
Abstract
Health research funders in the UK now ask applicants to state how their research will involve patients and members of the public. Such involvement can help with questions that researchers repeatedly face: about improving trial recruitment, response rates and follow-up. Patient and Public Involvement (PPI) in research is usually presented in the form of a ladder, from a low rung where studies are led by researchers with no patient involvement, to a high rung where studies are patient-led. This hierarchy does not sit well with many clinicians and academics whose expertise appears to have been downgraded. This article argues that research quality and relevance are optimised when patient expertise is integrated with researchers’ and policy-makers’ expertise, and each role acknowledged and valued, illustrated by an alternative model for PPI which places research and expertise at the centre of the involvement enterprise.
Background
Patient and public involvement (PPI) in research has moved from a special interest area to a requirement in many funding applications. Ignoring PPI is no longer an option: major health research funders in the UK require applicants to state how patients will be involved in their work. 1 Applicants for research funding can draw on initiatives to help them design their PPI, including a UK-wide network of Research Design Services, and NIHR's INVOLVE. Funding bodies themselves are also engaging patients in their decision making.2,3 The scale of the potential patient influence is no small matter, considering that NIHR is investing £4 billion in research and development in the next four years, 4 the majority of which will be allocated with input from patients, and further include patients in research design and conduct. There is also funding for those researching PPI itself with studies exploring both the process and outcomes of PPI in research.5,6
At the heart of PPI in health research lies the idea that health knowledge comprises more than expertise gained through research and medical practice, because patients also have expertise gained through experience of living with an illness and receiving treatment. 7 As such, planning and conduct of involvement initiatives need careful consideration of the nature and requirements of the expertise people bring to the decision-making table. Most models of PPI in health research do not, however, tend to focus on expertise, but are more concerned with how people are involved. Often represented as a hierarchical ladder, involvement is displayed in terms of the extent to which patients are consulted, collaborated with or steer the project.8,9
While this hierarchy has been criticised for focusing solely on power relations and ignoring the different forms of expertise, processes and outcomes that come about in involvement initiatives, 10 it has largely remained as the main model for analysing involvement in health research.
In line with Tritter and McCallum 10 we argue that the hierarchy fails to reflect the complexity of PPI, in particular in relation to the question of expertise. Instead of a hierarchy, we argue that it is more meaningful to apply Rowe and Frewer's focus on the flow of communication: “The lowest level involves top-down communication and a one-way flow of information, while the highest level is characterized by dialogue and two-way information exchange”. 11 The problem with the INVOLVE model is that it implies that consultations cannot be part of a two-way information exchange, and that the value of the involvement hinges on which of these approaches are adopted, rather than focusing, as Rowe and Frewer do, on the extent to which ideas are exchanged and decisions shared.
We propose an alternative model to the hierarchy which places research at the centre and acknowledges the different areas of expertise which contribute to and improve research relevance and quality. If different types of expertise are recognized, the mode of involvement becomes secondary, because the model for scientific inquiry will itself incorporate expertise which lies outside of the scientists’ repertoire.
A new model of PPI in research
We present a new model for considering PPI in health research. We do not contend that this is a fully-fledged and complete product, but intend that it will contribute to a more useful way of planning and conducting involvement initiatives. This model focuses on the expertise needed in research and the key entry points for different experts in the main stages of research.
This model first acknowledges that different kinds of expertise are needed. We argue that, relevant, rigorous and influential research requires expert input from patients and the public, researchers, and decision-makers. This includes, but does not necessarily preference what Collins and Evans 12 have termed experience-based expertise: that which typically is held by patients who have received services and lived with a medical condition. Second, this model plots these different kinds of expertise in relation to key areas of decision-making in research.
This model starts with research prioritization and choosing of research focus and questions. Once a set of priorities have been established, researchers then further develop detailed protocols, choose the research designs and methods, and consider analytical tools; in other words do the research. Finally, policy decision-makers consider the research findings and whether they are implementable in relation to certain contexts defined by cost and acceptability. While each of these groups of people may usefully contribute to each stage, we argue that certain kinds of expertise are more relevant to some stages than others, and that this is defined by the task in hand.
