
Abstract
Objectives:
To examine differences in the amount of treatment provided by UK and non-UK trained dentists in the Scottish National Health Service.
Methods:
Using a unique administrative data set, we utilize multivariate fixed effects regression models that control for patient characteristics and unobserved heterogeneity across dentists to explore the extent of treatment delivered.
Results:
Non-UK trained dentists initially provide more treatment than UK-trained dentists, but over approximately two years of practice their treatment converge.
Conclusions:
As with many OECD countries, the UK relies on foreign-trained health professionals to address workforce shortages and one concern is whether they provide equivalent health care to their domestically trained counterparts. Whilst there is a difference in the amount of treatment provided by UK and non-UK trained dentists, the effect is modest and transitory.
Introduction
To address the shortages of trained health care professionals, many Organisation for Economic Co-operation and Development (OECD) countries have adopted a mixture of long-term policies of increasing domestic training, improving retention, and adapting skill mix, and short- or medium-term policies of international recruitment. 1 Foreign-trained health professionals have proven to be a flexible and low-cost resource and make a significant and escalating contribution to health care labour markets in industrialized countries. In the year 2000, there were approximately 420,000 (18%) foreign-trained doctors and 710,000 (11%) foreign-trained nurses working in the OECD. The United Kingdom (UK), in particular, has become one of the largest recipient countries, with 33% (69,813) of the doctors and 10% (65,000) of the nurses working in 2006 qualified overseas. 2
There are important questions for policy-makers regarding the extent to which foreign-trained professionals are substitutes for their domestically trained counterparts, especially in the realm of health care, where in the presence of asymmetric information such professionals have considerable discretion over the type of care they deliver.1,3 Furthermore, reducing unwarranted variation in health care is a priority in the British National Health Service (NHS) 4 and the “NHS Atlas of variation” has been published “to stimulate, within all levels of the NHS, a search for unwarrented variation”. 5 Our research fits into this broader agenda through assessing the extent to which the location of training gives rise to variation in dental health care.
Variation in dentists’ clinical treatment decisions has been well documented in terms of the provision of specific procedures, the costs and number of procedures provided for specific patients, diagnoses, intervention decisions and treatment selection for individual teeth. 4 Research has concluded that individual training programs, personal experiences, and new information can all lead to inter-practitioner variation. 6 Our research provides further evidence on the impact of country of training.
This paper uses a detailed administrative data set to compare the treatment provided by UK and non-UK trained dentists in the Scottish NHS from their initial engagement for two years. To control for unobserved heterogeneity in dentists’ characteristics, we adopt a fixed effects linear regression model and include an extensive set of variables to control for observed characteristics of patients. We observe an initially modest difference in treatment, with non-UK trained dentists providing more treatment than their UK-trained counterparts, but this difference is largely eroded after two years of practice.
Methods
Setting
The majority of primary care dental services in Scotland are provided by the NHS General Dental Services (GDS). The costs of GDS treatment are met in part out of public funds, but, unlike other health services supplied by the NHS there is a substantial element of patient cost sharing; unless exempt from charges the patient pays 80% of the NHS fees for their treatment up to a cash limit.
The GDS Terms of Service, 7 require dentists to set out and complete “the care and treatment (if any) which in the opinion of the dentist, at the date of that examination, is necessary to secure and maintain the oral health of the patient”.
Most GDS dentists are non-salaried and are paid a fee for each treatment provided, which are regularly published in the Statement of Dental Remuneration (SDR). Salaried GDS dentists are usually recruited to areas where access to GDS is limited. While salaried GDS dentists are not paid on a fee-for-service basis, the treatment they provide is recorded in the same way as for non-salaried GDS dentists.
GDS dentists may also provide treatment privately. Very little is known about the extent of private sector dental services, but the Information Centre for Health and Social Care reported that about 12% of dentists in Scotland who responded to a survey about working patterns reported spending more than 75% of their time on private dental care. 8
In order to practise dentistry in the GDS, dentists need to obtain a list number, which in turn requires they be issued with a Vocational Training (VT) number to indicate that they have satisfactorily completed their training in the UK, or are exempt from that requirement for one of a number of reasons, including that they are EC/EEA nationals and hold a recognized European Dental Diploma. Figure 1 shows that the number of VT numbers issued has more than doubled during the past nine years. Most of this increase was accounted for by EEA nationals. Non-UK trained dentists come from a wide range of European countries and the five most common countries of application since Vocational Training year 2000–01 are Poland (36%), Ireland (14%), Greece (13%), Spain (9%) and Germany (8%) (see 9 for information on the inflow of non-UK trained dentists in NHS Scotland).
