
Abstract
Objectives:
To examine the skills and expertise required and used by non-clinical call-handlers doing telephone triage and assessment, supported by a computer decision support system (CDSS) in urgent and emergency care services.
Methods:
Comparative case study of three different English emergency and urgent care services. Data consisted of nearly 500 hours of non-participant observation, 61 semi-structured interviews with health service staff, documentary analysis, and a survey of 106 call-handlers.
Results:
Communication skills and ‘allowing the CDSS to drive the assessment’ are viewed by the CDSS developers and staff as key competencies for call-handling. Call-handlers demonstrated high levels of experience, skills and expertise in using the CDSS. These workers are often portrayed simply as ‘trained users’ of technology, but they used a broader set of skills including team work, flexibility and ‘translation’. Call-handlers develop a ‘pseudo-clinical’ expertise and draw upon their experiential knowledge to bring the CDSS into everyday use.
Conclusions:
Clinical assessment and triage by non-clinical staff supported by a CDSS represents a major change in urgent and emergency care delivery, warranting a detailed examination of call-handlers’ skills and expertise. We found that this work appears to have more in common with clinical work and expertise than with other call-centre work that it superficially resembles. Recognizing the range of skills call-handlers demonstrate and developing a better understanding of this should be incorporated into the training for, and management of, emergency and urgent care call-handling.
Introduction
Demand for emergency and urgent care health services in the UK continues to rise.1,2 Calls to the national 999 ambulance service increased by 3.56 million (42%) between 2002 and 2012. 1 The fragmented nature of urgent care provision makes it difficult to assess demand but Richards et al. (2008) reported a 26% increase in out-of-hours calls following the introduction of the new general medical services contract in 2004 (an agreement between general practices and primary care trusts (PCTs)). 3 Calls to NHS Direct (the national nurse-led telephone service) have increased by 20% every year since its introduction in 1997. 4 In response, government policy has aimed to tackle rising demand whilst simultaneously meeting commitments to improve services and reduce costs.5,6
One route taken to address rising demand has been the use of digital technologies. These offer the promise of changing work practices, workforce configuration and reconfiguring tasks to require fewer or different competencies. As more and more expertise is vested in these technologies, in principle it becomes possible to replace expensive clinical skills with cheaper staff. 7 In urgent and emergency care, a range of digital technologies has been deployed to support nurses and paramedics to provide telephone-based triage, consultation and advice (tasks traditionally undertaken by doctors).8,9 More recently however, telephone triage has been performed by non-clinical call-handlers supported by Computer Decision Support Systems (CDSS).10,11 This use of non-clinical staff is currently being extended and is the foundation of the new ‘NHS 111’ urgent care telephone service.10,11
Emergency ambulance services (999) and GP out-of-hours (OOH) providers have long employed call-handlers to answer calls, but where call-handlers once acted as ‘receptionists’ or operators, taking details and passing on messages to clinical staff,12,13 they are now using expert systems to make complex assessments of callers’ needs. Call-handlers are often portrayed by policy-makers and service providers as trained ‘users’ of technology whose role is to capture the information needed for the CDSS to reach safe and effective decisions. 11 However, these staff are now making decisions, supported by CDSS, about how quickly patients receive care and the type of care they receive.
The size of this ‘extended role’ call-handling workforce is set to increase with plans to roll-out the NHS 111 service. 14 Telephone triage and assessment by non-clinical staff represents a major change to urgent and emergency care, but little is known about the skill requirements of this new group of health workers. Much of the literature about telephone assessment focuses upon clinicians’ use of CDSS.8,9,12,13 From this research we know that nurses commonly draw upon experiential and tacit knowledge when working with a CDSS, 15 and that this work may provide the opportunity to develop new skills. 16 This contrasts however with existing knowledge about call-handlers working in services outside health care, which suggests that there is little room for the development of skills or autonomy where high levels of technical control and managerial surveillance are central to the organization of work.17,18 The implications of this for health care delivery may be that call-handling requires minimal skills and decision-making autonomy. However, the transferability of these findings to health care is not well understood.
This paper presents findings from a larger study that examined how the use of a single CDSS technology shaped everyday work, workforce configuration and service delivery in different NHS emergency and urgent care settings in England. The aims of this paper are to: describe the key competencies, qualifications and experience required to perform call-handling work; and understand the skills, experience and expertise that call-handlers actually use in their everyday work. This paper offers the first description of call-handling skills and work, and discusses the implications of this new form of health care work for the organisation and delivery of services.
Methods
We undertook a detailed comparative case analysis of non-clinical call-handlers’ use of a CDSS to triage calls. Survey and ethnographic (non-participant observation, semi-structured interviews and documentary analysis) methods were undertaken in three settings. This small number of comparative cases offered the optimum combination of close familiarity with individual settings and work, with the opportunity for analytical and theoretical generalization. The ethnographic (08/H0104/56) and survey (09/H0104/65) components of the study were approved by Wiltshire Research Ethics Committee.
The CDSS
The CDSS is an NHS-owned system designed to enable trained call-handlers to offer safe clinical triage of calls to emergency and urgent care services. The assessment concludes with a disposition determining the clinical care needed and the time frame in which this is required. If an emergency ambulance is not required, an automatic search of an integrated database is used to locate an appropriate service local to the patient.