1. Patients and the public have expertise in the problems investigated by research. Their experience of health, illness and receiving services, enables them to identify topics, questions, populations, interventions and outcomes of importance. Examples of this include the National Cancer Survivorship Initiative's consultation with cancer survivors about their research priorities. When compared to the existing research evidence-base, the Initiative found that cancer research was mainly driven by areas of interest rather than areas of need. 13 In another example, patients engaged in a trial of group medication education sessions highlighted the fact that the outcomes important to them were not measurable by the existing research tools. 14 Patients’ expertise not only lies in making the research sensitive to the needs and preferences of patient groups, but also in terms of how the research is conducted. For example, patients and the public may help develop information sheets to make them more user-friendly and relevant, thereby increasing recruitment rates. 15 This is not to say that patients’ capacity to participate is limitless. Research has suggested that when involved in technical decisions, public participation can lead to worse and not better project outcomes. 16
2. Researchers have expertise in designing research, framing answerable questions, choosing appropriate methods, collecting and analysing data. They are trained in the technical skills essential for rigorous research. Researchers who are experts in their topic areas can also situate a problem in a historical context, and are more likely to be aware of topic and methodo logical work that has gone before. This is not to say that research expertise is the domain of academics alone. Patients and the public can become skilled researchers. Nevertheless, some research skills are more easily transferrable than others and a training course does not necessarily equate to expertise. While PPI challenges the notion of research validity, and user-led research has an important contribution to make, the majority of research still needs skilled and experienced researchers.
3. Policy makers and practitioners have expertise in terms of research use and need, including other sources of evidence such as available budgets and the scope of infrastructure. If an intervention is too expensive or complex in its delivery, it is unlikely to ever be implemented irrespective of the research evidence. Decision-makers also have views on what constitutes the problem, from a macro-perspective, and these ideally will inform the beginning of the research cycle, as they often do, in terms of research commissioning. Of course, for much clinical research, there is the added benefit that the researcher is also a clinician.
Each of the three types of expertise outlined above plays stronger or weaker roles at different stages of the research cycle (See Figure 1). The arrows flowing from each stage indicate that decisions made at one stage influence the next, and this will be the same for expertise too, although there is one set of knowledge which will be particularly pertinent at each point. All types of expertise are important for improving research validity and relevance. Focusing on these areas of expertise and where they are needed in research, rather than the degree of involvement of only one group (as in PPI hierarchies do), may help researchers plan their studies more effectively, and clarify the scope for PPI within their studies. Furthermore, by enabling different stakeholders to see what they and one another bring to the process, patients and members of the public, as well as policy-makers and researchers can better understand how they can contribute to enable better research.
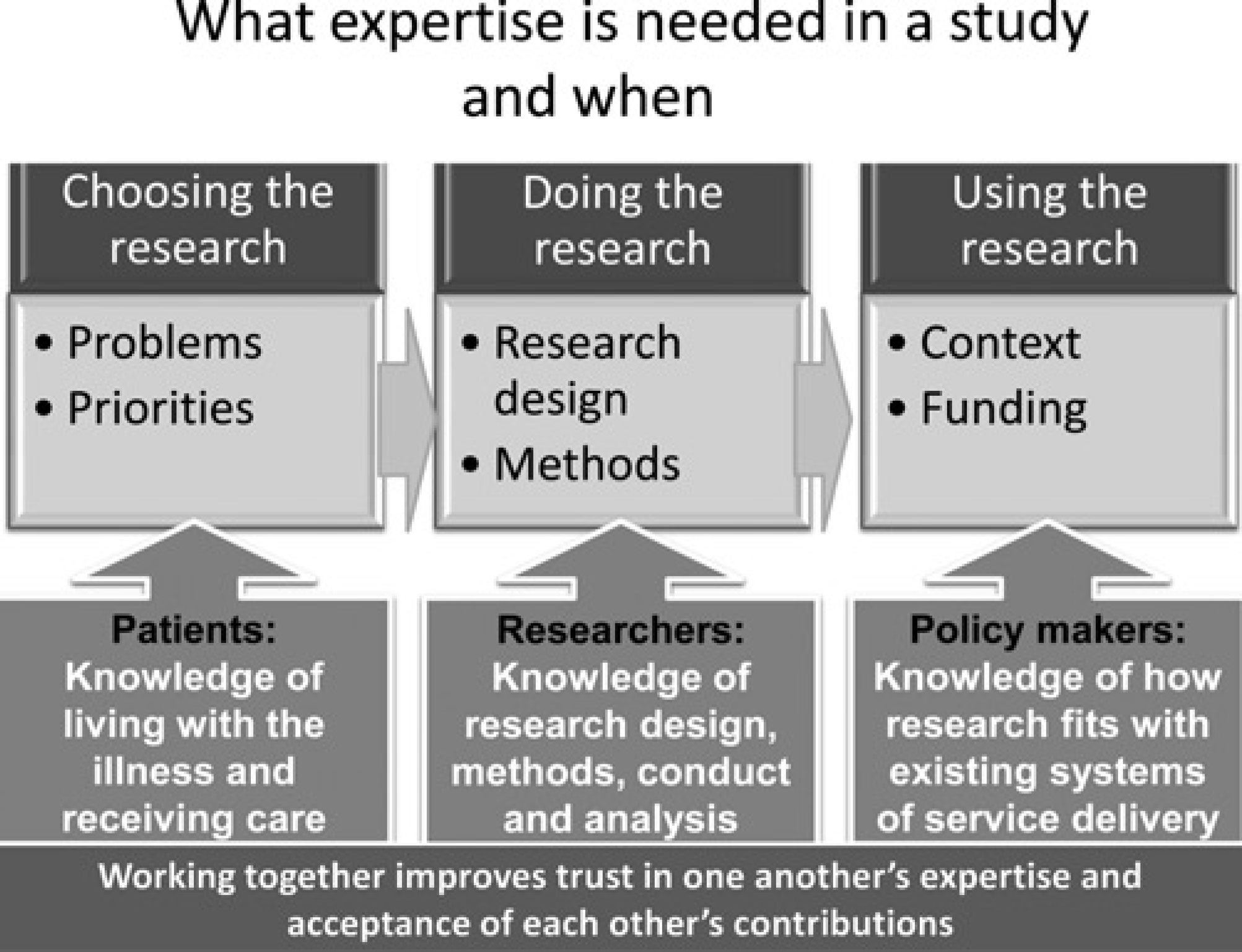
What expertise is needed in a study and when
Discussion