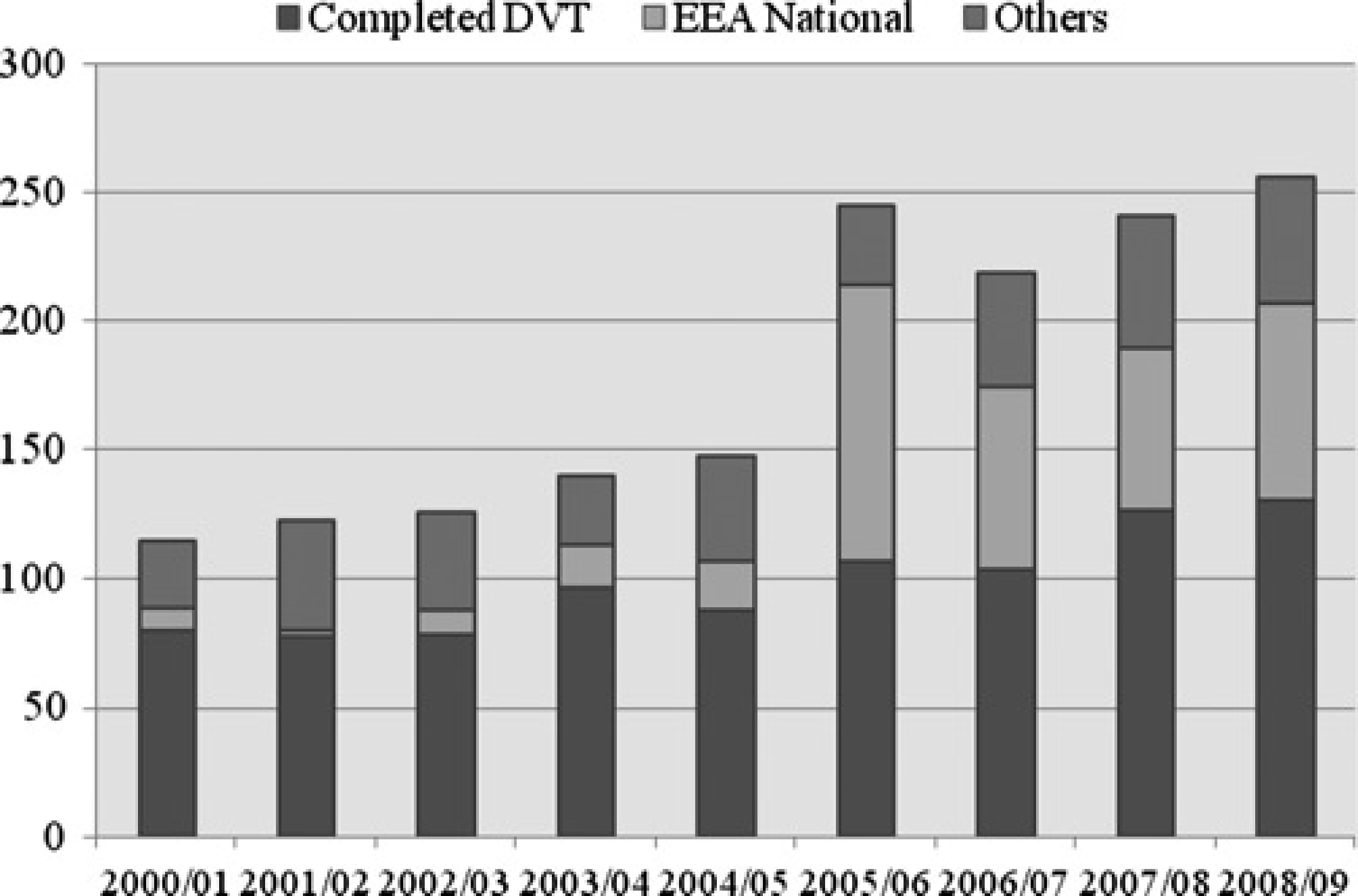
VT Numbers issued by vocational training years
The current policy framework for dental services in Scotland was set out in 2005 in the Dental Action Plan. 10 This described a series of policy initiatives designed to address poor oral health, provide better access for patients and provide incentives for dentists to practise in the public sector. One of the policy initiatives was to recruit about 35 dentists directly from Poland in 2006, to arrive in Scotland in three cohorts. These Polish dentists were employed on a three-year contract with the salaried dental service after satisfactorily completing an intensive eight-week English course and attending a two-week residential course. 11
Data
The anonymized treatment data are derived from the Management Information and Dental Accounting System (MIDAS), which is a large-scale administrative database that records all GDS treatments paid for in Scotland. The bundle of treatments that are necessary to secure and maintain the oral health of the patient is called a claim. Practitioner Services (Dental) monitor and verify these claims before payment is made.
