
Abstract
Objectives:
In 2009, one Scottish region launched a smoking cessation programme offering a weekly financial incentive of £12.50 over a 12-week period. However, a significant proportion of registered participants dropped out of the programme, some even failing to collect the financial reward they were owed. We explore reasons for disengagement and failure to re-engage within this group.
Method:
Individuals (n =14) were interviewed in depth. Transcripts from recorded interviews formed the dataset and were analysed using the “Framework” method.
Results:
Incentives appeared to introduce a potential change/reversal in the felt contractual relationship between service provider and client: the client was now the provider and being paid to quit. This led to an increased sense of obligation towards the service, and enhanced feelings of failure, guilt and shame post-relapse, and reluctance to continue engagement or re-engagement. Other service factors promoting disengagement included issues of practical delivery through location, timing, administrative burden and incentive preference.
Conclusion:
The future design of incentive-based schemes should be cognisant of the potential impact on the client-professional relationship. Increasing the value of the incentive may overcome clients’ antipathy towards bureaucracy and monitoring, but may simultaneously exacerbate the sense of failure and resultant stigma associated with relapse. It may be more cost-effective to reduce barriers/costs such as inconvenience, lack of privacy, timing and embarrassment of association of attendance at the pharmacy with methadone use. Alternatively, risks may be managed by reframing weekly rewards as three separate month-long stages, increasing a sense of achievement that a particular stage has been achieved before any relapse.
Introduction
Incentive based schemes are gaining significant attention as a means of promoting behaviour change through extrinsic motivations.1,2 However, such schemes have led to a number of questions with regard to political acceptability, ethical justification and effectiveness. 1 For example, concern has been expressed that the use of incentives contains overtones of “bribery” and “coercion”, as well as being characterised by elements of injustice and inequality.1,3 In addition, questions over their ability to sustain behaviour modification once an incentive is withdrawn have been raised. 2
A central feature around which questions of ethics and effectiveness revolve is the level and form of the incentive.1,4 A reward deemed too high is likely to be met with public calls of inequity, accusations of bribery and challenges to defend publicly, irrespective of overall cost-effectiveness. A reward deemed too low is likely to reduce uptake, long term engagement and thus overall effectiveness.
In 2009 NHS Tayside, in partnership with NHS Health Scotland and the Scottish Government, launched Quit4u, a two year project specifically targeting the 36,000 smokers living in areas of deprivation in Dundee. 5 Smokers living in deprived areas (depcat postal areas 6 and 7 on the Carstairs categorisation 6 ) were eligible to collect £12.50 per week in vouchers over a 12 week period to spend on groceries if they remain abstinent. Confirmation of smoking status was obtained by carbon monoxide breath testing on a weekly basis at a local pharmacy or smoking cessation group meeting.
In order to register with Quit4u, individuals were required to complete documentation for the smoking cessation team, as well as an application for a national entitlement card. Subsequently, a supermarket card was electronically topped-up on confirmation of weekly cessation. However, analysis of registration figures for the Quit4U scheme showed that around 25% of people who registered failed to take part further in the scheme and an additional 10% were recorded as being smoke-free for one week but then ceased involvement. This paper attempts to shed light on the range of reasons why some clients disengage from this initiative and the relation of such behaviour to the central incentive debate.
Methods
The Quit4u intervention is currently the subject of a three-year independent evaluation, being conducted separately by a collaboration between the Scottish Centre for Social Research, the University of Aberdeen and the University of Edinburgh on behalf of NHS Health Scotland. The evaluation involves a comparative quantitative analysis of Scotland-wide and NHS Tayside's smoking cessation rates, a cost effectiveness analysis, longitudinal qualitative research undertaken with Quit4U participants, and interviews with service managers, smoking cessation providers and other health professionals.
Study design
The project explored the nature and range of individuals’ perceptions, beliefs and behaviour rather than frequency. This indicated that a qualitative method was most appropriate. We chose individual in-depth interviews over focus groups to ensure confidentiality and ease of access. Ethical permission was obtained from Tayside & Forth Valley research ethics committee.
