
Abstract
Objectives
To investigate the tensions faced in commissioning services for children's speech, language and communication needs and to identify variation in commissioning practice in response to these tensions.
Methods
Quantitative and qualitative evidence from a review of speech, language and communication services in one English region, focused on three case studies.
Results
The case studies reveal variation in practice in relation to commissioning tensions generated by: low incidence/high needs cases, blurred boundaries between health and education, multi-agency working, parental voice and service development. The introduction of commissioning and models of practice such as ‘the commissioning cycle’ has left huge variation between localities in levels and type of provision for these services.
Conclusion
Large variation in commissioning practice is associated with commissioners' adoption of one of three models: a market model, an integrated model and a top-up model.
Introduction
A national review of provision for speech, language and communication needs (SLCN) in England made 40 recommendations 1 that later became part of national guidance, Better Communication Action Plan. 2 The review highlighted variation in commissioning and intervention: ‘access to information and services is often poor, services themselves are very mixed, continuity across the age range is lacking, effective joint working between the health and education services is rare and there is something of a postcode lottery across the country. Above all, local commissioners attach a low priority to the subject and we believe that this must change.’ This judgment on the quality and consistency of provision is of concern given the consequences of delayed language in children for their future learning. It is estimated that about 6% of five-year-olds have speech and language difficulties. 3
Factors which create tensions for commissioning
Commissioning is based on a contracting model that aims to create distance between a purchaser seeking to maximize public welfare and competing providers (whether public sector or not). This model has been evolving over many years in the National Health Service in England. Commissioning is intended to improve standards by encouraging budget-holders to consider a range of providers and allow competition to promote quality, whilst still maintaining a strong strategic approach to planning rather than adopting a passive purchasing role. Practice has recently been guided by a commissioning cycle which encourages commissioners to follow a sequence of assessing needs, securing services and evaluating provision. 4 However, a recent government Green Paper asserts a need to improve commissioning of services for special educational needs. 5 Commissioning for SLCN faces five particular challenges.
Low incidence/high need cases
The economic viability of commissioning depends on the possibility of being able to categorize particular conditions such that standard interventions can be costed. When needs and interventions cannot be exactly specified in advance, contracts necessarily remain incomplete. That is, the requirements for service provision are inexact and this makes the position of the commissioner difficult in two ways. First, the commissioner relies on the providers' judgments about the needs to be met. Second, when needs are non-standard it becomes harder for commissioners to judge whether providers are delivering the most appropriate service. Some children with SLCN do not have discreet conditions that can be addressed by single solutions by service providers. 3,7 When children have long term and complex difficulties (low incidence and high need), it is more difficult and expensive to devise a contract to meet their needs.
Blurred boundaries between health and education
Public funding for children's language development has been channeled through two departments in England. Historically, responsibility for all children following a normal development pattern fell to education with responsibility for language delay and disorder falling to health. The chief points of contact between these two services occurred when children with speech and language difficulties made the transition from preschool to school and when school-age children with longer term SLCN were educated in special schools with specialist intervention by speech and language therapists taking place on school premises. Three subsequent policy changes leave the distinction much less clear: public funding and regulation of education has been extended to pre-school children; 8 an inclusion agenda has increased the proportion of children with speech and language difficulties in mainstream schools; 9 and the role of speech and language therapists has changed from providing more or less exclusively child-focused intervention to also supporting other professionals including teachers and teaching assistants through diagnosis, programme design and training. 10 These shared interventions make the boundaries of responsibilities (between health and education) harder to pinpoint.
