically to determine: whether it was a reconfiguration, investment or a disinvestment; the scope of the initiative (e.g. whether it was aimed at all diabetes patients in the PCT or a specific group of patients with diabetes); and details of funding including the total amount of financial resource allocated. The commissioning manager was asked to answer a series of structured questions relating to processes within the five commissioning domains listed above for their largest initiative. Telephone interviews were undertaken by a small team of researchers, with the majority undertaken by one of the authors (FS). Interviews were recorded to ensure that data had been recorded accurately on the questionnaire.
Analysis
We compared characteristics of PCTs that participated versus non-responders with respect to basic demographic characteristics using routine data sources.14–16 We also compared the World Class Commissioning competency scores and ranking according to the world class commissioning assurance exercise. 17
We describe the proportion of commissioners reporting the use of each of the processes defined above for their largest commissioning initiative starting in 2008/09 and in 2009/10. A comparison of processes between the two time points would potentially be invalidated due to changes in those PCTs who responded at each point. Therefore we restricted our change over time comparisons to the group of PCTs for which we had data at both time points and that had an initiative to report in both years. We compared proportions of commissioners reporting adherence to processes using McNemar's test for paired data. 18
Ethics
The research was classed as a service evaluation by South Humber Local Research Ethics Committee. We obtained ethical approval for the study from the University of Sheffield.