Setting and participants
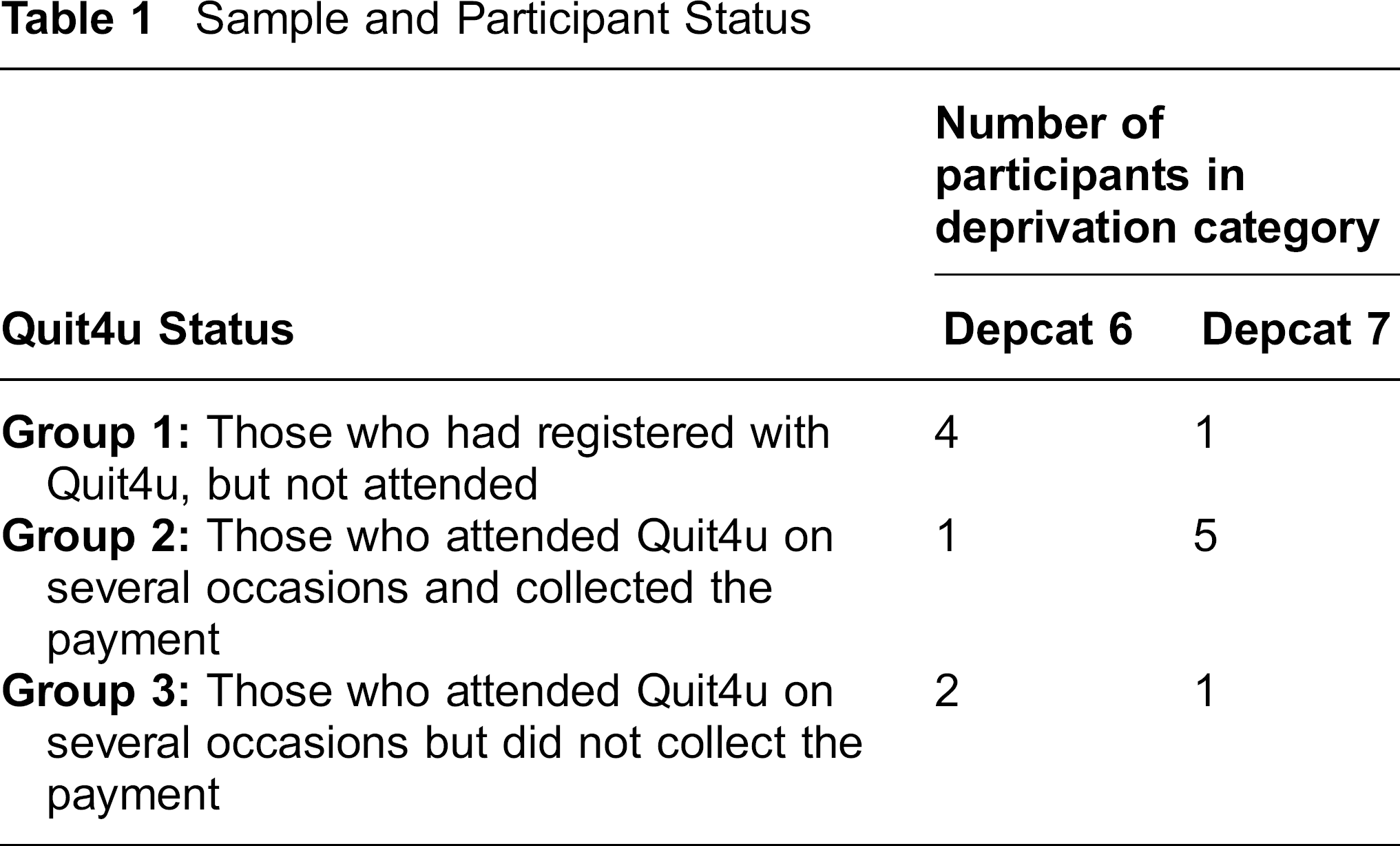
A purposive sampling strategy was adopted in order to enable identification of the range of views and experiences of participants. 7 Candidates who qualified for the study had to be aged over 18, living in a depcat 6 or 7 area, and:
Had registered, but not attended; Had attended on several occasions and collected the payment, or Had attended on several occasions but did not collect the payment.
An established Quit4Udatabase of all those who had registered and their recorded weekly participation was used to identify potential participants. A total of 14 individuals (2 male, 12 female) were recruited and interviewed (see Table 1). All had a smoking history exceeding 10 years. Ages ranged from 27 years to 61 years with a mean age of 44 years. Nine were unemployed, disabled or retired; five were in regular employment. Seven were monitored at 6 different pharmacies, and 7 were monitored at smoking cessations groups.
Sample and Participant Status
Recruitment
Potential participants were contacted by a member of the smoking cessation team and informed of the project. A participant information sheet detailing involvement in the study was sent to those who reacted positively; they were subsequently telephoned by the researcher to arrange the interview. Written consent was obtained on meeting, before the interviews.