Multi-agency working
The blurring of boundaries between provision for health and education has been strongly associated with a move towards multi-agency working in which assessment of a child's needs is expected to be holistic, drawing on expertise from a range of professions, and intervention programmes coordinated to match the needs of children and families. In so far as this requires an increase in the amount of time which professionals spend working together, this is not cost-free. Therefore, the additional costs of collaboration should be included in a contract.11,12 This presents the commissioner with a problem, as collaboration costs are likely to be higher if separate providers are contracted for each element of an integrated service. A longstanding body of organizational research treats these costs as a fundamental reason for the existence of organizations or firms. 13 That is, organizations reduce costs by avoiding the need for negotiation required when separate bodies try to co-operate. Therefore, a commissioner reduces the costs of providing an integrated service by commissioning from one organization, but then risks failure to optimise provision of each element of the service. The tensions in commissioning SLCN are unlikely to be eased by indications that underlying models for health and education provision in England are moving in different directions. Commissioning for children's services, led by local authorities, is increasingly emphasizing collaboration between providers in a multi-agency setting, underlining commissioners' ‘strategic understanding of how the whole system works and how the total resource is being used’. 14 Health policy is giving increasing emphasis to commissioners relying on competition between providers to improve the cost and quality of provision. 15
Parental voice
There are three distinct dimensions to be considered in relation to parental voice. Parents may be viewed as consumers who provide crucial incentives for service improvement through their exercise of voice as well as choice (or exit in the terms coined by Hirschman 16 ). This line of argument concentrates on what parents want. Two cases present themselves. In one case, parents voice their preferences through complaints to commissioners, who secure service improvements by tightening contracts or by choosing an alternative provider. Commissioning happily resolves choice and voice in a way which is not envisaged in Hirschman's analysis. In an alternative case, parental voice is largely addressed to providers with only a few unrepresentative voices being heard by commissioners. This alternative case may also turn out well if providers engage constructively with parents to improve the service and to minimize complaints. It may turn out less well if commissioners act strongly on the basis of weak information about parents' preferences. A second argument focuses on what parents know. Parents may be viewed as experts 17 in understanding their child's needs since they have far more opportunity than professionals to find out how their child responds to particular situations. However, we may expect substantial differences between parents in their capacity to deploy their knowledge in negotiations with professionals about their child's needs. 18 Third, parents may be viewed as co-workers in the development of children's language. This argument concentrates on what parents do. The literature relating to parenting programmes indicates that intervention that supports parental skills is associated with improved outcomes. 19 If parents' knowledge and actions have a crucial part to play in interventions to address SLCN then commissioners have to find a way to devise contracts that include aspects of interventions that lie beyond their control. In principle, this might not be too problematic if contracts could specify how professionals should engage with parents. However, commissioners would need to know what constitutes a reasonable expectation of professionals given the particular parent group with whom they are expected to engage.
Service development
Quality improvements over the long run depend on improvements in providers' expertise and capability. There are two tensions here for commissioners. Service development is expensive: commissioners may face a tension between short and long-term quality in choosing between a provider which includes a cost line for service development in a tender and a provider which does not. Also, in a multi-agency setting, service improvement depends partially on developing a strong local network which facilitates good communication and reciprocity in professional relationships. This strongly favours an existing provider and may also, therefore, be a source of organizational slack 20 as existing providers are somewhat insulated from actual and potential competitors.
Method
The evidence reviewed in this paper is drawn from a review of SLCN provision throughout one region of England. The review aims were: (1) develop an understanding of the commissioning, planning and provision of services for SLCN; (2) identify good and innovative practice in supporting children and young people with speech, language and communication needs; and (3) facilitate an improvement process through undertaking a review of the quality of joint commissioning and provision of services for children with SLCN with partners.
This paper reports on aims one and three by reconsidering the data in the light of the five tensions identified through the review of literature.
Sample
All 24 partnerships in the region were invited to participate and 23 organizations took part, with 217 contributions from commissioners, service managers and practitioners. This included meetings with 79 individuals from local authorities and health bodies responsibile for commissioning and delivering provision to a specific geographical population. The invitation asked for representation from multi-agency commissioners, provider leads, and practitioners from a range of services. The commissioner and provider leads nominated participants for the interviews and practitioner workshops for their own geographical area. Many areas functioned as agreed partnerships, but not as formally agreed children's trusts and therefore did not have shared management, funding and delivery of services.