Results
Response rates
Fifty-one percent (77/152) of PCTs agreed to participate in the survey in 2009 and a further 14 PCTs agreed to participate in 2010 (60%, 91/152). We compared the characteristics of respondents with non-respondents in 2010 (Table 1). Non-respondents were ranked lower in the World Class Commissioning assurance exercise and were less financially healthy, but otherwise were comparable.
Comparison of respondents and non-respondents for the 2010 survey
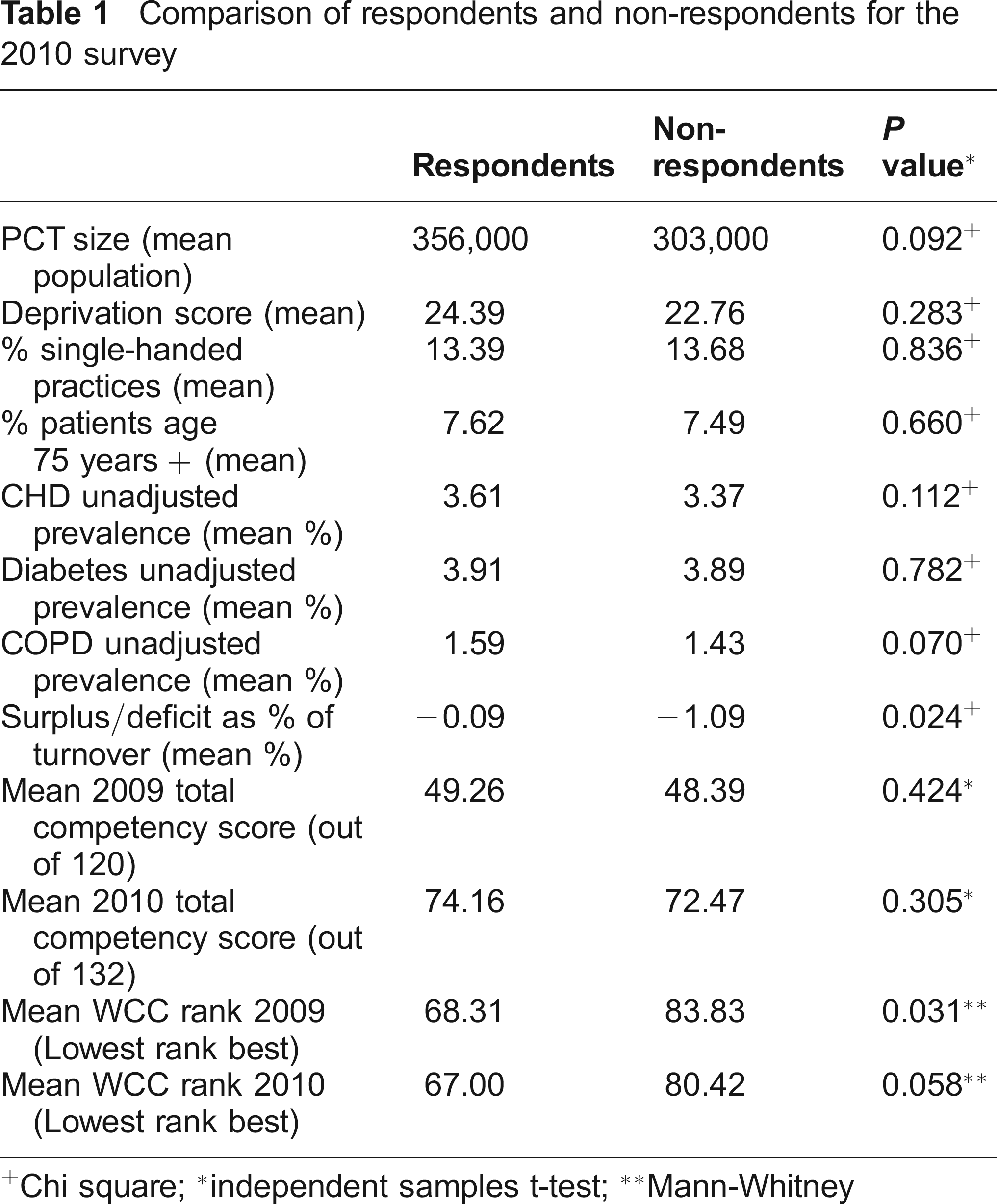
Chi square;
independent samples t-test;
Mann-Whitney
We interviewed up to four commissioners in each PCT: diabetes (n = 74 and n = 72), CHD (n = 65 and n = 67), COPD (n = 71 and n = 64) and emergency and urgent care (n = 67 and n = 66). In total we undertook 277 interviews in 2009 and 269 in 2010, although some interviewees in 2010 who had not participated in 2009 described an initiative which began in 2008/09 rather than 2009/10 because this had been their largest initiative. Figure 1 shows the numbers interviewed in each year and the total number of initiatives for which we had information.

Recruitment and response details
Cost, size and type of initiatives
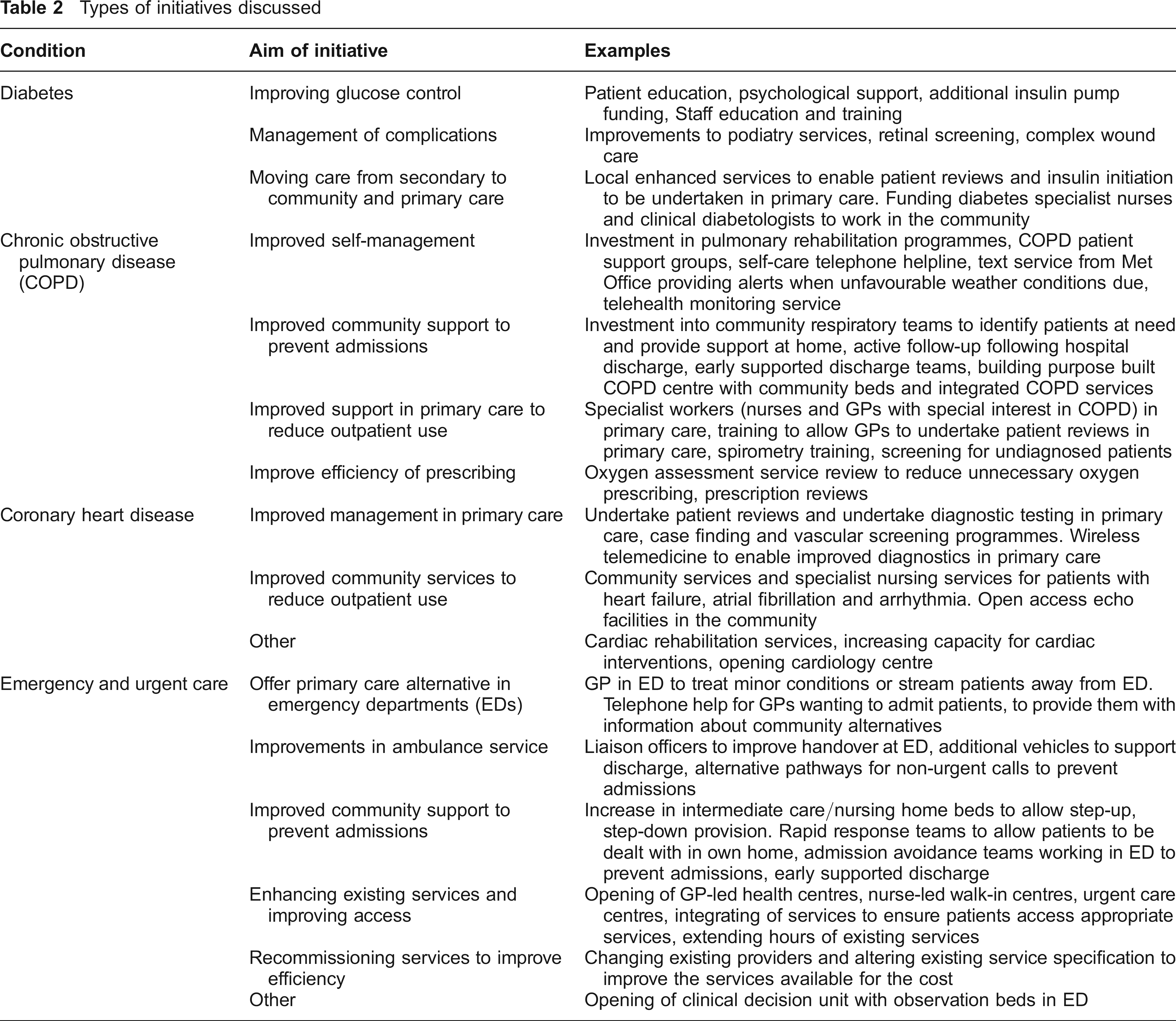
Around two thirds of managers reported that the PCT had commissioned initiatives that started within 2008/ 09 or 2009/10 (191/305, 63% v 140/241, 58% respectively). Of the 191 commissioners who said that an initiative had started in 2008/09, 34 went on to give details of a larger initiative that had been commissioned within the two years prior to that and were thus excluded from this analysis (Figure 1). Only 68 commissioners in the same area in the same PCT started an initiative in both years and could be included in the paired analysis. Commissioners