Data Collection
Interviews were undertaken in the participants’ own home or at a mutually convenient location. Interviews were unstructured and all were digitally recorded and conducted by a researcher not involved in the programme or employed in the NHS. Participants were assured that all comments would remain anonymous.
Analysis
All interviews were fully transcribed and formed the data set for this project. Transcripts were analysed using the “Framework” method. 8
Results
A range of barriers and impediments to engagement and ongoing participation with Quit4u were reported. The incentive was not sufficient to overcome these issues, particularly if more than one issue was experienced. When examined, a clear hierarchy of psychological, social and practical issues emerged. These appeared to be either attributed internally to the participant or externally to the project (Figure 1).
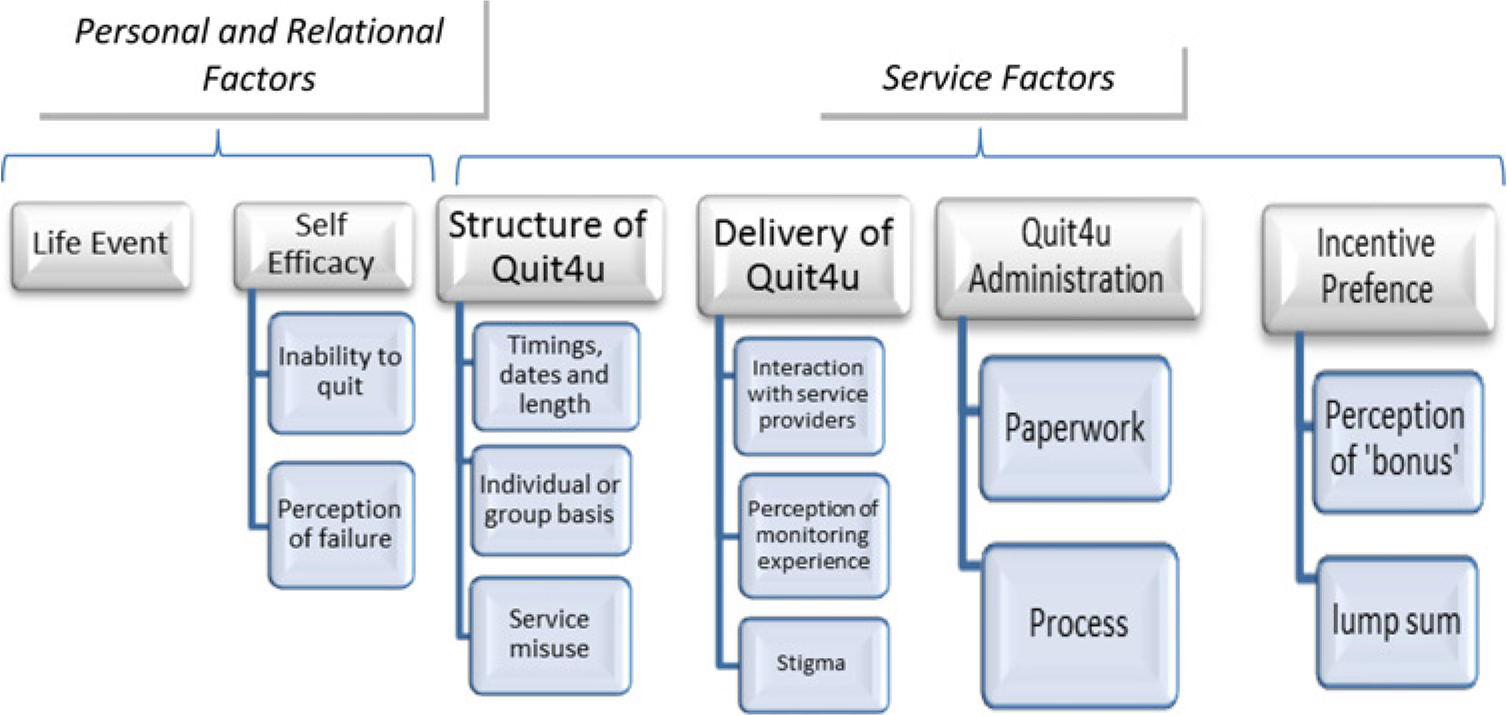
Quit4u barriers
Personal & Relational Factors
Participants reported a number of reasons for disengagement, independent of service organizational issues.