Settings
We examined call-handling in three different settings:
‘999’ – an emergency call-handling service run by an Ambulance Trust, serving large cities and towns, and some more remote rural areas (population of approximately 2.5 million). The CDSS has been deployed in this setting since 2006. ‘SPA’ – a single point of access urgent care telephone service operated by the same Ambulance Trust. This new service began in October 2009 for two PCTs (population of about 600,000). Call-handling operates 24/7. ‘OOH’ – a long established GP-led out-of-hours service, serving a large town and surrounding suburban area (population of approximately 140,000). The CDSS replaced a ‘paper protocol’ system for prioritizing calls in October 2009.
Ethnographic methods
This study component employed observational, interview and documentary methods to provide a detailed understanding of the design, management and use of the CDSS in each setting.
To identify the qualifications, skills and experience that service providers and the CDSS developers believed important for performing call-handling, we examined job descriptions from organisational and job vacancy websites, paper recruitment materials, and training and audit materials from each setting. To explore the first aim of the study and complement the documentary data, semi-structured interviews were conducted to examine call-handlers’ and managers’ perceptions of the call-handling role, including discussions about their skills, experience and expertise. A purposive sample of interviewees was identified following initial observation in each setting, and included call-handlers and associated stakeholders (e.g. system developers, corporate and operational managers). Interviews typically took 30–90 minutes. A topic guide was used to explore experiences and views about call-handling and using the CDSS. In total, 61 interviews (approximately 20 per setting) were conducted with 64 participants (34 call-handlers, 11 supervisors/managers, 4 clinicians, and 15 corporate/operational managers).
Observation was conducted in call-centres to examine call-handlers’ use of the CDSS, including their skills and expertise and whether these deviated from those skills and practices required by the organization. This totalled nearly 500 hours of observation (170, 172 and 149 hours at 999, SPA and OOHs respectively), conducted at different times of the day, over approximately 35–45 days in each setting over several months. Detailed notes were overtly taken and transcribed soon afterwards.
Qualitative analysis
Fieldnotes and transcripts were read and open coded independently by five members of the research team. Documents were examined looking for specific details, for example, recruitment documents were examined to identify required qualifications and competencies, audit measures for norms and expectations of practice. Emerging codes and themes of interest were discussed. Interpretations were arrived at through discussion until consensus was reached. Data were imported into Atlas. Ti 6.1 and coded to facilitate data management and retrieval. As the study progressed, analysis was structured to examine all the data about each setting in turn, and then across settings using our research questions. Normalisation Process Theory was used to structure the analysis. 19 Narrative and data summaries were written to support the analysis and a mixture of analytical approaches was used such as identifying and refining themes, and charting to facilitate comparison.
Survey
