
Abstract
Objectives:
The objectives of this paper are to analyse the determinants of prostate cancer screening uptake in the Republic of Ireland and to compare the role of non-need factors in uptake of screening among those in and outside the age range recommended as cost-effective for screening according to the European Randomised Study of Screening for Prostate Cancer (ERSPC).
Methods:
The investigation combined a logistic regression analysis of uptake, with an estimation of income-related concentration indices and decomposition of the indices using data collected as part of the Survey of Lifestyle and Nutrition (SLAN) 2007. Comparisons were made across groups differentiated by age in terms of the expected value of the prostate cancer screening.
Results:
Uptake of prostate screening in men 40 years and over in the preceding 12 months was approximately 24%. Uptake was higher among those in age groups that are perceived to receive most benefit from a Prostate Specific Antigen (PSA) test based on the findings of the ERSPC trial. Screening is highest in those with highest socioeconomic status and educational attainment, and who also hold private insurance cover. The largest socioeconomic inequality is observed for men over 70 years of age (0.2298). The smallest inequality was observed for those aged 55-69 (0.1573). Decomposition of the concentration indices shows that possession of private insurance is the largest determinant of inequality among those aged 55-69 (36%) and remains a significant determinant for those aged 40-54 (26%) and those aged 70 and over (17%).
Conclusions:
There are high levels of prostate cancer screening uptake and significant income-related inequality in uptake in the Republic of Ireland. Given that the merits of prostate cancer screening overall and across different age groups are the subject of debate, the high levels of screening and income-related inequalities in uptake warrant closer attention and identification of potential policy responses.
Introduction
Prostate cancer is the most common cancer in men in developed countries. 1 Over the last two decades, in many Western countries incidence rates have risen. 2 In the Republic of Ireland (RoI), approximately 2,500 men are diagnosed annually with prostate cancer and age-adjusted incidence rates have increased faster than for any other common cancer.3–4 As elsewhere, the upward trend is considered to be related to the extensive use in primary care of prostate specific antigen (PSA) testing.5–8 Population coverage of PSA testing is higher in Ireland than many other European countries 6 and the incident rate of prostate cancer was the highest in Europe in 2008. 9
There is debate as to the value of PSA tests at both population and individual levels.6,10–11 Two recent RCTs that examined the impact of PSA testing on prostate cancer mortality had contradictory results. 10 The European Randomized Study of Screening for Prostate Cancer (ERSPC) found that PSA screening decreased mortality by 20% after 9 years, the benefit greatest in men aged 55–69 years. By contrast the Prostate, Lung, Colorectal and Ovarian (PLCO) Cancer Screening Trial found no mortality benefit. At the time the SLÁN data used in this study were collected, there were no formal guidelines on PSA testing in the RoI; however the National Cancer Forum (2006) had recommended against the introduction of population-based screening. 12
In the RoI a mixed public-private health care system operates both in terms of finance and delivery. Those without a medical card (entitlement to which, at the time of the study, was means-tested in those under 70 years and universal in those 70 years and older), must pay a contribution for visiting the GP and for hospital inpatient stays (approximately €60 per visit/night) as well as the full costs of prescription medications. 13 Approximately 30% of the population has a medical card, just under half have private health insurance and some have medical cards and private insurance (thought to afford speedier access to follow-on care where necessary). 14 The varying entitlements evident in the funding system may well impact upon access and observed patterns of service use with respect to care generally and PSA uptake specifically.
We examine the role of income and private medical insurance in the uptake of PSA testing in RoI using data from a large population- based survey. We compare the role of these and other variables in groups of men differentiated by age in terms of their capacity to benefit from testing.