Identity, stigma and the “contractual relationship”
Reasons for disengagement hinted at a felt change in clients’ relationship with service providers, with the incentive introducing a quasi-contractual relationship. This placed the patient in the role of “providing the service” (smoking cessation) and the health care professional as the “buyer”. For some, this relationship manifested itself in a sense of obligation to the service providers, manifest most clearly when they had “failed to deliver”:
“….I just felt I had let them down as well. Even though it is yourself, you still feel as if you are letting other people down as well which again is a horrible feeling so then you feel guilt again and I think, I'm just gonna have a fag.” (female, 35, lab worker, group 3)
The enhanced feeling of guilt, made worse with knowledge of the financial gain and subsequent relapse, led to non-attendance at weekly monitoring sessions. There was concern of reprimand for poor use of the service, embarrassment of confessing their failure and the perceived stigma.
“When we came back I was sort of, I wasn't scared to go back, but I said if I go back I'm going to get a right row for not phoning them or not turning up, eh, that's really the reason why, you know.” (male, 56, council worker, group 2)
Many could not fault the support they subsequently received. However, while this change in relationship was largely reported as “felt” rather than “experienced” there was some evidence to suggest that the act of providing the incentive may sometimes risk shifting staff attitudes from the client-professional status to one of greater dominance and professional as service purchase. This was cited as a reason preventing some from advancing in the Quit4u programme:
“She [the pharmacist] was very patronising……for somebody to sit there and patronise you, it was just not helpful. I cannae quote her but it was like, “right, we're trying to help you, you are just throwing it back in our face.”(female, 61, retired, group 2)
The delivery timing of Quit4u also risked damaging self-identity through another means. In some pharmacies it coincided with the distribution of methadone. Some feared being recognized in a queue associated with drug addicts, particularly in ethnic communities.
“I mean, well, standing in the queue was bad for a start but then the people that are standing along in the queue are not normal. They, the junkies, are totally out of this world I think and emm, some of them just start speaking to you and like you don't even know them. That was one of the things that put me off.” (female, 27, unemployed, group 2)
Six of the seven participants monitored at pharmacy settings reported stigma/shame; compared to only one of the seven people in the smoking cessation group. This provided further supportive evidence that the sense of obligation may be exacerbated predominantly in the context of the pharmacy setting and relationship.
Life events & self-efficacy
Where failure was attributed to unanticipated and unavoidable life events, such as bereavement or divorce, there was a sense in which responsibility for failure and associated shame or guilt was diverted. In these circumstances there appeared a greater likelihood for future re-engagement:
“I went back to smoking, we had a horrible family emergency which kind of threw me back into smoking and what not again. Yeah, I've tried very hard, very, very hard but unfortunately it didn't work. I'm a bit disappointed in myself but I'll try again.” (female, 36, unemployed, group 2)
Service Factors
Participants highlighted a range of perceived and experienced problems with regard to the structure, administration and incentive itself.
Structure
Participants raised concerns over structural aspects of the programme and inconvenience related to location, timing and time taken to be monitored. Such issues appeared to be of greater concern and inconvenience for those with a disability or with childcare responsibilities.
“with it being away in street, there is that many things happening there as well, it's always in the back of your mind. Not that anyone would think of attacking me but you just never ken”. (female, 55, recently made redundant, group 1)
“First, it was a bad time at 4 o'clock because they work and I look after the grandchildren, you know, after school which was a bad time and then with me being deaf.” (female, 59, retired, group 1)
Despite these problems, most participants recognized that monitoring had to be frequent to be meaningful. However, some believed that any process other than daily monitoring could be misused:
“you can cheat, you can beat that test because they say that it takes like 24 hours for the carbon dioxide to come out your body. You know, you think, well I can smoke today because I don't go into town until the next day..” (female, 36, unemployed, group 2)
Administration
Administration was frequently cited as an issue impacting on participants’ use of Quit4u.
“I mean the £12.50 is great but the palaver to get it, is it worth it? But I guess that's probably because I'm working. People that aren't working probably have the time to do all that but I mean it could have been done, I just haven't got around to it yet.” (female, 35, lab worker, group 3)
Privacy in a busy pharmacy was also raised as a deterring issue, where medical information could be overheard and monitoring occur in public view.