The survey of call-handlers was designed to provide further data on the skills that call-handlers perceived to be important. It also focussed on aspects not fully captured by the ethnography including call-handlers’ qualifications, demographic characteristics, previous work experience and work aspirations. The list of skills was developed from our documentary analysis of a Continuous Quality Improvement tool (CQI) used to audit call-handler performance. Items were grouped into six ‘competency categories’: call control; questioning; listening; providing information/advice; communication; and using the CDSS functionality (Table 1). Call-handlers were asked to rate the importance of skill in performing their role, scoring from 1 (not very) to 10 (very important). Items derived from the CQI were supplemented with questions about skills and practices identified in the qualitative analysis, including team-working and knowledge sharing. The survey consisted of 26 skill items in total.
Skill competency categories and individual skill items
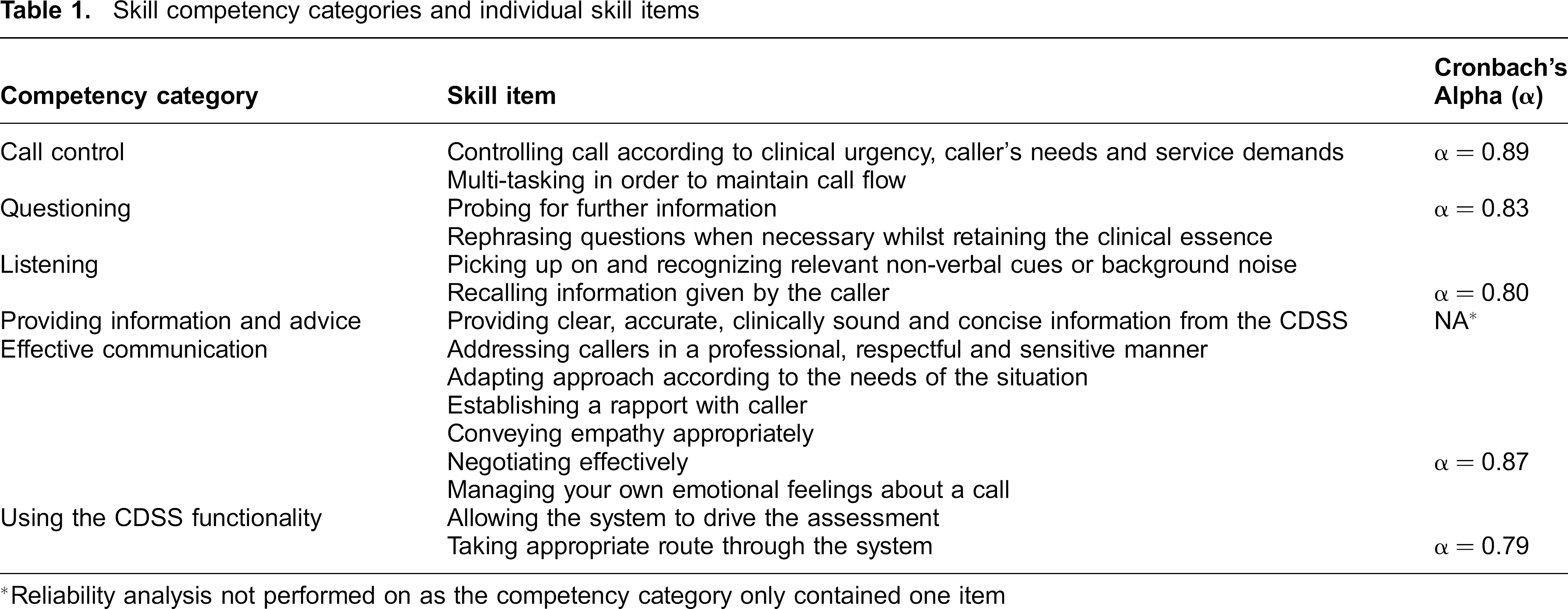
Reliability analysis not performed on as the competency category only contained one item
Following survey piloting with staff at 999, who commented on survey length, readability and content, rewording questions and adding of items were undertaken. All call-handlers (n = 166) were sent a questionnaire: participant information sheet and Freepost return envelope: 999 (n = 53); SPA (n = 59) and OOH (n = 54). The survey was distributed by managers or the researchers. A follow-up reminder was e-mailed after 3 weeks.
Survey analysis
Data were double-entered in MS Excel and exported to IBM SPSS. Data were summarized for the call-handlers’ characteristics and qualifications, career aspirations, previous work experience and skills. Skills items were averaged for each competency category; descriptive statistics were calculated. Reliability analysis (Cronbach's Alpha), performed on all fifteen items for the competency categories, revealed a high level of internal consistency (α = 0.94). Each competency category also revealed high levels of internal consistency (Table 1). Chi-squared tests and Analysis of Variance were used to test for differences between settings.
Results
Job requirements: qualifications and skills
Analysis of documents about 999 and SPA job specification included the requirements of computer skills, decision making, negotiation, communication and multi-tasking, as well as personal attributes (team player, integrity, flexibility and willingness to work under pressure). In OOH, the core skill specified was to be able to provide a fast, accurate and effective telephone call-taking service in an emergency setting to identify the best route of care. There are no national academic minimum educational requirements, 20 but our examination of job descriptions and advertisements revealed that, at 999 and SPA, a minimum of 5 GCSEs (A-C) or equivalent was required. Training materials, designed by the CDSS developer team, encompass key aspects of using the CDSS (e.g. clinical decision making, providing care advice), as well as developing communication and interpersonal skills (e.g. listening, negotiation skills, controlling the call).
Call-handling workforce: characteristics, qualifications and experience
Of 166 questionnaires, 106 (64%) were completed and returned, 31 (58%), 39 (66%) and 36 (67%) from 999, SPA and OOH respectively. The majority of call-handlers in each setting were female. SPA and 999 had a younger workforce compared to OOH (Table 2). Most call-handlers fulfilled or exceeded the minimum of 5 GCSEs (A-C) required for employment by 999 and SPA (Table 2). SPA call-handlers showed higher levels of educational achievement – 67% had A-levels, or a university degree. OOH call-handlers had lower levels of educational qualifications, possibly reflecting the older average age of this workforce and also perhaps the higher proportion of part-time workers.