Methods
Data
Data were extracted from the Irish health and wellbeing survey, SLÁAN 2007. This is a large, nationally representative, cross-sectional survey that collected individual data including uptake of prostate cancer screening in the preceding 12 months. Details of the survey are discussed extensively elsewhere.15–16 Data on 2465 men aged 40 and over, were extracted for analysis. Determinants shown in previous work to explain screening utilization in RoI - including, equivalized household income and possession of private health insurance - were extracted for use among the list of explanatory variables. 15–17 No attempt was made to re-weight data as the focus of the paper was on explaining variations in uptake rather than estimating nationally representative levels of uptake.
Concentration indices
Uptake was examined using a series of multivariate logistic regression analyses across groups differentiated by age. The role of income was examined using concentration indices. These detail the degree of inequality in uptake of screening across income groups. The ranking variable used to construct the concentration indices was equivalized net household income. 18 Income was captured in the survey as a series of categorical variables with 25 categories in all; individuals within each category were assigned the relevant class midpoint. Following Kakwani et al. and Van Doorslaer et al., the concentration index is presented as equation 1.19–21

where yi is healthcare utilization, μ is its mean and Ri = i/N is the fractional rank of individual i, with i= 1 for the poorest and i = N for the richest.
As this analysis used a binary response of whether a man had a PSA test in the preceding 12 months or not (age being the only “need” variable examined by stratification), normalized concentration indices employing the Wagstaff framework were adopted. 22 Standard errors for the normalized indices correct for both autocorrelation and heteroskedasticity.

Decomposition Analysis
Decomposition analyses of concentration indices were used to determine the impact of a range of socio-demographic variables on any inequality in screening uptake. This is based on a partition of total inequality into the precise inequalities observed by each individual regressor. 23 As the binary response in this analysis is fundamentally a non-linear relationship, a logistic model was employed with a linear approximation to allow for the correct decomposition. Equation (3) represents the linear approximation of the logistic results where β k n are the average partial effects of each variable (x) – yielding the likelihood of screening (y). Equation (4) represents the decomposition analysis which comprises of average partial effects of each x as well as their means and individual concentration indices.


In equation 4, the first expression represents the contribution of equivalized income, the second expression represents the other socio-demographic variables perceived to influence screening utilization, while the final expression represents the residual term. Separate analyses of men differentiated by age were undertaken. The age ranges selected were based on evidence from the ERSPC study that indicated those aged 55–69 were likely to experience the greatest benefits from screening.10,24
Results
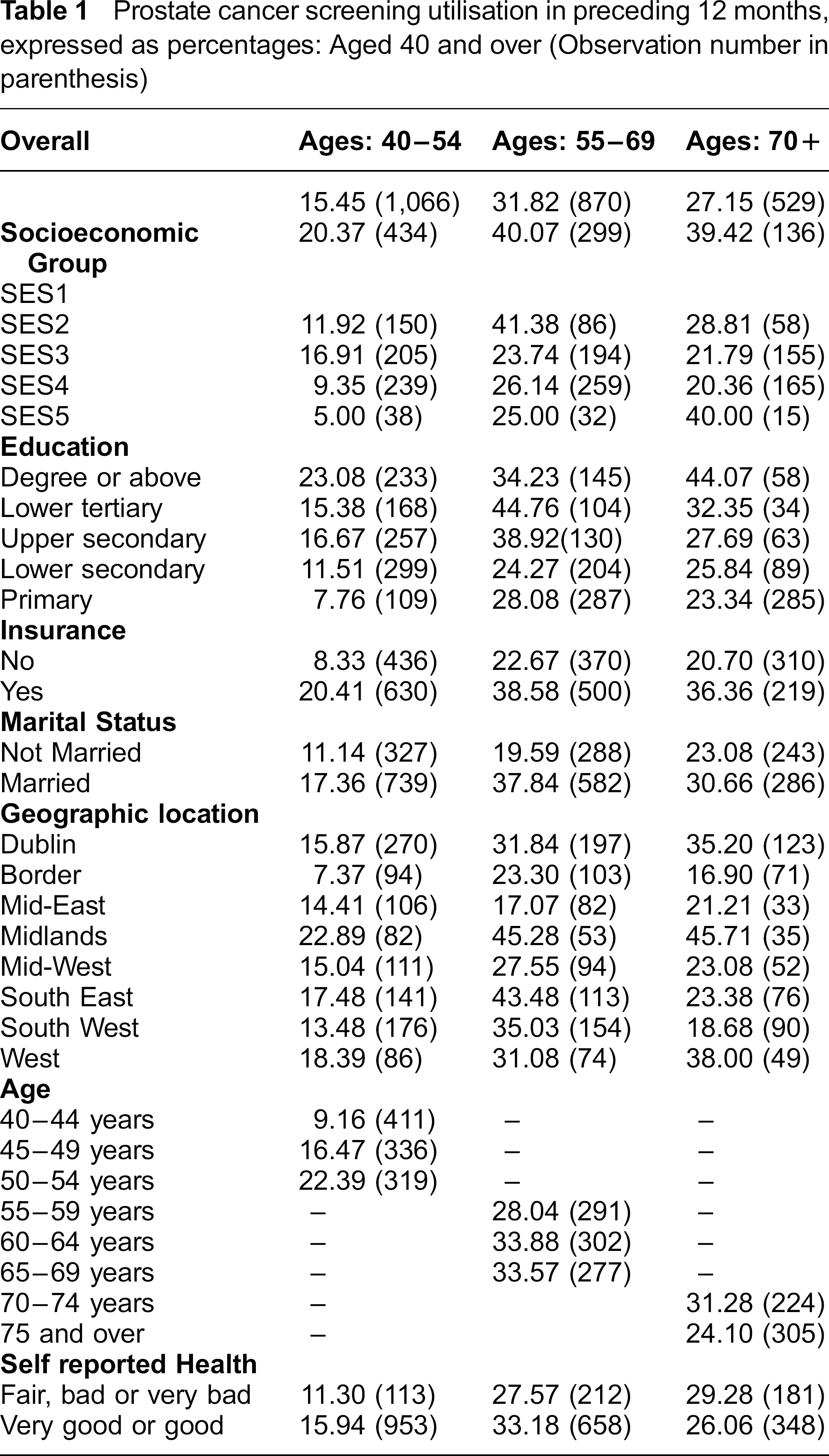
Table 1 presents descriptive statistics on uptake of PSA screening in the previous 12 months. Uptake was highest among those aged 55–69 years (32%). Uptake was also higher among those of higher social status and among those with private medical insurance.