Sources of data
The review team used six sources of evidence to collate information:
Online survey, collecting data on models of service, leadership, staffing and workforce development. This was completed by the provider leads; Guided interviews with strategic leads for providers and commissioners of multiagency children's service. The interview questions aimed to explore how partnerships approached joint planning, commissioning and monitoring of provision for SLCN; Practitioner workshop with professionals from local authority and health services delivering intervention at universal, targeted and specialist needs. The child's journey through services was plotted to identify current processes and service gaps; Quantitative data were gathered for each of the 24 localities. The Child Maternal Health Observatory (ChiMat), was used for data on the number of speech and language therapists.
21
The National Pupil Database was used for the percentage of children with SLCN as the primary cause of special needs.
22
The ChiMat database is a government funded database intended to be used by (amongst others) health commissioners in the assessment of needs. The Index of Multiple Deprivation was used to provide a measure of social deprivation;
23
Evaluation of the review process from the practitioner workshop; Submission of best practice examples from service providers.
Data analysis
Three reviewers undertook the collection and analysis of the qualitative data. A systematic approach to coding the data, identifying themes and assigning the data to these themes was used. The reviewers were then able to make a comparison between organizations and identify enablers and barriers to implementing the national recommendations for children with SLCN. A consensus approach was used to verify the themes and conclusions from the comparison. The results from the interviews, workshops, data mapping and best practice examples are described using three case studies.
Results
Variation in the provision of services as indicated by speech and language therapists per 10,000 children is presented in Table 1. Some of this variation may be accounted for by measurement error in the data provided for the ChiMat database and higher levels of therapists in more socially deprived areas (though there was no statistically significant linear correlation, P = 0.12). However, interviews with commissioners gave some grounds for doubt over the degree to which systematic information was informing needs assessment and decisions over service levels. Commissioners in 11 areas asserted that no use was made of national data in comparing service provision for SLCN and in the remaining localities use of these data was reported as being under development.
Scale of service provision in different areas in one region (Localities ordered by size of child population)
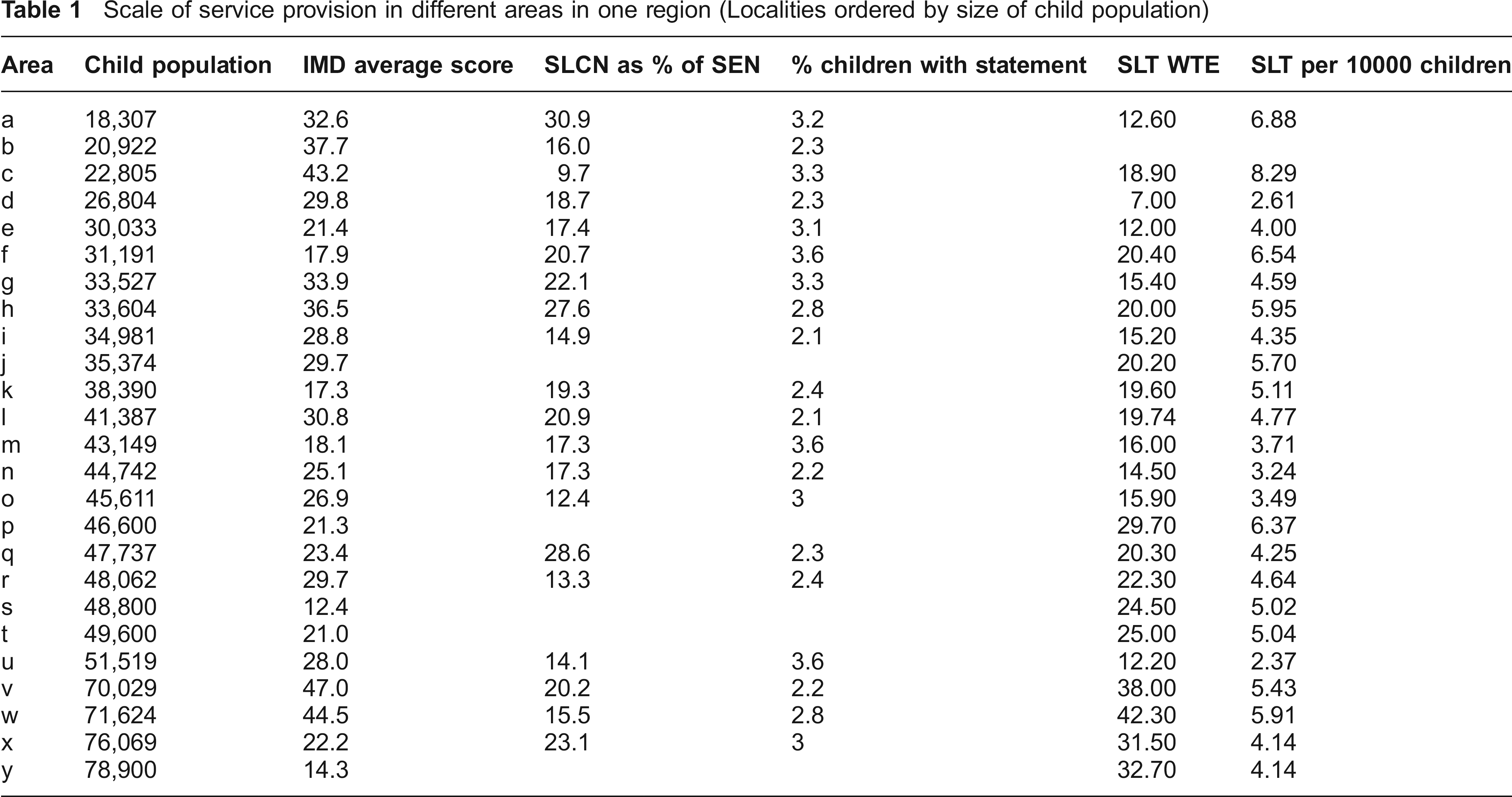