Characteristics of participants by setting

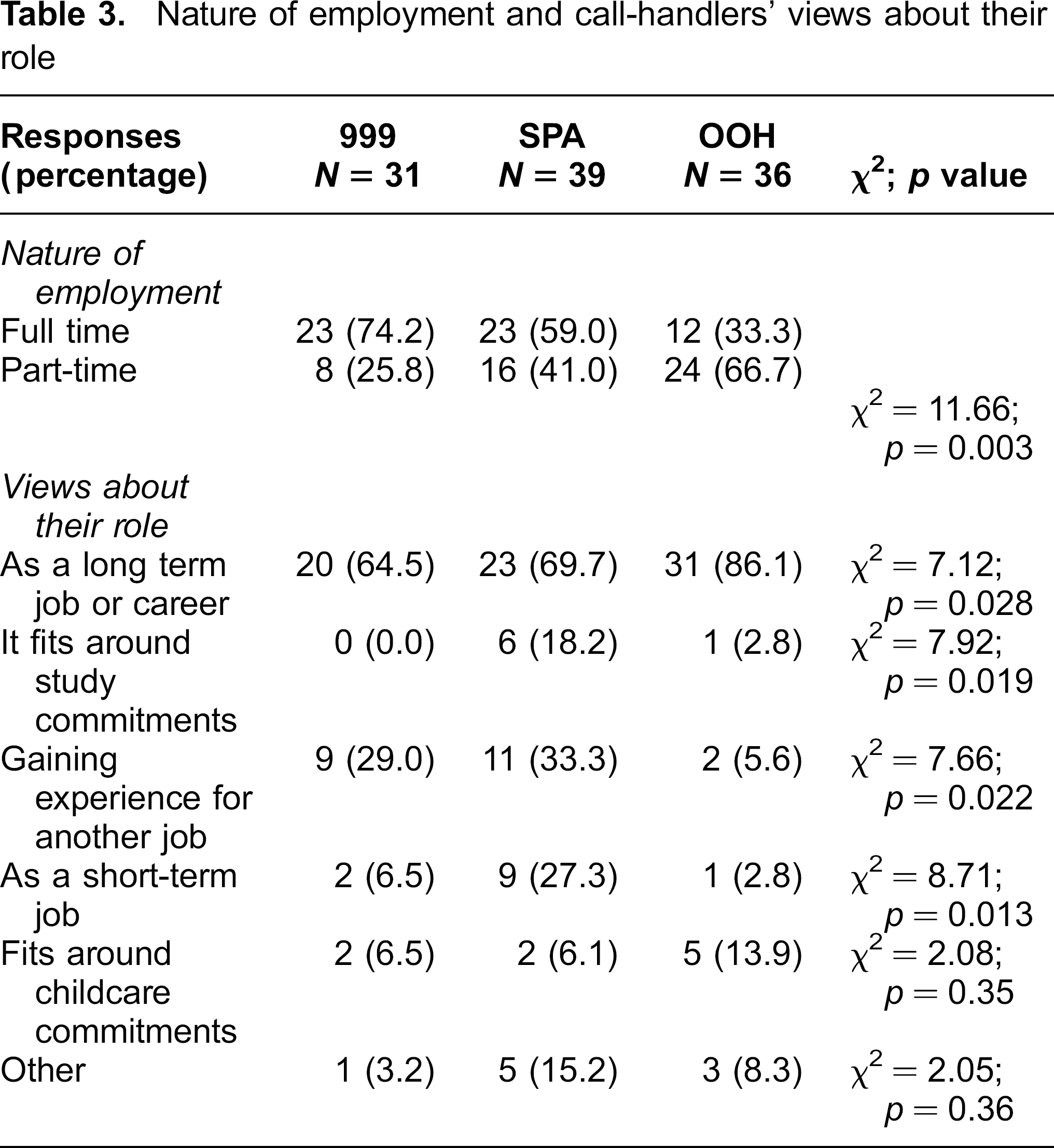
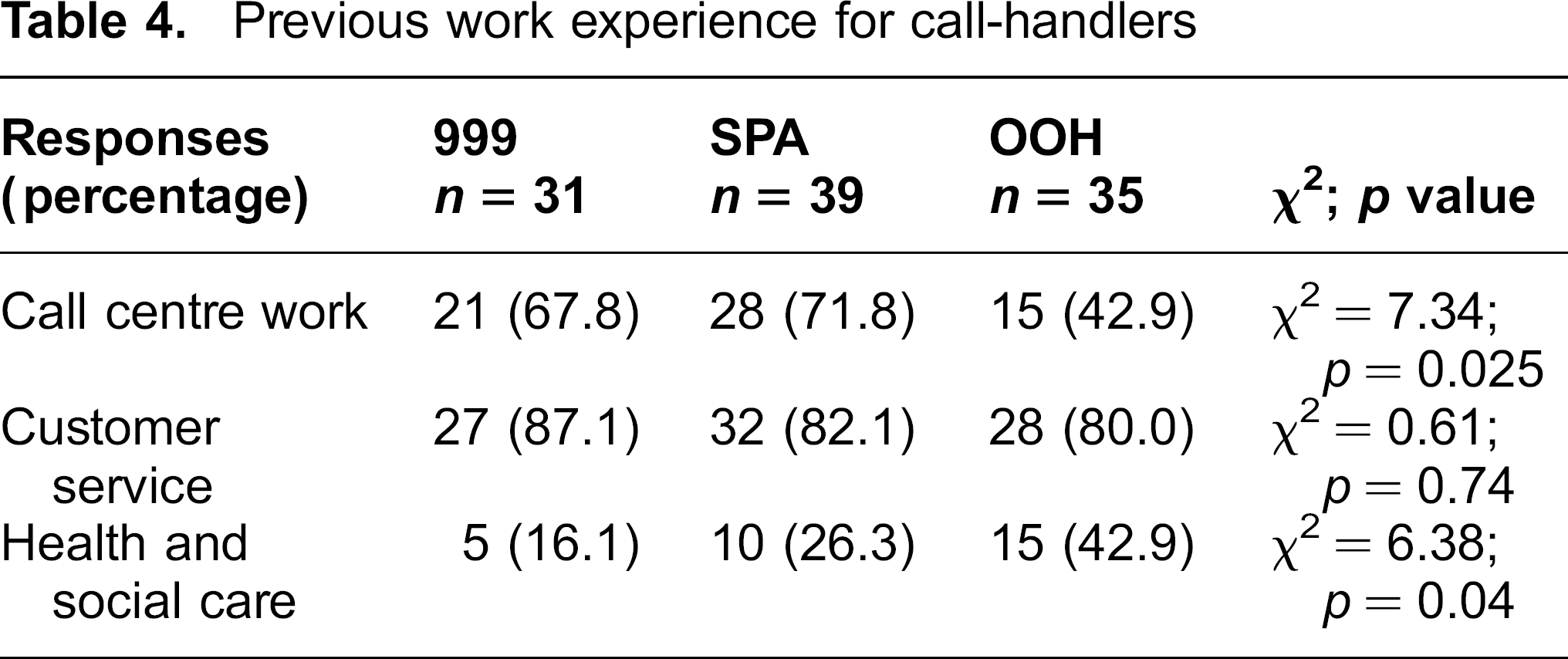
The majority viewed health care call-handling as a long-term career, particularly in OOH (Table 3). This is slightly surprising since many were employed on a part-time basis, or reported using the job to gain experience for another job. Although previous call-centre experience was not explicitly required by employers, many had experience of customer service roles (over 80%) and call-centre work (Table 4). Almost half of OOH call-handlers had experience of health or social care settings.