described a wide range of initiatives (see Table 2), with the costs ranging from £2,000 to £7.2 million (mean £391k, median £204k 2008/09; mean £362k, median £133k 2009/10). In 2008/09, two PCTs reported zero cost service reconfigurations and no disinvestments were reported. In 2009/10 there were 12 zero cost initiatives and two disinvestments.
Types of initiatives discussed
Clinical engagement
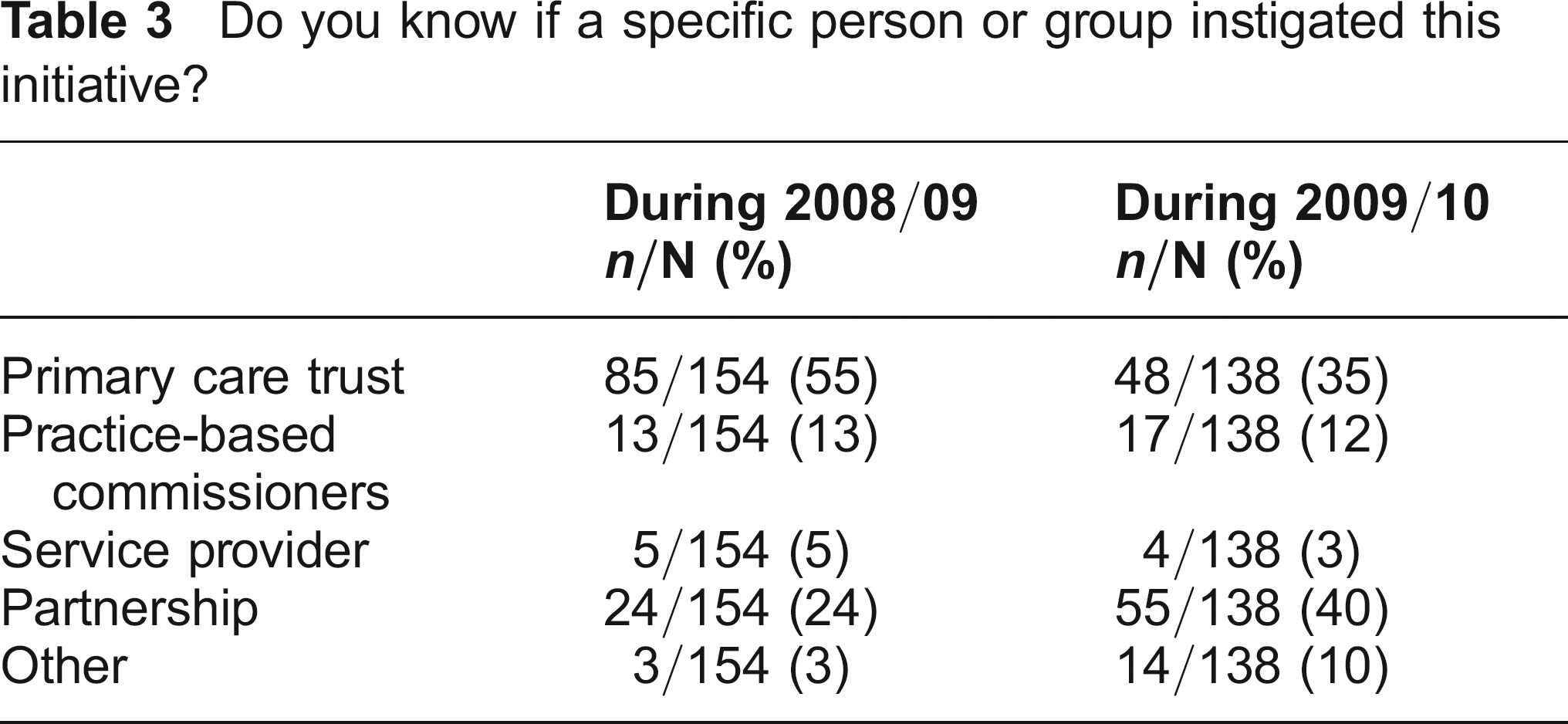
Over half of all initiatives commissioned to start in 2008/ 09 were reported as instigated by the PCT alone (Table 3). However there appeared to be a considerable shift the following year to initiatives instigated by some combination of PCT, practice-based commissioners, service providers or other groups such as cardiac networks. This shift to partnership commissioning was statistically significant in the paired analysis (10/68 v 28/68, P = 0.001). Practice-based commissioners instigated initiatives either alone or as part of a group in 18% of initiatives (28/154) in 2008/09 versus 29% (40/138) in 2009/10. However, this increase was not statistically significant in the paired analysis (15/68 v 19/68, P = 0.481).
Do you know if a specific person or group instigated this initiative?
We asked respondents to describe who had been involved in developing and shaping the initiative (Table 4). The majority of the initiatives were reported as having a variety of clinicans fully or largely involved. These reported proportions were similar for both years and the paired analysis showed no difference in the level of involvement of specialist clinicians, GPs or practice-based commissioners between the two years. In around 80% of initiatives GPs usually involved in the PCT, other GPs or practice-based commissioners had been fully or largely involved in both years (125/157, 82% in 2008/09, 103/131, 79% in 2009/10).