This model focuses on one important aspect of PPI as an intervention, namely the issue of expertise. We acknowledge that it does not present an overall analytical tool for PPI but argue that the core basis for PPI rests on the idea that expertise extends beyond traditional understandings which only include researchers and professionals. Other models are needed for other aspects of involvement, such as how people are brought together, how communication is facilitated and how decisions are integrated into the final research products.
If we accept that there are benefits to be had from including a wider range of experts in knowledge production, how far do we go in involving people, and what requirements do we set for those who become involved? This question has largely been ignored by involvement studies in health research which have focused primarily on the democratic right of citizens to determine how tax payers’ money is spent, and on pragmatic issues, developing standards for how involvement should be implemented and how people should be treated when involved.
A central principle in some research epistemologies is that the researcher should be removed from the field in order to obtain an objective eye and to reduce the likelihood of researchers having vested interests in the findings. Of course, many if not most scientists will have preferences for certain study results, and this is particularly true where there is potential for commercial exploitation.
The challenge of involvement is therefore less related to the issue of bias, and more about who are qualified to be involved and when. Research is a skilled and often technical activity, and researchers are trained in particular methods to suit their field. These methods have been developed over years, through experiments and theoretical work. While it is important to challenge these, it is also important to acknowledge the long-term process of testing and failing that underpins these. Furthermore, some people are likely to be more suitable for involvement, because they have the aptitude for certain skills, such as the ability to listen and reflect on different perspectives.
Two issues arise in terms of who should be involved: what topical expertise they bring and their ‘interactional expertise’. 12 ‘Interactional expertise’ refers to people's understanding of systems and organisations, how they work, and how their own actions relate to the systems. We argue that people should be primarily involved according to their topical expertise, and have suggested a model for plotting this against the requirements of the key stages in the research production process. This is inline with Khwaja's findings on public participation which show experience-based expertise can benefit the topical decisions in a project, but can also be detrimental to technical decisions. 16 As our model suggests, research expertise is needed for technical decision-making, and experience-based expertise is needed for prioritizing research.
Conclusion
The idea that people affected by research should have a say in how the research is focused or conducted is supported by basic ethical and democratic principles, but also by the pragmatic argument that involvement of patients results in research findings which are more relevant to patients’ needs and priorities. However, this idea (in its simplest form) also goes against some of the basic scientific principles, appearing to support the inclusion of potential bias and encourage vested interests. 17 As such, patient influence on research represents both a potential threat to, and the potential improvement of, research validity. Models which describe involvement in terms of a hierarchy over-simplify involvement in terms of the power relationship held between two parties, researchers and users. A hierarchy may be helpful when considering the amount of influence desired in a study, but it obscures the goal of improving the research.
We argue for a model which acknowledges what different stakeholders bring to improving research and when. The proposed model aims to assist researchers who want to plan PPI, helping them to think through when to involve patients and for what purpose. The model also enables research funders to assess proposed PPI in funding applications and consider the potential implications for the relevance and quality of the research.