Nature of employment and call-handlers’ views about their role
Previous work experience for call-handlers
The key competencies: What skills do call-handlers perceive as important?
Consistent with the requirements specified by service providers, call-handlers from all settings rated all competency categories identified in the CQI as important (Table 5). Telephone assessment requires offering information and advice, and call-handlers rated this as the most important set of skills needed to do their job. Across all settings, call-handlers endorsed the importance of allowing the system to drive the assessment and taking the appropriate route through the system (‘effective use of CDSS functionality’) (Table 5). Some call-handlers acknowledged that this was important because they lacked clinical training.
Call-handlers’ rating of the importance of skills (figures are means (SD))
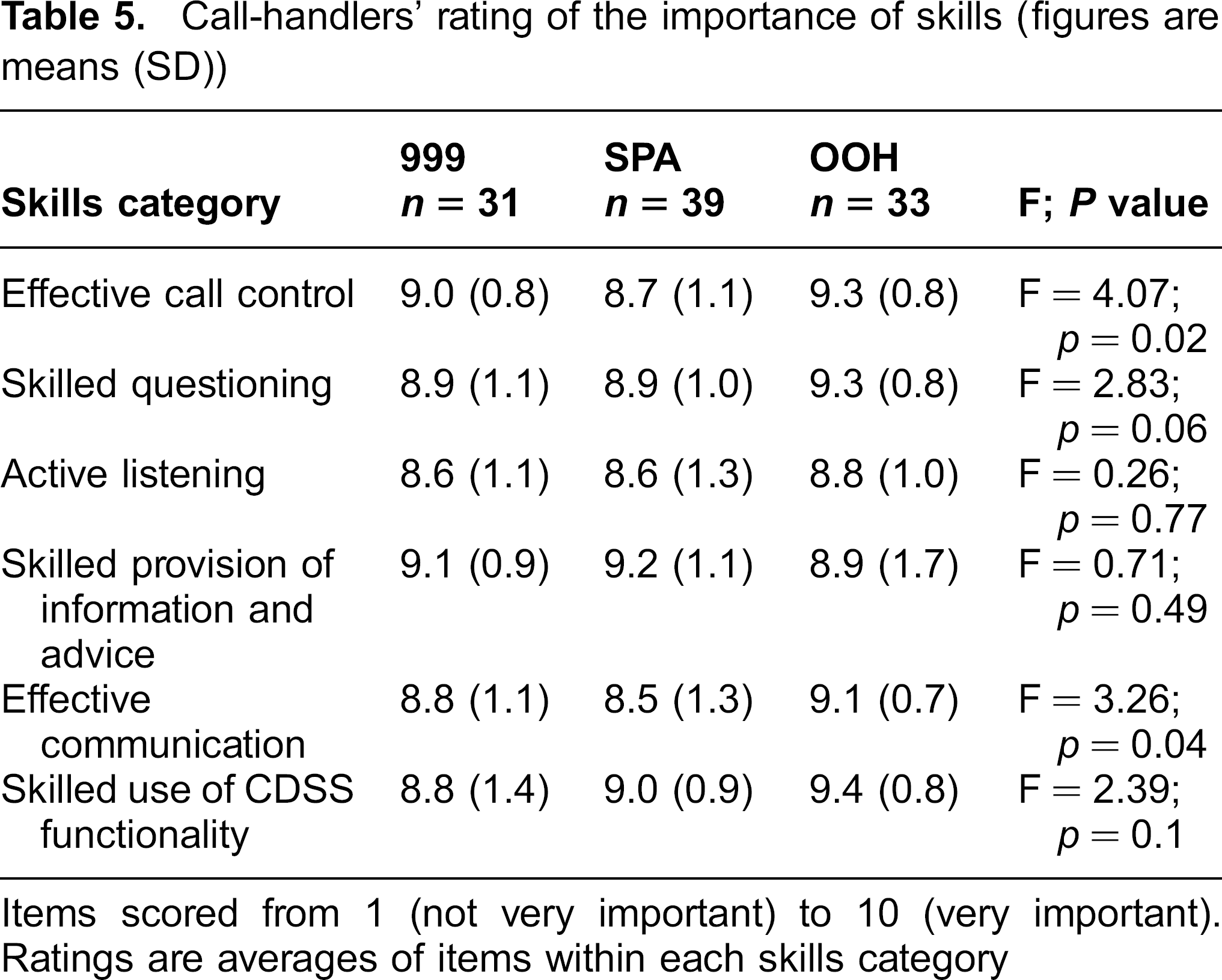
Items scored from 1 (not very important) to 10 (very important). Ratings are averages of items within each skills category
A patient calls with back pain. He provides lots of additional information, requiring the call-handler to ‘[
As long as you're using the supporting information, keeping the clinical essence, probing enough … it's pretty much foolproof as far as over the phone can be […] If doctors [used the CDSS] they'd probably go, “well, I'm not happy with this. I'm going to ask them a question that's not on the system,” but that's not our job to do. Interview, SPA call-handler, CT63.