To what extent were any of the following groups involved in developing and shaping the initiative?
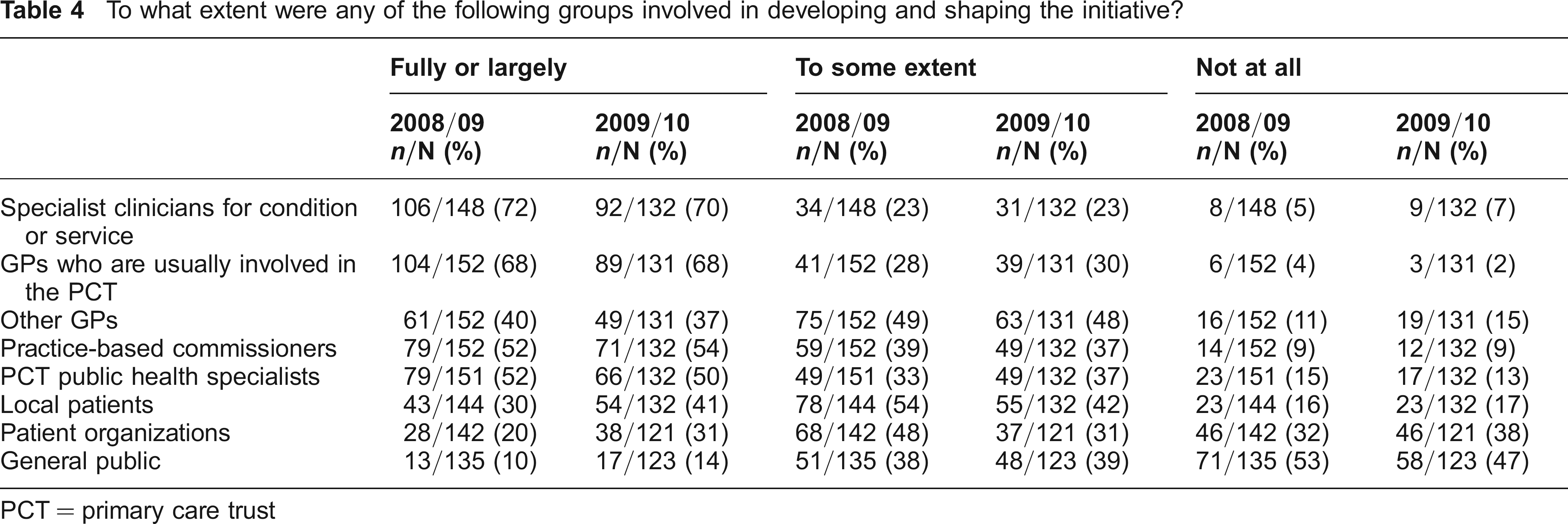
PCT = primary care trust
Public and patient involvement
The reported levels of public and patient involvement in the developing and shaping of initiatives were considerably lower than for clinicians (Table 4). There was evidence of an increase in involvement over the two years, with patient or public involvement of any sort (local patients, organizations or general public) increasing from 35% (52/149) to 51% (67/132) of initiatives. This was a statistically signicant change within the paired analysis (21/65 v 33/65, P = 0.043).
Evidence and needs assessment
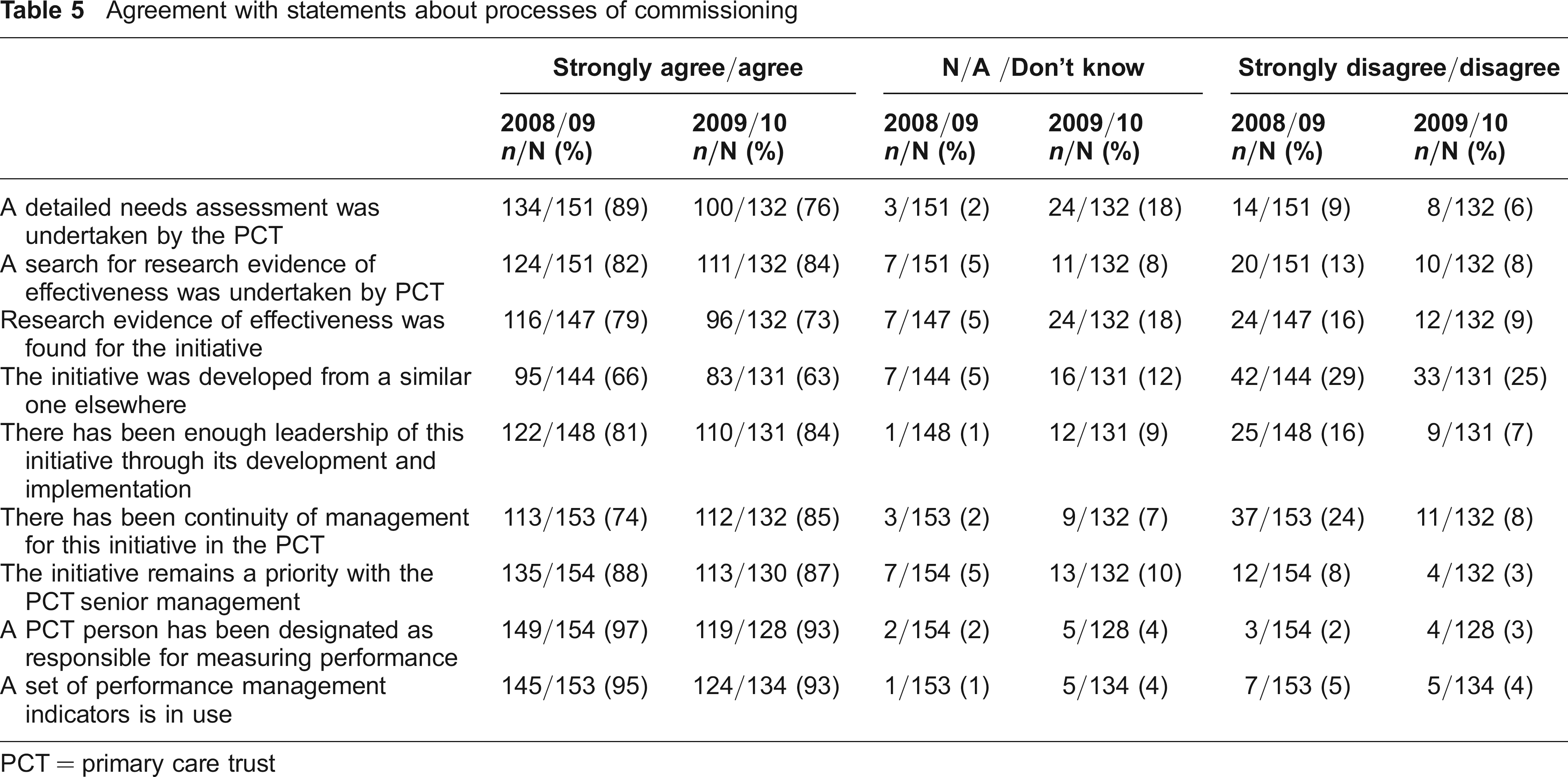
We asked commissioners to rate their agreement with a series of statements about the processes of commissioning used for the initiative, using a five point Likert scale (see Table 5). We grouped responses into strongly agree/agree, not applicable/don't know and disagree/ strongly disagree for ease of reporting. Four fifths of initiatives were reported to have been based on research evidence and there was no indication that this changed over time.
Agreement with statements about processes of commissioning
PCT = primary care trust
Leadership and management
There was a high level of agreement with most of the statements around leadership and management. In particular, the existence of a specified person responsible for performance management, and the use of performance management indicators, were almost universal. There were no statistically significant differences between the two years.
Commissioning for outcomes