The remainder of this section presents three examples which are based on evidence from interviews with providers and commissioners. The cases have been selected on the basis of illustrating ways in which professionals in different areas have attempted to resolve the tensions outlined earlier. These different ways of resolving tensions also shed some light on the variations in Table 1. The presentation of each case study strives to keep close to the terms in which it was presented by the commissioner and provider. In the Discussion we consider each case in terms of attempts to resolve the tensions outlined in the Introduction.
Case 1
This small area had an index of multiple deprivation score more than one standard deviation above the average. The commissioner and the provider were not able to provide a figure for the number of WTE therapists in the service. An earlier service reorganization left a situation where this area had no in-house provider of its own and the service was commissioned from the provider in a neighbouring area. The commissioner met with the provider lead (who was not themselves a qualified speech and language therapist), but these meetings did not include a representative from education.
Discussion between commissioner and provider was reported as focusing on effective delivery of a historical model rather than review and revision of the service. No reference was made either by commissioner or provider to any review of how the service was meeting the continuum of children's needs in response to questioning about overall provision. The historical service model in this area involved three types of delivery site: clinics, children's centres and special schools. The service was not employing therapy assistants and had not introduced any element of service delivery in family homes. The commissioner and the provider both expressed misgivings about the suitability of this model of service provision but attributed the lack of change to health and education organizations to which the commissioner reported. The commissioner and the provider believed it would not be possible to change from the existing model without an injection of additional resources which the governing boards were unwilling to provide.
The commissioner reported relying on evidence of client satisfaction largely through complaints, rather than through the provider's engagement with parents. There was no system of routinely gathering views from parents and neither commissioner nor provider referred to issues of engagement and participation by parents. It was not clear to what extent complaints had been received directly from parents or from managers of children centres or schools. However, the commissioner reported that they had responded to these complaints by commissioning a private provider for some of the special schools. The proportion of the service being delivered by the private provider was increasing.
