
Abstract
Integrated care is central to current health care reforms as policy makers and practitioners struggle to address fragmentation of care planning and delivery. However, those pursuing integration have failed to appreciate the complex nature of fragmentation. We seek to bring some much-needed clarity to current debate by considering fragmentation as a ‘wicked problem’ requiring a locally driven and multifaceted approach to integration.
Introduction
Integrated care is a central theme in current health care reforms as policy makers and practitioners struggle to better coordinate care around the needs of patients, improve patient outcomes and connect the health care system with other service systems, such as long-term and social care. 1
This focus on integrated care is not new. It stems from concerns over fragmentation of care that patients experience in many ways, including gaps in care when transferred between institutions and duplicated interventions.1,2 Such fragmentation may occur between different professionals in primary care, between hospital and community services and across health and social care.
In 1973 Rittel and Webber published a paper examining ‘Dilemma's in a General Theory of Planning’ 3 in which they argued that complex social problems – like fragmentation– cannot be definitively described and have no clear, objective answer. Nearly forty years later their arguments remain relevant. A number of integration initiatives have focused on reducing fragmentation (for instance, ‘integrated care pathways’), but have failed to appreciate the complex nature of fragmentation; lacked clarity about what they are addressing and why; and rarely appreciated the way in which the context of such initiatives shapes integration. Services remain fragmented and ill-equipped for patients with complex needs.
Fragmentation as a wicked problem
Fragmentation of care can be thought of as a ‘wicked problem’ in that it is a longstanding and complex social problem for which it is difficult to produce a definitive formulation.3,4
Like other health care problems, the general increase in fragmentation reflects the increasing complexity of the health care system 5 and increasing specialization. 2 As diagnostic taxonomies and treatment opportunities have expanded, the challenge of coordinating care has increased. As a result, it is now ‘less apparent where problems lie and less apparent where and how we should intervene’ 3 (p159). Planners need to adopt a different approach to thinking about and resolving fragmentation that shifts away from an ‘idealised’ approach to health care planning, characterized by objectivity and predictability, and involving a series of ‘choice paths’ oriented to reaching a preferred solution.5–7 We describe a more nuanced approach to understanding fragmentation and integrative approaches to resolving it.
The need for a system perspective
Fragmentation is complex in that it is not owned (or caused) by any one part of the system, but comes as a result of limited cooperation between those providing health and care.1,2 Hence, like every wicked problem, fragmentation can be considered to be a symptom of another problem elsewhere in the system. 3 Hence there is no natural focal point for those addressing fragmentation, but rather a configuration of relationships, structures and operating arrangements between the different components of the system. The level at which fragmentation is addressed therefore depends less on logical models than on a careful analysis of services and the problems experienced by patients who use them.
Different types of integration seek to align clinical, managerial and service user interests and coordinate the work of professionals, teams and organizations (Table 1). Simply focusing on one part of the health care system is unlikely to bring about change. For instance, focusing on organizational integration may not, by itself, improve care for patients 8 or change the way doctors practise medicine. 9 Underpinning clinical and normative changes in teamwork and care delivery are also required. However, current responses to fragmentation tend to be limited, with interventions tailored to small parts of the health care system; attending to one or two levels 2 (such as the pathway from primary to secondary care); and focusing on specific disease (such as diabetes). The result is continued duplication and discontinuity.