Prostate cancer screening utilisation in preceding 12 months, expressed as percentages: Aged 40 and over (Observation number in parenthesis)
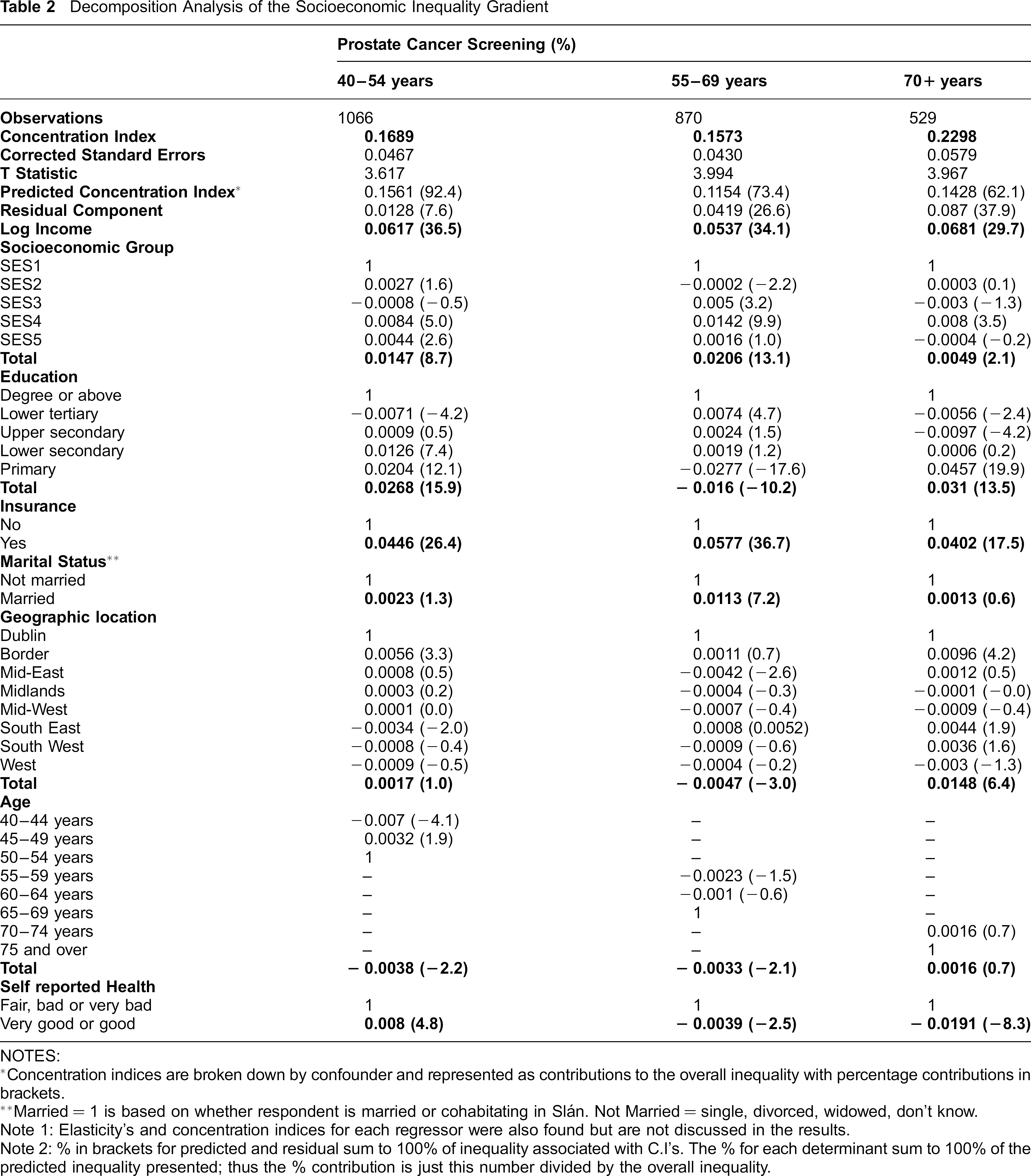
Normalized concentration indices in Table 2 highlight statistically significant income-related inequality in PSA testing. The largest socioeconomic inequality is observed among men aged 70 years and older (0.2298). Private health insurance is the largest determinant of inequality observed in the 55–69 age group (explaining 36.7% of inequality) and contributes significantly in the 40–54 (26.4%) and 70 and over (17.5%) age groups.
Decomposition Analysis of the Socioeconomic Inequality Gradient
NOTES:
Concentration indices are broken down by confounder and represented as contributions to the overall inequality with percentage contributions in brackets.
Married = 1 is based on whether respondent is married or cohabitating in Slán. Not Married = single, divorced, widowed, don't know.
Note 1: Elasticity's and concentration indices for each regressor were also found but are not discussed in the results.
Note 2: % in brackets for predicted and residual sum to 100% of inequality associated with C.I's. The % for each determinant sum to 100% of the predicted inequality presented; thus the % contribution is just this number divided by the overall inequality.
In Table 3, a series of logistic regression analyses are presented examining variations in screening uptake across age groups as a function of the variables specified. Here again we see a significant contribution of private insurance across the three age groups presented. While not the focus of this paper, geographical location and education also play a significant role, though this varies across age groups.