“You are standing in the shop and people can learn your business and that, ken there's no privacy or anything, like when you are speaking about health issues and everything like that.”(female, 35, unemployed, group 1)
Incentive preference
Perceptions about the incentive differed. Some deemed the payment as an incentive to change:
“Well, it's like if you've got that £12.50 on your card for so many weeks and I'm on state benefits so it's no that much so I know that I have got that card and I know I could go up there and go and get shopping.” (female, 44, unemployed, group 2)
Others recognized it as a bonus but not a factor which was going to sustain motivation on a weekly basis:
“It was like, if I was having a good week, yes, £12.50 is coming my way but when you are having a bad week and things are up in the air, I couldn't care less about the money. If it's not there I'm not going to change the way I am. If I do, I mean when I do go and stop smoking again, I'm not really bothered if I get the money or not.” (female, 36, unemployed, group 2)
Discussion
While smoking cessation initiatives which offer incentives have better uptake rates and engagement compared to non-incentive programmes,9,10 our study suggests that a number of factors may still reduce the effectiveness of this approach, particularly after smoking relapse. In particular, the perceived change in the “contractual” and exchange relationship between service provider and client may enhance feelings of failure and deter continuation or future re-engagement post relapse. In addition, practical delivery through location, timing and administration all come at a cost to some clients and therefore reduce the net value of any incentive. Our sample focussed on the one third of individuals who disengaged with the programme. While the issues identified may well be important for future service design it would be important to recognise that two thirds of individuals remained with the format and structure, and for them these issues may not be as important or relevant.
Offering a valued incentive is at the centre of many social marketing approaches. 11 However, our data suggests that for some people the exchange may alter perceptions of the patient/health professional relationship in subtle but potentially important ways. There appeared to be an increased sense of obligation to service providers evident in patients’ comments about failing the service, causing disappointment or anticipating reprimand, and feelings of shame or guilt. Research elsewhere has shown that such feelings are commonly associated with stigma; guilt, emanating from self-criticism and shame, emanating from disapproval from others. 12 Both appeared to be present among those who discontinued with the Quit4U service and perhaps reinforces existing poor self-efficacy and self-esteem issues associated with this socioeconomic group. Whilst this felt stigma was clearly important it is relevant to note that it was not reported by all participants. This may suggest that some individuals do not perceive a shift in relationship (or already see all healthcare provider relationships as this type), that forms of social exclusion have generated a familiarity and tolerance of potentially stigmatizing relationships with providers, or greater self-esteem and self-confidence have proved protective factors. Further exploration of the reasons for this may be helpful.
Identifying the source of this shift in relationship and associated consequences is complex. However, two characteristics of the incentive scheme may be responsible. Firstly, the provision of the service (in this case the voucher) to the client is conditional. It is dependent on a behaviour being supplied (smoking abstinence) thereby removing traditional rights-based access. Indeed, some authors have suggested that extrinsic forms of motivation may risk shifting the client/patient into a position that they in fact feel controlled and manipulated rather than empowered.13,14 Secondly, relational theory suggests that exchange within most societies is based on one of four relationships: communal sharing (CS), authority ranking (AR), equality matching (EM), and market pricing (MP). These relationships vary in levels of equality, structure and co-operation; and by differing social expectancies and roles. Heyman and Ariely have argued that moving from what was previously a social exchange to an economic exchange may alter the type of relationship and in fact actually reduce the amount of effort that people are willing to commit to any transaction (in our case behaviour change). 15 The voucher scheme at the heart of Quit4U is financial and may therefore be regarded as a quasi-commercial transaction; an exchange in which they are being “paid” to provide a service (smoking abstinence). This feeling of a move from social exchange to economic exchange may well be exacerbated by the provision of the service in a setting such as a commercial community pharmacy. In such a scenario, the participant is no longer the client but the provider under obligation: a shift from Fiske's “Communal Sharing” to “Market Pricing”. While the social marketing approach clearly extols rewards as incentives rather than purchases, this may be less clear in the minds of some participants. Theoretically, an incentive should not convey a sense of obligation as the reward follows the behaviour and is therefore dependent on it being initially provided. However, incentive based schemes such as Quit4u offer vouchers over a prolonged period of time (weekly over 3 months). Consequently, if a client receives financial rewards over several weeks or months, they are likely to feel increasingly obligated to remain abstinent on the basis of all the past vouchers that they have received.
One might anticipate that a sense of obligation, however subtle, may be helpful in sustaining a behaviour and engagement in a programme. Indeed it may be regarded as a negative reinforcement with continued cessation promoted to avoid the embarrassment, shame and guilt associated with relapse after having been paid.16,17 Future research could explore this in greater detail and ascertain whether larger payments at more infrequent intervals may enhance the reward and reduce the sense of obligation; or embarrassment could be avoided through continued engagement at a different pharmacy.