A sample of data on UK and non-UK trained dentists was acquired by identifying dentists issued with a VT number. For non-UK trained dentists, the sample was restricted to include only dentists who began providing treatment after January 2006 until the end of the sample period, September 2008. For UK-trained dentists, the sample was restricted to dentists who completed Vocational Training in 2006.
The initial sample consisted of claims for treatment provided to adult patients by 199 non-UK trained dentists (264,843 claims) and 83 UK-trained dentists (217,755 claims) and paid before September 2008. In order to control for the effect of the duration since the patient's last course of treatment, each patient's first treatment was dropped, which restricted the sample to 116,211 claims made by 192 non-UK trained dentists and 112,394 claims made by 83 UK-trained dentists. Finally, we restricted the sample to the first 24 months of a dentist's experience in the GDS, which further reduced the sample size to 107,378 claims made by 192 non-UK trained dentists and 108,528 claims made by 83 UK-trained dentists.
Non-UK trained dentists had fewer claims per dentist during the sample period. This may in part reflect the fact that non-UK trained dentists were only observed for an average of 14 months compared to 22 months for UK-trained dentists.
Table 1 reports the descriptive statistics separately for UK and non-UK trained dentists. For confidentiality reasons, we do not report descriptive statistics of variables associated with a small number of dentists. Our dependent variable is the value of a claim, which is measured at constant GDS fee levels, and gives a natural measure of the amount of treatment that a dentist provides to a patient. While Table 1 shows that non-UK trained dentists provide nearly 3% more treatment per claim, Figure 2 shows how treatment per claim changes during the sample period. As reported elsewhere, 12 Figure 2 shows that while there is some difference between UK and non-UK trained dentists initially, there is convergence from the fifth quarter after entry onwards. Figure 2 also indicates that both groups of dentists exhibit an initial period during which the amount of treatment per claim increases. This reflects the fact that during the first few months of practice, only relatively low value claims will be paid because larger value claims are likely to be provided over several dental appointments. Thus, we focus on the treatment provided after the second month from entry. This reduces the sample size to 103,412 claims made by 179 non-UK trained dentists and 107,668 claims made by 82 UK-trained dentists.
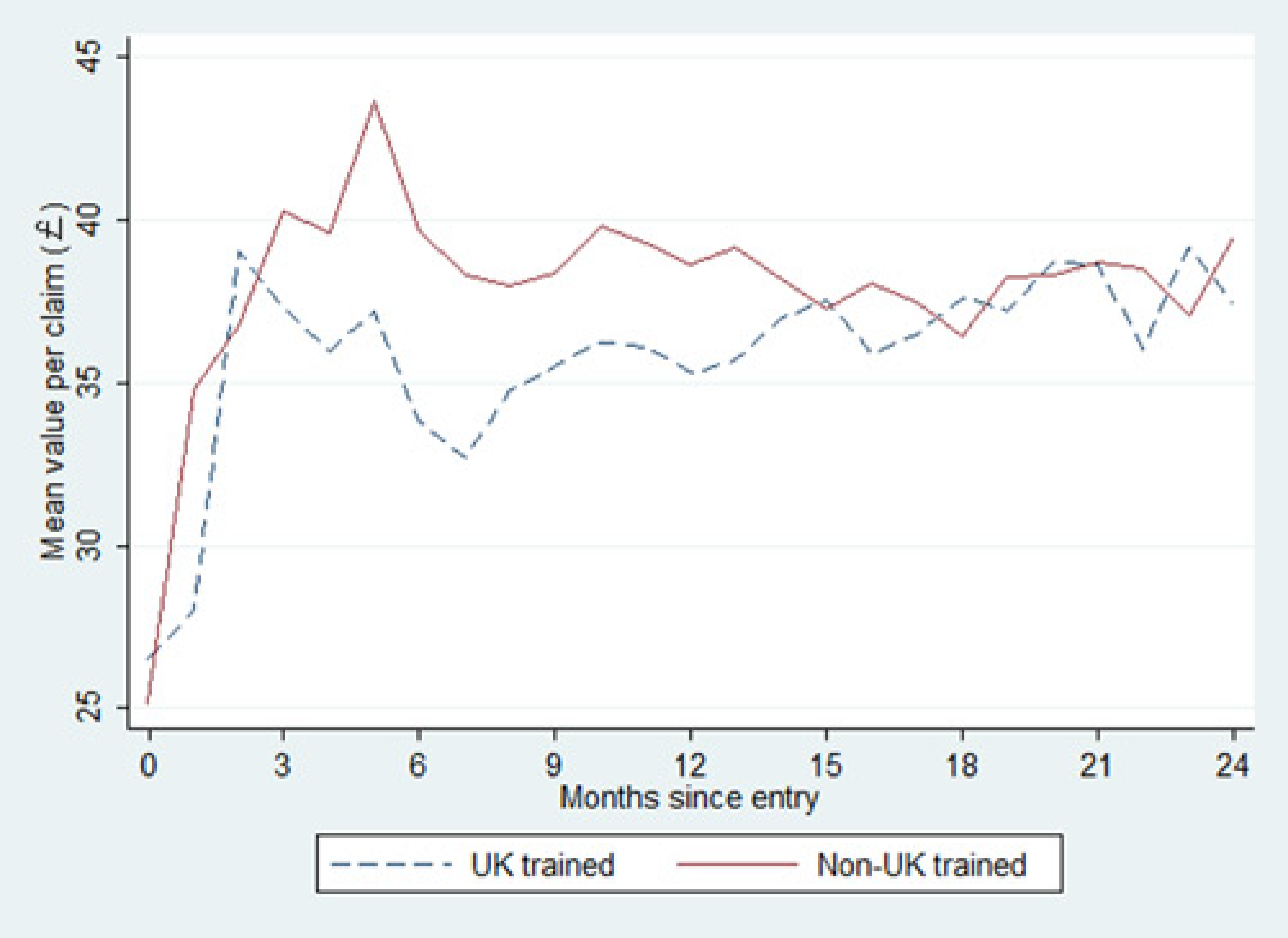