Types of integration
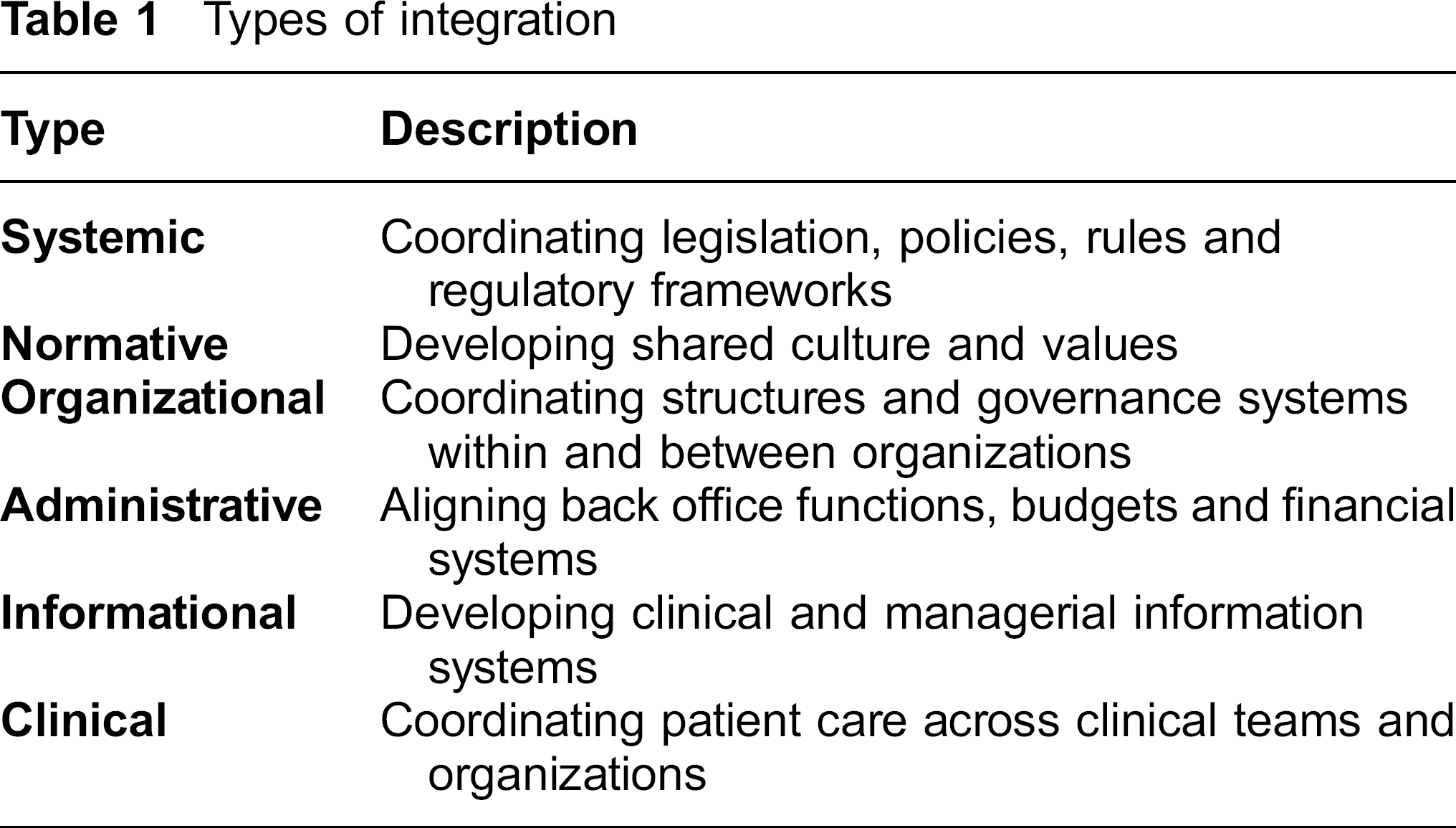
Across the system, different groups and interests are potentially involved in integrating care (for instance, patients, professionals and policymakers). This means that judgements about perceived benefits of integration are likely to differ widely and be focused on whether an initiative is thought to be ‘good’ or ‘bad’. For instance, a two-year evaluation of 16 Integrated Care Pilots in England found that staff reported (mostly process-related) improvements in care, but that patients did not share the same sense of progress. 10 Researchers concluded that the ‘integrative actions’ they observed (e.g. reducing falls in over-60s) were driven by professional rather than patients’ concerns. 10
Fragmentation as multi-dimensional
Fragmentation is widely recognized, particularly in relation to patients with complex problems.1,11,12 However, it is often unclear exactly where the ‘problem’ lies or how best to intervene.’ It defies close definition.10,13 This is because fragmentation – like many problems in health and social policy – is multi-faceted, has ‘fuzzy boundaries’ and requires political judgement to find a way forward.3,5 What follows is that the judgements that people make about resolving fragmentation shape what the problem is or, as Rittel and Webber say, ‘the formulation of a wicked problem is the problem!’ 3 (p161). For example, current reforms in England emphasize the need for integration to achieve ‘efficiency savings’ and, in doing so, frame fragmentation as a problem of ineffective use of resources.