The everyday work of call-handling
In addition to the job requirements and key competencies, the observation work identified an additional set of skills, experience and expertise that call-handlers used in their everyday work which was not included in the CQI.
Team work
The ability to work as a team is assessed at recruitment, but it is not part of performance audit assessment. Working alongside, and supporting other call-handlers, were highly valued aspects of the work and appear to add interest. This finding applies to all settings, but was particularly apparent at OOH (Table 6). In all settings, the spatial location of the work appeared to facilitate team communication and sharing of knowledge – and, in turn, support the operationalization of the CDSS and call-handling work:
Call-handlers’ rating of the importance of skills not assessed in the formal audit process (figures are means (SD))
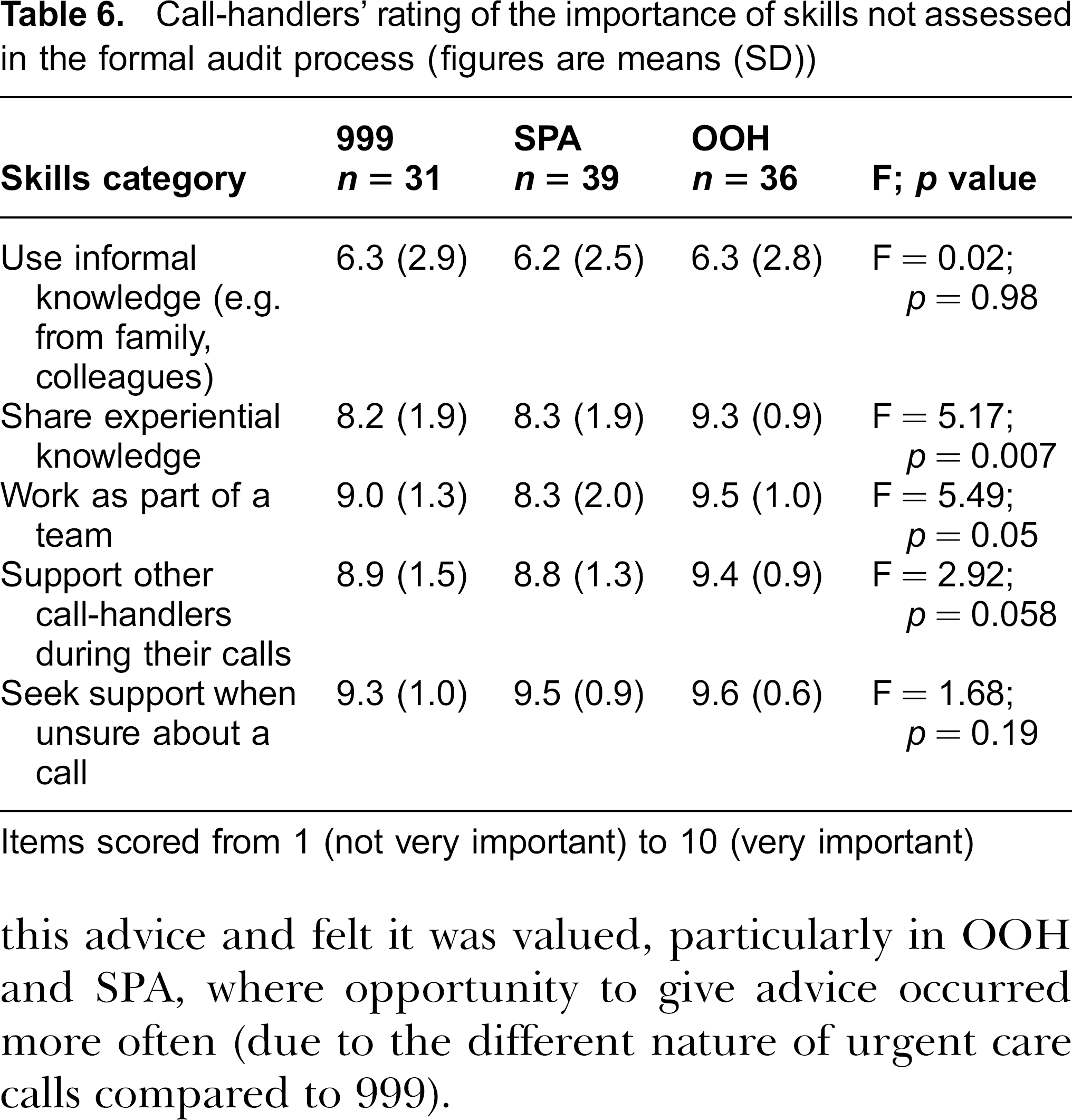
Items scored from 1 (not very important) to 10 (very important)
…you're not trained or told you've got to help [other call-handlers]. But when you start, people are obviously keeping an eye out for you … Then, once you pick up stuff … you just go over, and start trying to do something. Interview, 999 call-handler, CH18.