Average treatment value for UK and non-UK trained dentists over time
Descriptive Statistics
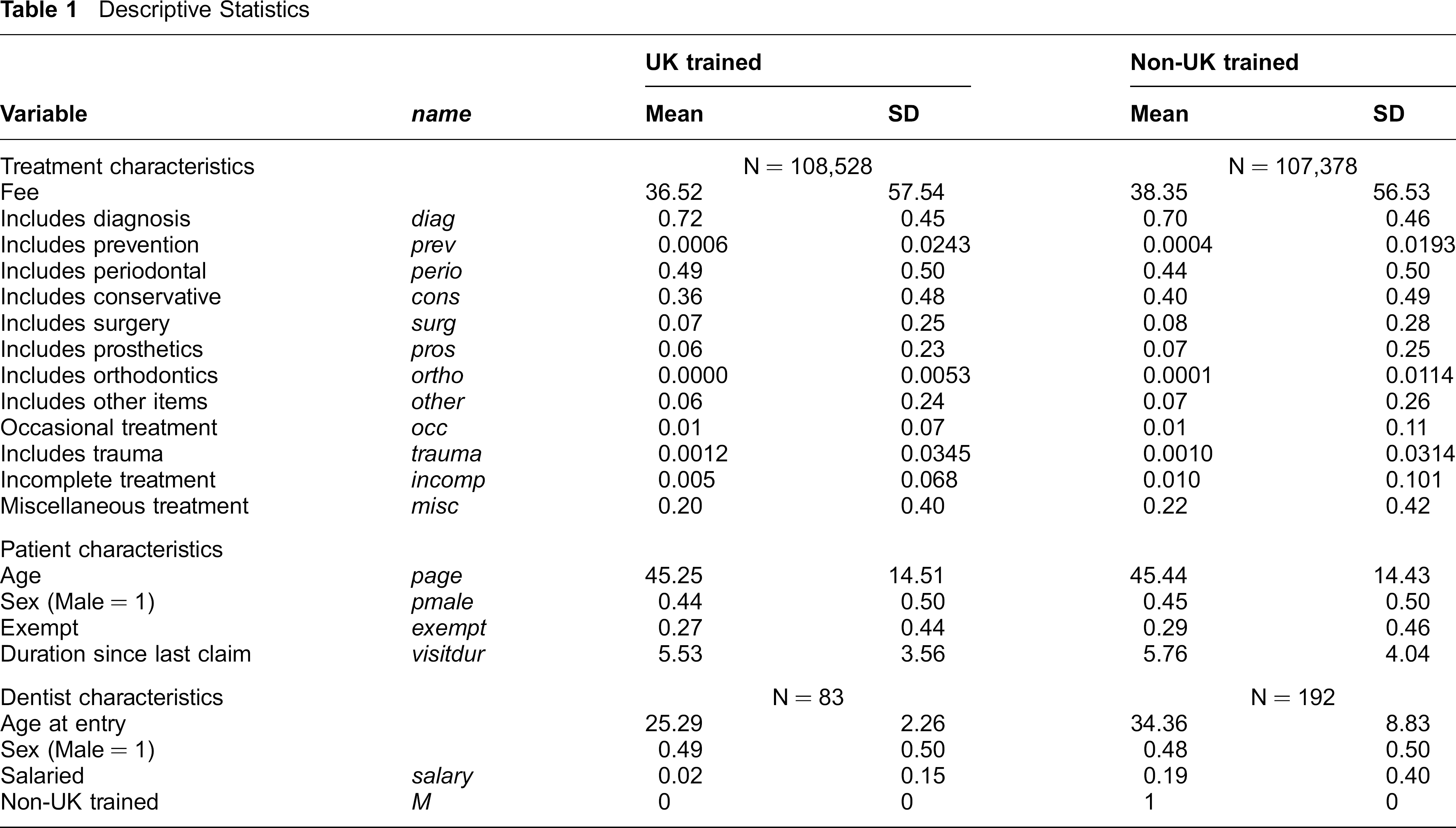
Patients treated by the two groups of dentists are very similar in terms of their age, gender, exemption status and duration since their last visit.
The fees in the SDR are organized into several broad treatment categories within which there are many individual treatment items. We created dummy variables to indicate whether the claim included at least one item from each of those broad treatment categories. For example, 72% of claims provided by UK-trained dentists had at least one diagnostic item, which could include one of four different types of examination or many different types of radiographic examination or both. Table 1 shows that the type of treatment provided to these patients is very similar, but there are some differences in the proportion of claims that included at least one diagnostic (examinations and radiographs), periodontal (scaling and polishing), and conservative (fillings) item.
The average age at entry of the non-UK trained dentists was 34, nine years older than UK-trained dentists. UK-trained dentists were more likely to be non-salaried than non-UK trained dentists, perhaps as a result of the Scottish Executive's recruitment initiative.