Because fragmentation is multidimensional there are lots of possible resolutions: ultimately ‘anything goes’ 3 (p164). Integrated care is the current lingua franca of health care policy, hailed as a panacea for fragmented health care systems.
Like fragmentation, integration can take many forms. 8 The focus of current reforms is on reshaping the way in which combinations of primary, secondary, community and adult social care services are organised and delivered (Table 2).
Examples of attempts to address fragmentation of care services
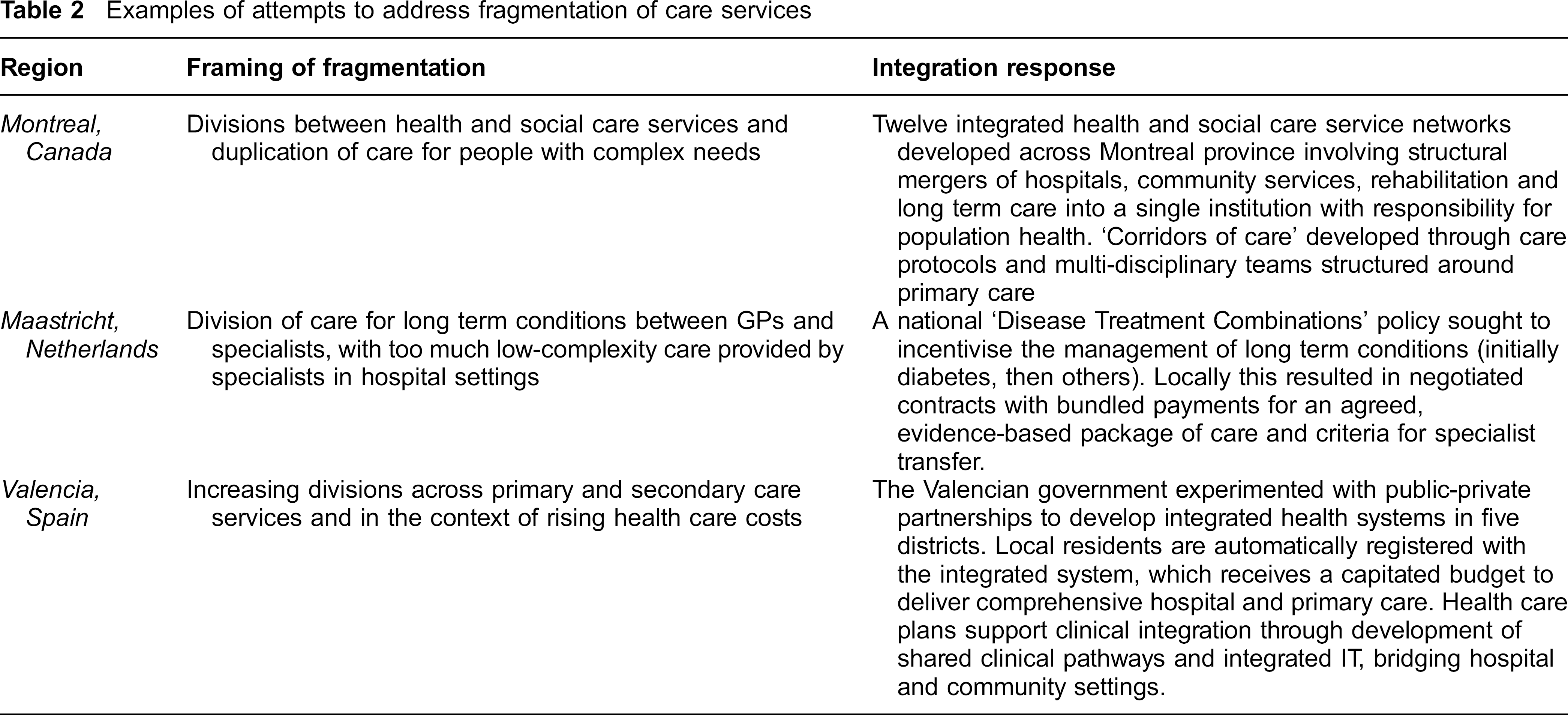
Work to improve integration involves inter-related integrative processes, some focused on systems and structures, others on less tangible aspects such as teamwork (Table 2). This interplay is vital because, ultimately, all parts are connected. For instance, system-level integration is important in shaping national/ regional policy, enabling regulatory requirements to shape the environment in which integration happens (see e.g. examination of how Canadian legislation constrains integration 14 ). However, organizational, administrative and/or clinical changes are needed to operationalise integration ‘on the ground’ (for instance, underpinning work within teams to align incentives and coordinate care around patient needs). 15 Furthermore different types of integration are likely to reinforce the effect of the others (for instance, integrating administrative processes can significantly aid integration of clinical services into a single process 16 ).
Re-solving fragmentation in context
Whilst there is some evidence that integration can help to address problems of fragmentation (see above), it is unclear which integrative activities work most effectively to address fragmentation in different contexts. This is because one cannot fully understand fragmentation – and what to do about it – without first knowing the circumstances in which it has evolved. 3 Because these circumstances are unique, so every wicked problem is unique. 3 What follows is that fragmentation needs to be addressed through locally-adapted ‘integrative activities’.
Efforts to integrate care are mediated by local context and the views of local actors. 9 For instance, although policy makers have the power to enact policies and legislation to support integrated care, they have less control over how these are put into practice. This is not a distinctive feature of policy on integrated care: it affects all policies. What it means for integration is that different regions have different starting points which drive different approaches (Table 2).