We're all in it together. If someone doesn't know then somebody else does … We're always listening in [to see] if you can help. Interview, OOH call-handler, CH82.
Developing pseudo-clinical expertise
Qualitative analysis suggested that call-handlers develop ‘pseudo-clinical’ expertise. Although we did not observe call-handling prior to the introduction of the CDSS, the range of tasks appears to have increased. For example, offering clinical information and advice, supported by the CDSS, adds a greater clinical component to the role. Call-handlers often enjoyed being able to give this advice and felt it was valued, particularly in OOH and SPA, where opportunity to give advice occurred more often (due to the different nature of urgent care calls compared to 999).
… you didn't take calls as far as we do now … you just got the main bit of information for the [ambulance] crew … I think they probably feel they're helping the patient a lot more, because there's a lot more on-line care during the call. We always gave CPR [instructions] … but now they tell them how to give the ‘hypo kit’ &; how to do fever management, paracetamol … I just think it's a totally different model of call-taking. Interview, 999 manager.
Call-handlers internalized knowledge of the system and the clinical information it contained – so that they were able to anticipate questions. This was especially noticeable at 999 where the CDSS had been deployed for several years. Additionally, those who had worked with the system for some time (999 and OOH) drew on personal and experiential knowledge about medical conditions or health care.
The call-handler is typing demographic information and she asks a caller with hip pain “Can you put any weight on it?” “Have you had an injury?” “Has it got worse?” These questions are asked before reaching the point in the assessment where the call-handler selects the relevant body part on the screen to invoke the appropriate algorithm. Observation, 999.
The call-handler says “we've all got our bits of knowledge … someone's husband has diabetes, someone else knows about asthma”. They can ask each other for advice and learn from their experiences. She describes a call about a baby who was fitting. Prior to the CDSS, advice included removing some layers of clothes, sponging with cold water and opening windows. But this call-handler still advises “right well, undo the top buttons of her cardigan and open a window”. The call-handler merges her advice with the CDSS to offer what she thinks is the best advice. Observation, 999.
The survey suggests that call-handlers rated the use of informal knowledge from friends, family, and colleagues less highly than other key competencies (Table 6), reflecting their awareness that this is not formally sanctioned, but nonetheless they acknowledge its place in their work. In OOH, there was less explicit emphasis on the clinical component of the work, but the levels of embodied knowledge seemed similar.
We're not diagnosing … if I'd wanted to be a doctor or nurse, I'd have done that years ago […] It's interesting, but I don't think we need it for the job because [the CDSS] does it for you […] Our job is to collect information, input it, and let the system … come out with the appropriate course of action. Interview, OOH call-handler, CT82.
‘Translation’ skills
Service providers, the CDSS developers and call-handlers all recognise that the work requires a high level of communication skill. The observation revealed that the call-handler acted as a ‘translator’ between the technology and the caller and this was critical to the assessment of the call. This included rendering clinical terms or colloquialisms comprehensible and providing explanations, and conversely, interpreting the caller's description of the medical problem to fit the options in the CDSS:
We were told in training to stick to the question first … a lot of research has gone into it. They [CDSS developers] have tried to get the best wording possible … but sometimes that just doesn't work, so you have to work round it. You've got to be sure obviously, not to lose the clinical essence of the question […] and in [this region] … different words mean different things, there's all the slang. Interview, SPA call-handler, CH62.
A man calls on behalf of his son. His first language is not English. He is OK with most words but has difficulty with some e.g. “slurring”. The call-handler tries several different ways to explain. Observation, 999.
Interpretive flexibility
There appears to be an inherent tension in the work of call-handing. On the one hand there are strong normative messages in their everyday work which reinforces the claim that “if you follow the system you can't go wrong” (Observation 999). On the other hand, call-handlers are expected to use a degree of “common sense”.
Some will use it like a robot … They'll say, ‘well I can't ask that because I'll deviate from the system’. But I always say ‘we expect you to use some common sense and judgement’. It's not about deviating from the system, it's about sometimes having that gut feeling we all get when we think something's not right […] You've got to allow call-takers to be empowered but you've got to give them some guidelines Interview, 999 Clinical supervisor.