Figure 3 shows the distribution of claims by deprivation category of the practice, where 1 indicates least deprived and 7 indicates most deprived; 13 it indicates that non-UK trained dentists work in areas of greater deprivation than the UK-trained dentists.
Regression models
Figure 2 suggests that apart from some initial difference, the mean value of claims converges. In order to formally test for convergence, whilst controlling for both observed and unobserved differences between individual dentists and the patients that they treat, we estimate the following regression model:
Distribution of courses of treatment by deprivation category of the practice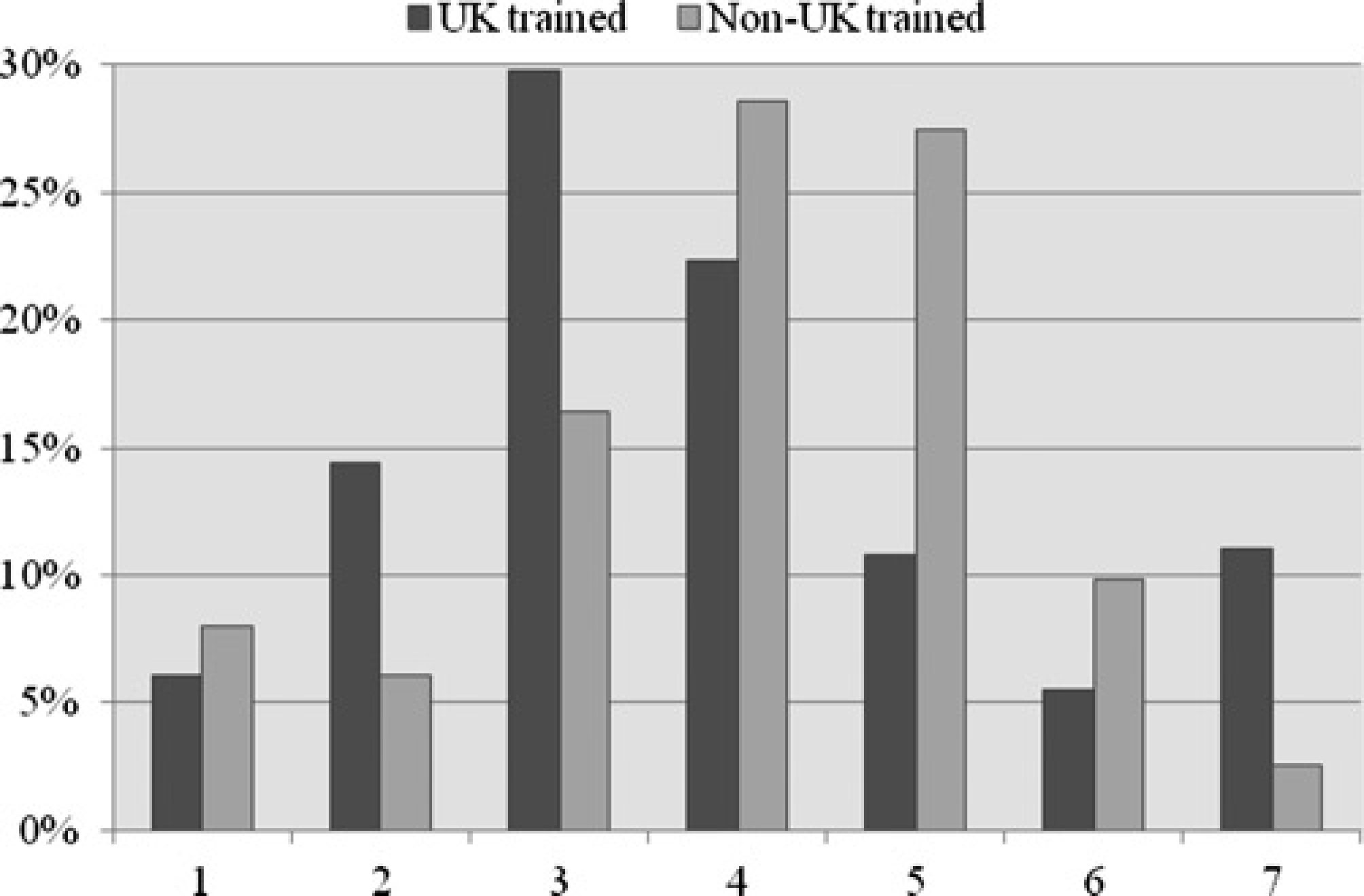

While the fixed effects estimation method is preferred to allow for arbitrary correlation between unobserved dentist effects and observed explanatory variables, an implication of this method is that the coefficient on Mi cannot be estimated directly since a dentist's country of training does not vary between claims. Our analysis therefore focuses on the interactions between Mi and other observable features of treatment (these interactions are set out in columns three and four in Table 2).
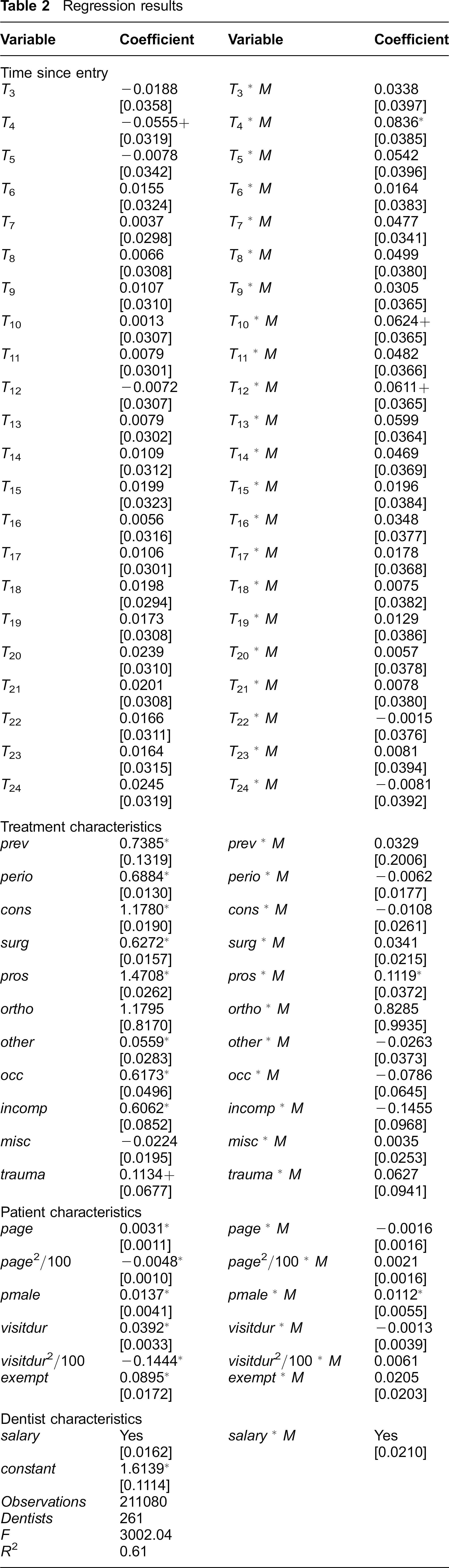
Regression results
Convergence in the amount of treatment per claim between UK and non-UK trained dentists during two time points a < b is measured by δ b - δ a . If δ b - δ a < 0 then there is convergence.