Case 2
This small area had a slightly above average score on the index of multiple deprivation and a relatively high level of therapist provision (more than one standard deviation above the average for the localities studied). A joint commissioner represented the interests of governing boards for both health and education and met jointly with provider leads from health (a qualified speech and language therapist) and education (school inclusion) to review and plan service delivery and development. At the time of the data collection the commissioner and the providers regarded their approach to service review, planning and delivery as a work in progress. The service for speech and language therapy was reviewed in a holistic fashion, matching resources to a continuum of need (for children 0 and 19 years and between type of need), rather than matching resources to sharply defined types of provision. That is, resource allocation was not based on historic provision, such as so many clinics and so much for special schools. This approach was facilitated by a decision to merge budgets from different contracts.
The commissioner relied on providers to supply information on parents' views. Simple measures such as pre- and post- intervention questionnaires were supplemented by an initiative which recruited local parents into the provision of speech and language support. These parents provided an immediate source of parental knowledge and preferences to providers. Nonetheless, whilst the commissioner was able to set the format for gathering and reporting parents' views, he was reliant on providers' implementation of this process and, to some extent, on their interpretation of the data generated. In practice, service review and planning was substantially shaped by professional judgement, drawing on providers in education as well as health. This approach to commissioning places a high premium on providers' expertise, judgement and integrity. In the words of the commissioner ‘good joint working between the local authority and health depends on the importance of relationships and good will and the determination to make provision excellent.’ The provider leads described relationships between their staff in exactly these terms, describing colleagues from health and education as having a can-do attitude.
This joint strategic planning process identified problems which were perceived as being shared between education and health. For example, early years professionals were identified as being insufficiently skilled in relation to language acquisition. This was a problem for education because it limited the potential impact of staff employed by education. It was a problem for health since one consequence was that referrals to speech and language therapists from early years professionals were often inappropriate. The agreed solution to this problem was to provide training for early years professionals which was jointly planned and delivered by therapits and staff from education. The commissioner and the providers took pleasure in what they regarded as their innovative approach to service delivery. They referred particularly to a shift away from SLCN provision through clinics and towards provision through nurseries and at home. This included the allocation of resources to therapy assistants who were employed to work alongside teachers and teaching assistants in school and pre-school settings.
Case 3
This large urban area had a multiple deprivation index score almost two standard deviations above the average and a staffing level for therapists just under one standard deviation above the average. There were high levels of migration within the area as well as migration into and from the area. Safeguarding children had for some time been a priority in the design and management of children's services in the area. A Children's Board had been established with representation from education and health and this had governance responsibility for commissioning. However, the commissioner from whom evidence was gathered aligned herself with health rather than referring to herself as a joint commissioner. Evidence was also gathered from a lead for speech and language therapy a strategic lead for special educational needs and an Early Years Foundation Stage strategic lead. Each of these interviewees asserted that they were not clear about the expected relationships between the Children's Board and service provision.
The delegation by the local authority of the budget for special educational needs to schools also meant that they had budgets they could use to commission speech and language therapy, supplementing the baseline service provided by the provider and funded through the health budget. The provider service was responding to commissioning by schools by developing packages of services (such as training or assessment of set numbers of children) which it was intending to offer to schools as products to be purchased. Subsequent to the completion of the interviews for this project, one group of schools in this area decided to jointly purchase services from a national charity.
Although the provider liaised routinely with the local authority children's services, this liaison occurred in service delivery rather than service review and planning. The lead for speech and language therapy and her strategic lead for Early Years explained that the rationale for the type of service provided through the health budget and for the design of services which were to be offered to commissioning schools, was based on their professional knowledge and expertise. In particular, they referred to guidelines provided by the Royal College of Speech and Language Therapy and their own reading of relevant research literature. However, they also developed their own procedures. For example, in response to pressure (from commissioning) to reduce the rate of non-attendance by parents, they introduced a policy removing children from their register after three successive failures to attend an appointment. This practice appears problematic in the context of concerns over safeguarding and the problems with family mobility in the locality. It might be taken as an indicator of the limited connections between health and other services at the level of service review and planning. There were plans to address this problem through a joint service review later in the year.