Given the recent focus on commissioning for outcomes, we asked commissioners what outcomes they expected to obtain from the initiative, when they expected to obtain them and the size of change anticipated. We provided a list of outcomes and asked them to specify which were primary or secondary outcomes of the initiative. The most commonly reported expected outcome was a reduction in emergency admissions (Table 6). Few commissioners were able to report on the size of change anticipated specifically for these outcome measures, although there was an increase in the proportion of commissioners who were able to quantify the expected reduction in emergency hospital admissions between the two years (paired analysis 4/15 v 11/15, P = 0.039).
Expected outcomes for each initiative (five most commonly reported)

Discussion
The study suggests that PCTs commonly used some processes associated with quality commissioning. For most of their large initiatives they reported that performance management was in place, that there was continuity of leadership and that needs assessment had been undertaken. They performed less well on clinical involvement but still reported that some type of clinician had been involved in the development and shaping of the majority of their largest commissioned initiatives. However, in a fifth of cases the commissioner reported that there had been little or no involvement of GPs. They were considerably less likely to have reported that there was patient and public involvement, although this appeared to have increased over the time period of the two surveys. There was also a shift from PCT instigation of initatives towards partnership instigation of initiatives and an increase in the ability of commissioning managers to quantify some of the primary outcomes expected from initiatives.