Failure combined with the operational similarity to methadone dispensing within the pharmacy, generated a sense of spoilt identity or stigma among some people. 18 Although this stigma was generally felt rather than enacted, there remained sufficient evidence to indicate that the approaches used by staff may require attention. 19 Possible solutions may include changing the location or timing of monitoring (or providing a choice of locality e.g. a smoking cessation group), increasing anonymization by removing the pharmacist's or smoking cessation support worker's knowledge of the test results or reassuring individuals that they do not need to attend if they have relapsed but can remain within the programme.
It was clear that when objective life events, such as bereavement impeded continued smoking cessation, clients were less likely to feel guilty. Indeed, there was an active expression of future intention to re-engage with the scheme. Such views implicate attributional style (in this case, external attribution to a situational factor) in protection from guilt and promotion of future cessation intentions. 20 Consequently, where relapse has occurred pharmacists and smoking cessation support workers may aid continued engagement through discussions of attributing factors of failure and exploration of how those factors might be managed or avoided in the future. A new timetable and action plan for engagement may then be established to translate abstract intentions into concrete action.21,22 Such cognitive reframing in relation to relapse is a known component of cognitive behavioural theory approaches in cessation programmes. It may be of greater importance for addressing relapse and promoting engagement in the context of incentive based schemes.23,24 Reframing may also address perceptions of failure and their resultant guilt. For example, if the current 12 week period was described to clients as three separate but sequential monthly schemes then success may be felt in relation to completion of each individual section. Furthermore any subsequent failure would be felt as only relating to the number of weeks (and associated finance) since the beginning of that month's scheme.
Clients also highlighted the impact of the administrative burden. Locality of monitoring, individual/peer meetings, paperwork and timing of monitoring related to convenience and raised issues such as child-care, working hours and meals times. The threshold of what was perceived as inconvenient varied between individuals. Perceived costs and barriers have been implicated in a number of behavioural theories attempting to explain and predict behaviour. 25 Solutions may focus on readdressing the balance between perceived costs and benefits. In an incentive based scheme this may point to increasing the value of the reward. However, not only would this make the scheme more costly, it may also increase felt obligation and guilt on relapse, thereby inhibiting re-engagement. As a result, it may be more cost-effective to address the problem by reducing barriers/costs such as inconvenience, lack of privacy, timing and embarrassment of association with methadone use.
The National Institute for Health and Clinical Excellence (NICE) Citizen's Council Report indicated some reservations and on-going questions over the acceptability of incentive schemes to promote health. 26 Stated caveats included the arrangement of personal contracts, behavioural monitoring and ensuring that people really were committed to behavioural change before joining such a scheme. These caveats all require additional administration, monitoring and staff. Financial implications aside, these are the predominant issues highlighted in the study that resulted in discontinuation with Quit4u. Although this might suggest that the balance between a successful incentive scheme and public acceptability might be challenging it must be borne in mind that under current arrangements the majority of individuals did not disengage with the scheme suggesting that for most people such procedures were acceptable.
Study Limitations
Although we pursued a diverse sample of respondents, in accordance with purposive sampling techniques, uptake of the research project was predominately by middle aged females. Further research into the views of other socio-demographic groups is required to confirm and/or extend the issues identified. However, accessing these groups may be problematic. Our study may also be potentially subject to volunteer bias. Only those who were willing to share information were willing to take part. All individuals contacted had previously consented to research interest and had volunteered to partake in the study. There is a risk that valuable issues specific to those on the Quit4u register who fulfilled the criteria for this study but did not provide initial consent were not identified. Potentially not all problems associated with the Quit4u service were considered.
Conclusion
There is growing evidence that incentive based programmes can be effective in increasing uptake to behaviour change programmes. However, this research suggests that the incentive based approach may alter the perceived nature of the client/health professional relationship introducing elements of obligation. This may prove useful to promote continued cessation but be unhelpful and promote disengagement post-relapse. The extra administration, bureaucracy and monitoring required by such approaches may counteract the incentive and reduce potential effectiveness. The concept of a “net-incentive” may therefore be helpful when considering the design of such interventions. This suggests that where administrative burden is significant, incentives may need to be raised to make the net-incentive a valuable driver to change behaviour or barriers may need to be altered to reduce the perceived burdens.