Logistic regression of prostate cancer screening utilisation in preceding 12 months, expressed as Odds Ratios
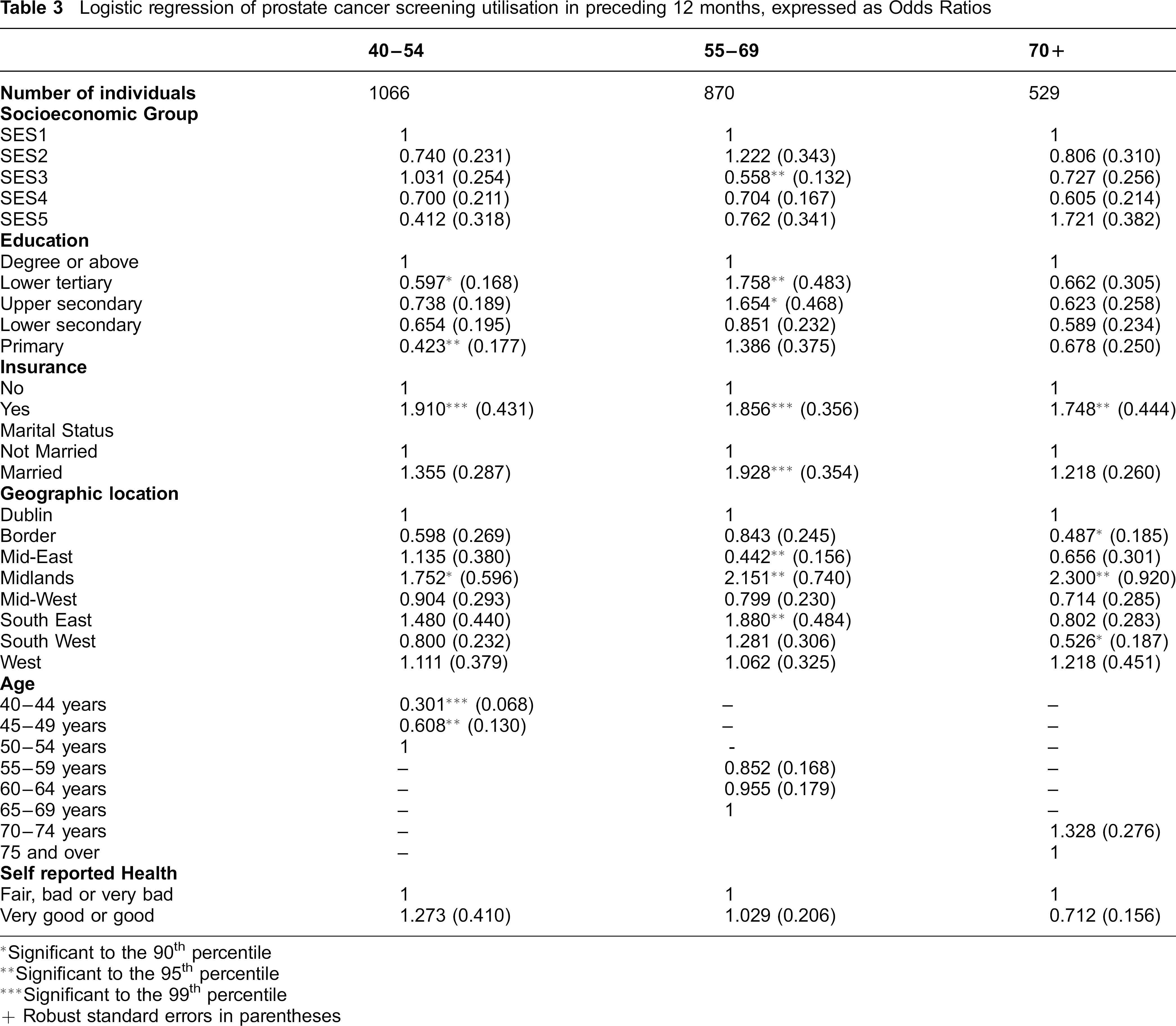
Significant to the 90th percentile
Significant to the 95th percentile
Significant to the 99th percentile
Robust standard errors in parentheses
Discussion
The decision to engage in prostate screening is one that is likely to be taken by the individual in consultation with their clinician; in this case almost certainly their GP. While the decision will be based on a comparison of the costs and benefits of screening as perceived by the individual (and, perhaps also, those closest to them), perceptions are likely to be informed and interpreted with assistance from the clinician. That a pro-rich inequality in uptake of prostate cancer screening exists is consistent with the notion that screening generates information, the value and acquisition cost of which varies across groups. For those with higher incomes, acquisition costs in terms of the out-of-pocket expenses of visiting a GP are likely to present a lower burden relative to those with lower incomes. That pro-rich patterns of inequality are evident among groups for whom risk of cancer has been (based on age) broadly equalized and is therefore not unexpected.