Results
Table 2 presents the results of estimating equation 1. An F-test that all explanatory variables were jointly equal to zero was rejected (F(260,210709) = 11.93, P < 0.001). Dentist fixed effects were significantly different from zero (F(110,210709) = 3002.04, P < 0.001) and a Hausman test rejected the random effects specification. Standard errors, which appear in parentheses below the relevant estimate, are corrected for both heteroskedasticity across dentists and within-dentist correlation using robust cluster variance estimation. Although not reported in Table 2, the regression included dummy variables for the deprivation category of the dentist's practice and the NHS Board in which the practice was located to control for socio-economic and regional variation.
The hypothesis that the coefficients on the interactions between training location and the treatment category indicators are jointly equal to zero is not rejected at the 5% significance level (P = 0.059). In terms of individual coefficients, the only significant difference between UK and non-UK trained dentists is for prosthetic treatment: non-UK trained dentists provide significantly more treatment for patients who receive some form of prosthetic treatment (11.19%, P = 0.003) compared with UK-trained dentists.
While UK-trained dentists provide exempt patients with 8.95% more treatment than non-exempt patients (P < 0.001), the interaction term shows that there is no significant difference between UK and non-UK trained dentists in the way they treat exempt and non-exempt patients.
In terms of the standard patient controls, only the interaction term on the patient's sex is significantly different from zero. This suggests that, relative to female patients, male patients receive significantly more treatment from non-UK trained dentists than from UK-trained dentists (1.12%, P = 0.043). While the individual coefficients are not reported in Table 2, F-tests suggest that non-UK trained dentists provide significantly different treatment to UK-trained counterparts according to deprivation category and (separately) NHS Board in which they practise.
The value of the treatment per claim provided by UK and non-UK trained dentists differs significantly during the sample period: an F-test that the interaction terms on the dentist's tenure are jointly equal to zero is rejected (P = 0.001). Figure 4 plots treatment experience profiles for both UK and non-UK trained dentists using the coefficients on the experience variables and shows that the difference between UK and non-UK trained dentists diminishes over time and is largely eliminated within two years of practice. During the first six months of practice, the value of treatment provided by both UK- and non-UK trained dentists increases, which is likely to be a result of the claim process. Seven months after entry, non-UK trained dentists provided 4.77% (P = 0.057) more treatment than their UK-trained counterparts. This difference increased to 6.24% (P = 0.013) in month 10, and then started to decrease and approach zero (-0.15%, P = 0.038) in month 22. These results are robust to different sample and model specifications (for detailed estimation results see 14 ).