This suggests that call-handlers are sometimes expected only to follow the system, but, at other times, are expected to know when it is acceptable to use ‘common sense’. This potentially may create variability in the way that call-handlers perform their role. It should be noted that using ‘common sense’ was particularly notable in settings where call-handlers had more experience overall (999 and OOH). In summary, the use of experiential knowledge, common sense, and translation suggest a degree of interpretative flexibility in call-handling work.
Discussion
This paper identifies the skills and experience required and used by non-clinical call-handlers using a CDSS to manage emergency and urgent care calls. We have examined the stated requirements (for example in recruitment documents), the perceived skills (notably via the survey) and those used in the everyday work of call-handlers.
Call-handlers had a range of skills and experience prior to joining the organizations, but it is notable that many had higher qualifications or competencies than required. This possibly reflects economic recession or limited local employment opportunities, but may mean that the training context has to be tailored to a higher level of competency or could have negative consequences for staff retention as overqualified staff become bored with their work. High attrition rates are well-documented in non-health care call-centres 21 as are concerns about high-skilled/low-paid workforces, where lack of career development opportunities may engender a lack of commitment amongst staff. 22 It is notable, however, that many call-handlers in our study viewed their job as a long-term career, suggesting high levels of commitment. We suggest that the health care context and the pseudo-clinical nature of the work add prestige, making the work more attractive, but this requires further investigation.
Similar to commercial call-centres, key recruitment requirements included staff skilled in communication, team working and flexibility.23,24 Our findings reveal that call-handlers agreed that these key skills were highly important. Call-centre work is typically highly individual, but frequently organized in teams. 25 In our study, call-handlers highly valued working alongside other call-handlers and this was crucial in developing their skills and experiential knowledge.
The extent to which call-handling is high or low skilled work is debated. 26 This work is often presented, in a technologically-optimistic narrative, as low skill. Repetition, lack of control and high levels of monitoring are well-documented,17,18 but it is also suggested that many call-handling roles require greater skills to perform what has been termed emotion and articulation work. 22 Whilst health care call-handling work may share some lower-skilled characteristics (e.g. lower pay, monitoring and auditing), we have found that it involves considerable skill and expertise. We suggest that call-handling in this sector is a complex task combining high levels of communication and cognitive skills, such as translation and skilled questioning that draws on experiential knowledge of symptoms, local dialect, and health care. The way in which call-handlers draw on wider knowledge to use the CDSS indicates that not all the expertise is inside the CDSS. This alternative knowledge is however, problematic in relation to the formal rhetoric about ‘following the system’ and the evidence being ‘in the machine’. In this study, the CDSS was introduced to standardize decision-making so that it did not rely on expertise or experience: service providers, CDSS developers and call-handlers place the utmost importance on the CDSS driving the assessment. However we observed experiential knowledge, expertise and other informal knowledge and considerable interpretive flexibility in everyday use to accomplish the task of call-handling. There are parallels here with studies about nurses’ use of CDSS, which have described how they draw upon their experiences and appear to integrate this experiential knowledge with the expertise contained within the CDSS, to inform their decision making.27,28
Previous research has noted the importance of good call-handling in patients’ experiences of using health services, 29 but until now little attention has been paid to the skills of call-handlers. We have provided unique insights into the call-handling workforce in urgent and emergency care. This study compared call-handling in three different settings, two of which were located within the same Trust. We are confident that our analytical framework (using Normalisation Process Theory 19 to structure the analysis) allows replication of our approach and that this, and the common features of NHS 999, SPA and OOH settings, enable transferability of our findings to other similar care settings. However, further work is required to examine how far our findings are generalizable to different types of service or health system contexts (indeed, we are currently undertaking a study of CDSS in relation to the ‘NHS 111’ telephone service).
Our survey was necessarily of the relatively small number of call-handlers available in the settings, but we obtained a reasonable response rate (64%) and these data are supported by rich qualitative data. We were unable to collect information about the demographic characteristics of non-responders.
Our findings suggest that call-handlers are more than merely passive users of computer software. They actively engage with CDSS to accomplish the tasks of triage and call-management. A better understanding of this needs to be incorporated into the training and management of emergency and urgent care call-handling. Current training and audit activities reinforce the idea that embodied and experiential expertise are not required when using the CDSS, but accommodating this expertise appears to be important for everyday call-handling work. It may be helpful to use the strength of team knowledge sharing to acknowledge this expertise so that it can be managed in ways that allow rigorous quality assurance while also developing informal knowledge constructively.
The workforce of non-clinical staff who perform clinical assessment and triage supported by a CDSS is growing. We suggest that the work done by call-handlers in urgent and emergency care settings has far more in common with clinical health care work than with the other generic call-centre work that it superficially resembles. Recognizing the range of skills call-handlers demonstrate and developing these will be essential if technologies like CDSS are to deliver on their promise.
Footnotes
Acknowledgements
Our thanks go to the participating NHS organizations and research participants. This project was funded by the National Institute for Health Research Service Delivery and Organisation programme. The views and opinions expressed therein are those of the authors and do not necessarily reflect those of the NIHR SDO programme or the Department of Health.