Consistent with the possibility that the value of information will vary as the ability to act upon it varies, the role of private medical insurance can also be readily interpreted. Given that insurance may influence the speed of subsequent diagnosis and follow-up care (if required), it is unsurprising that it should have a significant role in explaining inequalities and is consistent with studies in other jurisdictions. 25 While alternative explanations for this observation exist, (for example, it is conceivable that those who hold private insurance value health more highly and are therefore more likely to engage in screening) that posited here is consistent with other studies examining the motivation for holding private insurance in an Irish context. 26
The comparison of concentration indices across age groups and of the role of private insurance between them is worthy of comment. That the age group among whom evidence for clinical benefits is strongest is the group among whom uptake is greatest and among whom income-related inequality is least, may reflect the relative effort and success of GPs in encouraging uptake. The corollary of this is that among those for whom the clinical benefits are less evident, a greater role is accorded patient choice in the decision process, perhaps indicating a more passive role on the part of the GP. These results are consistent with findings regarding the attitudes of GPs to PSA testing in Ireland where a greater willingness to test asymptomatic men aged 50 to 69 compared to those in younger and older age groups was noted. 6
Some limitations with our analysis are worth noting. Firstly, the response rate in the survey used while high (62%) was not 100%. Secondly, that service use is self-reported in the survey gives rise to the potential for recall bias. As with response rates, it seems unlikely this would materially affect results given the nature of the test and communication of the result. Finally, the relationship between private insurance and screening has been presented in terms of the ability of insurance to facilitate access to diagnostics and care. As noted, it is possible that alternative explanations exist for the relationships observed.
Two policy implications follow from these findings. First, the relatively high levels of prostate cancer screening among age groups where the clinical benefits are questionable present challenges for individuals, clinicians, health insurers and policy makers. High levels of screening not only raise issues regarding resource use with respect to screening itself, but as is evident from the provision of rapid access diagnostic facilities in the RoI for those with raised PSA values, for other parts of the health service.12,27
Second, the clear role of economic variables in the uptake of screening provides policy makers with a range of options by which changes in behaviour might be achieved, should these be considered appropriate. Where GPs currently have difficulty denying access to services such as prostate cancer screening, the use of clearer guidelines to support conversations with patients and/or of higher charges may assist in adjusting behaviour.
Conclusions
Since the merits of prostate cancer screening across different age groups are the subject of continued debate, the high levels of screening in the RoI, the income-related inequalities in uptake and the role of private medical insurance in explaining these are issues that warrant close attention. The potential welfare loss in respect of prostate cancer screening in the RoI may be significant. The importance of economic variables, however, also suggests that policy instruments by which behaviour might be affected could be devised and may meet with some success.
Footnotes
Acknowledgements
This analysis was supported by a project grant from the Health Research Board. Brendan Walsh is an HRB/NCI research fellow in health economics. The authors would like to acknowledge the helpful comments of two reviewers on an earlier draft of this paper.