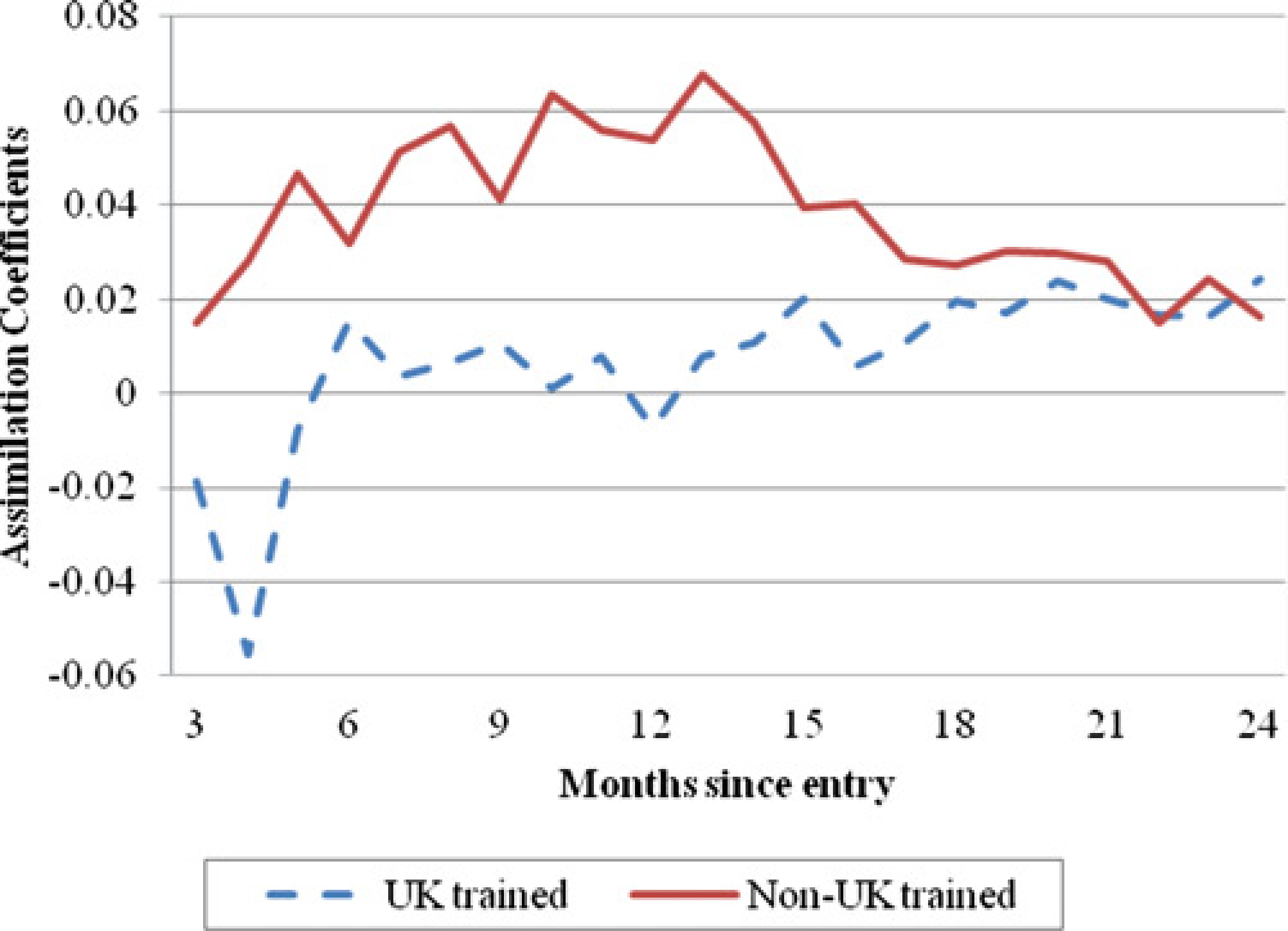
Predicted treatment experience profiles for UK and non-UK dentists
Discussion
There are several features of training for health professionals in the UK that are distinct from other training markets. First, training health care workers requires relatively large, long run and specific investments by several institutions and the trainees themselves; undergraduate and vocational training costs in Scotland are estimated at £250,000 per trained dentist. 9 Second, a key objective of the public sector in the UK is to deliver health care services, which means that the public sector is the purchaser of both training and trained labour. Third, the duration of health care training means that unanticipated periods of excess demand for health care services gives rise to rationing through either quantities (in the NHS), prices (in the private sector) or both, and these cannot be quickly resolved.
Taken together, these features provide policy makers with an incentive to substitute foreign-trained for domestically trained workers. However, such substitution naturally gives rise to concerns that health professionals who have received different training are not familiar with the health needs of indigenous patients or preferred practice methods. The evidence reported in this article may give some comfort to patients and policy-makers alike: whilst the use of non-UK trained professionals in this setting does contribute to some variation in treatment received by patients, the effect is modest and transitory.
While this is, to the best of our knowledge, the first estimate of the variation in the value of treatment provided by UK and non-UK trained health professionals, policy makers are likely to be concerned about several other dimensions of treatment; in particular, differences in the quality of treatment between UK and non-UK trained dentists. The Scottish Dental Reference Service helps to monitor the standard and quality of NHS dental treatment by inspecting the patient's mouth either before treatment is carried out or after they have received treatment. This information, in combination with the data reported in this paper, could be used to examine differences in the quality of treatment between UK and non-UK trained dentists.
Footnotes
Acknowledgements
We would like to thank Frank Windmeijer and participants at the Health Economics Study Group (HESG) Meeting, LSE, 6–8 January 2010 for helpful comments and suggestions.