The Department of Health undertook its own assessment of PCT commissioning with the World Class Commissioning assurance exercise. This exercise indicated that PCTs had improved on a number of commissioning competencies between 2008/09 and 2009/10, including public and patient engagement and collaborating with clinicians.19,20 We found no evidence of an increase in involvement of clinicians in developing and shaping initiatives but did find an increase in the proportion of commissioners reporting involvement of patients or public in new initiatives. This is an encouraging finding given that lack of progress on this front has been highlighted previously. 21 The increase in involvement over the two years studied suggests that the policy drive may have provided the impetus required to increase patient and public involvement in commissioning. The reported increase in partnership commissioning is reassuring given that collaboration between different clinical groups and organizations is seen as key to making a success of NHS reforms. 22
More recently there has been considerable emphasis on the need for commissioners to understand and demonstrate benefits by measuring outcomes. 13 We found that commissioners were clear about the types of outcomes they expected but often could not quantify the changes they hoped to achieve. With outcomes that were specific and measurable (e.g. reduction in emergency hospital admissions or outpatient visits) commissioners were more likely to be able to quantify the outcome and there was an increase in the proportion of commissioners who could report the size of change they hoped to achieve in 2009/10 for the key outcome of reducing emergency hospital admissions, suggesting that the drive to consider outcomes in the commissioning process may have had some effect.