Discussion
The histories of the organization of services in different areas and the knowledge and perceptions of decision makers have led to quite different ways of trying to resolve the tensions faced in the implementation of a commissioning model. Each case can be viewed as one way of resolving the five tensions in commissioning (Table 2).
Resolving commissioning tensions: altemative models in SLCN commissioning
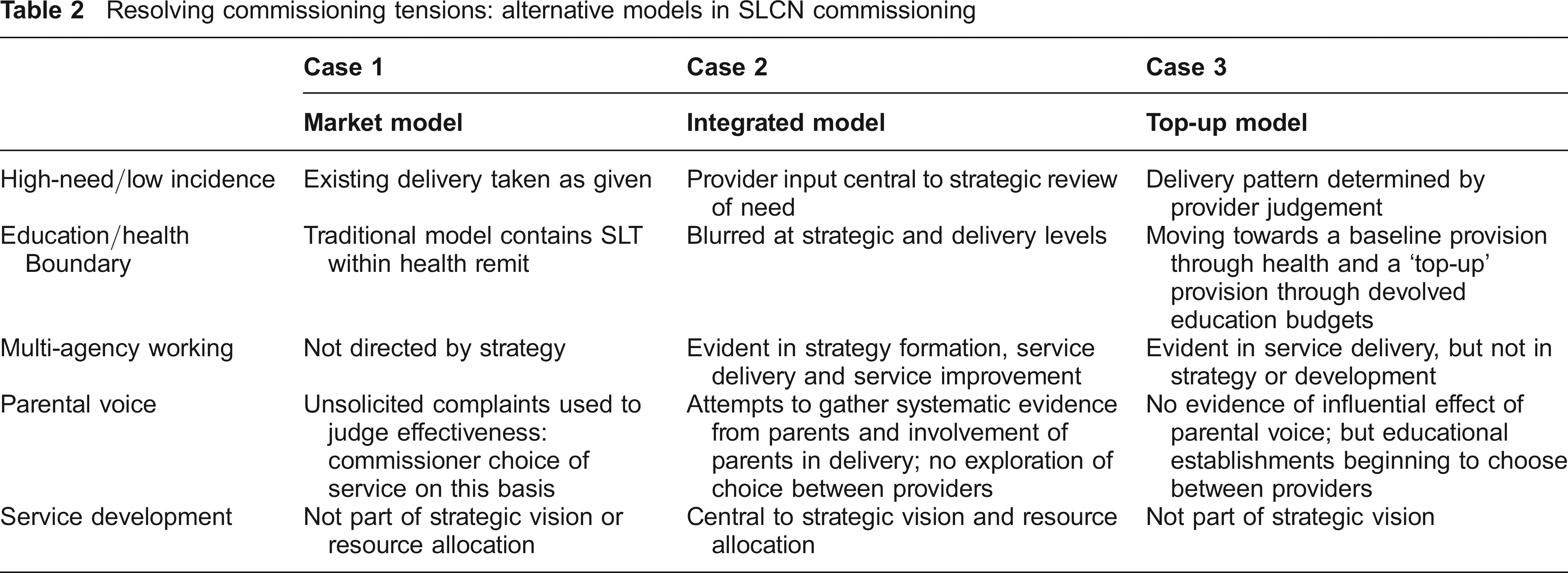
There is some internal coherence within each model which suggests that commissioners are not easily able to mix and match between elements of each model. For example, a commissioner has to choose whether or not to rely on providers in gathering information about the views of parents. This can be an efficient way of gathering data, since providers have direct contacts with parents which commissioners do not, but only if the commissioner can trust the provider. This kind of trust is more likely to be developed in the context of a long-term partnership than a short-term contract in which the provider has reason to worry about losing the business in the near future.