Integration is on-going
There are no ‘off the peg’ solutions for fragmentation and there is no ultimate a priori test of a solution. Rather fragmentation has to be resolved, ‘over and over again’ 3 (p160), as the actors and institutions change and evolve. Integration is therefore a process.
From this perspective, it is unsurprising that so many studies fail to provide conclusive findings about integration. In contrast to mathematical or mechanical problems (where analysts test out possible solutions with little or no impact on wider society), every attempt at integration has an impact that cannot be undone. 3 This means that every attempt at integration is significant, leaves traces and muddies the waters of experimentation. Hence there is little opportunity to learn by ‘trial and error’ 3 (p163). What this means is that the evidence is nearly always contestable, no ‘best’ approach to fragmentation is identifiable and the means of addressing fragmentation is therefore always debatable. For instance, studies of US integrated health systems suggest that they can provide high quality care to comparable patients at lower cost than other health care providers. 17 But findings are repeatedly challenged in terms of, for instance, research methods and transferability of findings to non-US health systems. 18
Conclusion
Fragmentation of care needs to be understood as a ‘wicked problem’ that is both complex and context-bound. Acknowledging fragmentation in this way requires that we shift away from a concern with ‘integrated care’ interventions tailored to small parts of the health care system, to consider the root causes across the whole care system. As a result, there is no ‘quick fix’.6,8 A bold approach is needed that embraces the complexity of care rather than putting it aside and engages stakeholders in planning.3–5
Our paper draws heavily on the work of work Rittel and Webber, published in 1973. Many of their ideas resonate with recent moves towards interpretive approaches to policy analysis and to thinking in terms of complex adaptive systems. Many of the papers we cite draw on such work,3–7 suggesting that our arguments are plausible in the current context. We therefore urge all those involved in thinking about, planning, developing and evaluating integrated care to be creative, embrace complexity and focus on improving fragmentation in ways that are relevant to those involved locally in providing and receiving care.