Given that under current proposals for NHS reform clinical commissioning groups will be responsible for the vast majority of NHS commissioning, it is a concern that our surveys showed limited involvement of practice-based commissioners in PCT commissioning, even though we focused largely on long-term conditions which these new types of commissioners were supposed to be more involved with. This is in line with other research on PBC which shows that it has not brought about the widespread change in clinical engagement that was initially envisaged.23,24 Perhaps what is more encouraging in our study is that practice-based commissioners were reported as responsible for initiating initiatives, either alone or in partnership with other groups in 18% of initiatives in 2008/09, rising to 29% in 2009/10. While the vision for clinical commissioning group-led commissioning does not require all GPs to become commissioners, it does require all commissioning to be led by GPs and our findings imply that there is still some distance to travel before GP-led commissioning can become a reality.
Strengths and limitations
This is one of the few studies attempting to quantify commissioning processes, offering a snapshot of recent commissioning processes in PCTs in England. Our quantitative approach complements and provides context for some of the excellent in-depth qualitative research which has recently been completed 5 or in progress.25,26 A strength of this study is the use of a telephone rather than a postal survey. Due to the complexity of the concepts of ‘commissioned initiatives’ we were able to probe and clarify aspects of the initiative that would not have been possible using a written survey. The survey also asked respondents to talk about the commissioning processes related to a specific initiative rather than simply asking for views on commissioning in general. The study does have limitations. We devised our own set of processes associated with quality, and these were limited by the need to be relevant to commissioning individual initiatives. We also relied on commissioners' self reports of processes in a climate in which they were being formally assessed on their commissioning competencies. Their views about the meaning of patients and the public being ‘fully involved’ might differ from the views of a researcher observing commissioners plan changes to health care. However, given that respondents were willing to report a lack of involvement of some important groups in commissioning, and we reassured participants that their answers would be anonymous, we would suggest that this has had only a partial impact.
We also acknowledge the existence of non-response bias. PCTs with low ranking in the World Class Commissioning assurance exercise and larger deficits were under-represented in our sample. Taking this into consideration, alongside the fact that commissioners were asked to describe processes associated with their largest initiative, where PCTs are likely to have made more effort to engage different stakeholders and ensure performance management procedures, indicates that the picture of PCT commissioning presented here may be more positive than in England as a whole.
The concept of ‘quality commissioning’ is difficult to define. A review of health care commissioning in Europe, New Zealand and the USA found no single systems of commissioning to work consistently well but that different models had examples of innovation and good practice. 27 We relied largely on the World Class Commissioning initiative to define processes associated with quality. We believe that this was an appropriate approach because PCTs valued this competency framework as a useful tool for improving the quality of commissioning. 10 World Class Commissioning was presented by national policy-makers as a vision for ‘best practice’ in commissioning. While it was by no means welcomed as the best solution to the problem of improving commissioning, 28 it was probably the most comprehensive framework available for addressing commissioning quality. It is also the case that some of the processes we included have been identified as facilitators for the effective commissioning of health care internationally, such as needs assessment, clinical engagement and patient involvement. 27
Implications
Health care commissioners in PCTs in England reported using processes associated with quality commissioning for the majority of the largest changes they made to health care provision, with the exception of patient and public involvement. While many of the processes we studied did not change over time, the policy drive for improving patient and public involvement appeared to have had some effect. This indicates that the quality of commissioning can be improved through national policy drives. The recent changes to commissioning in England have placed increasing emphasis on clinical engagement and clinical leadership. We found that although clinicians were often involved in developing initiatives instigated by the PCTs, clinicians as practice-based commissioners instigated change in only a minority of cases. This indicates the challenges facing the delivery of a clinician-led commissioning model. Indeed the shift over time we identified was towards a collaborative approach to instigating changes, rather than change led by a single agency or group.
Footnotes
Acknowledgements
We would like to acknowledge the help of Simon Dixon and Jane Carlisle in designing the data collection instruments, Clara Mukuria for helping with telephone interviews and Marc Chattle for data entry. This is an independent report commissioned and funded by the Policy Research Programme in the Department of Health. The views expressed are not necessarily those of the Department.
Conflicts of interests: None declared.