In Case 1, commissioning adopted a market model. The commissioner relied on complaints and attendance rates to gauge parent satisfaction whilst allocating contracts between alternative providers on the basis of performance against these criteria. This model would be sound if the commissioner could be confident that the current service provision was optimal. However, the commissioner asserted that this was not the case. When compared with provision elsewhere, the service looked problematic from the point of view of parental involvement, multi-agency working and professional judgement. The service appeared stuck with a sub-optimal combination of modes of provision through clinics, special schools and children's centre. Complaints about the quality of the existing service could not in themselves provide commissioners with the information that would tell them what kind of improvements were desirable. The role of customer/parent voice anticipated in Hirschman's model 16 is not sufficient to guide service improvement. The threat of switching to other providers will be effective if the problem with an existing provider is organization slack: 20 simply not providing value for money in the exercise of an optimal mode of delivery. It makes less sense if the problem lies with the mode of delivery itself and neither the commissioner nor the new provider is confident about what would be better.
The locality in Case 2 was similar to Case in 1 in terms of child population and deprivation. However, the integrated model of commissioning in this locality was very different from that adopted in Case 1. The commissioner aimed to deal with the information problem by relying on the provider to gather and interpret information on parental preference using their professional judgement. There was no suggestion of switching to an alternative provider and the commissioner worked with the speech and language therapy lead and local authority staff to develop a strategy for SLCN. This model was geared to service improvement through the way in which the provider was operating. It relied on the willingness of the provider to change practices in response to evidence of parental preferences and to be willing to deliver the service jointly with other professionals and parents. In the terms of Williamson's theory of organizations 13 this model reduces transaction costs by internalizing the relationships between commissioners and providers.
In Case 3 commissioning was split between baseline provision through health and a top-up provision commissioned by schools through devolved education budgets. This creates a new way of dividing responsibilities between education and health. The health commissioning implicitly relied on professional judgement to determine practice, whilst the education funding relied on the judgements of school managers. In neither case was there evidence of the attention to parental voice apparent in Case 2 and the exercise of choice was in the hands of schools.
Implications for policy and practice
There is indicative evidence that guidance, such as the commissioning cycle, has not constrained commissioners to adopt similar models of commissioning nor has it yet led to a rough equivalence in the intensity or the character of services provided for one set of health needs: SLCN. These differences are not easily attributable to the strength of commissioners' adherence to good practice. For example, we detected little indication that variation in the intensity or pattern of service delivery was associated with commissioners' use of national data to compare provision with other areas.
This is an exploratory study, so the findings are limited in their general application, and the strength and causality of any associations. However, there are potentially important implications for policy. The literature on purchasing (of which public service commissioning is a special case) has long debated a tension between short-term purchaser benefits from switching between competing suppliers and benefits from long-term relationships with a particular supplier. 24 Short term costs may be reduced by switching between providers but long-term service improvements may be easier to achieve through sustaining a relationship with a single provider.
Commissioners of services for SLCN face this problem without the benefit of information about public preferences provided through the price mechanism. In fact, their access to clients is usually mediated by existing providers. In these circumstances the extent to which a provider believes their contract is under threat may affect the trustworthiness of information they provide and their willingness to engage in long-term service development.
We identified three distinct responses by commissioners of services for SLCN to these problems: a market model of switching between providers for short-term cost-savings; an integrated model which opts for a long-term relationship with a single provider; and a top up model which uses a single provider for a core service whilst switching between alternative providers for additional services. The adoption of each model was associated with a particular intensity and character of service. We see little prospect that change in the structure of commissioning will be sufficient either to diminish this variation or, by itself, to create a context for greater short-term efficiency or long-term service improvement.
Footnotes
Acknowledgements
We are grateful to the participants in the review, delegates at the Service Delivery and Organisation Network and Health Services Research Network Conference 2011, and two anonymous referees for their helpful comments.