
Abstract
Objectives:
To ascertain if access to cataract surgery is being restricted in England and to describe any explicit threshold criteria.
Methods:
A survey of 151 local commissioners to explore their cataract surgery policy. A literature review identified research evidence about thresholds for cataract surgery. A checklist was devised and applied to the policies supplied by commissioners.
Results:
Almost half (71/151) of commissioners were restricting access to surgery and this included patients with some capacity to benefit. There was wide variation in the scope and content of the 67 policies which were available for review. Almost all (92%) commissioners use criteria that do not reflect guidance or research evidence.
Conclusions:
Patients who could benefit from cataract surgery are being excluded by some commissioners. Variations in policy between commissioners results in inequalities in access.
Introduction
The challenge of assuring a financially sustainable health system, whilst offering universal coverage, is a growing concern in developed countries. The current global economic downturn has increased pressure to contain escalating expenditure. Countries are pursuing different strategies, such as introducing user fees or restricting spending on drugs. 1 In England, the National Health Service (NHS) has to make £20bn efficiency savings by 2014/15.
One of the founding principles of the NHS is that access to treatment should be based on people's need, often interpreted as capacity to benefit. However, it is also recognized that resources are finite and not all health needs can be met. Therefore resource distribution must be prioritized and purchasers of health care have to make difficult decisions about which care to commission, and for whom. 2 Cost-utility analysis, in the form of cost per quality-adjusted life year (QALY), has been widely applied to inform which treatments the NHS can offer: its findings can lead to disinvestment of existing services or to limiting access to those who should benefit most.2–4
The National Institute for Health and Clinical Excellence (NICE) does not usually allow NHS patients access to new treatments that have a marginal cost of £20,000 to £30,000 per QALY, a figure that seems to align with the marginal valuation of a life-year in various programme budgeting categories based on commissioner spending patterns.5,6 Treatment thresholds focus limited resources on those subgroups of the population for whom receipt of an intervention offers the greatest cost utility, though other evidence, including equity and local circumstance, is often also considered. 7 Raising thresholds for elective surgery has been cited as a way the NHS could save money, and recent guidance suggests commissioners consider reducing access to cataract surgery.8,9
Cataract, the leading cause of reversible loss of vision, is caused by lens deterioration. Surgery is the only effective treatment and is generally cost-effective, with estimates ranging from US$245 to US$20,000 per QALY gained, comparable to hip, and more so than knee, replacements. 10 An estimated 17 cataract operations per 1000 population are needed annually among persons over the age of 55 years if medium strict access criteria, that include consideration of quality-of-life, are applied. 11 Cataract surgery is the most common elective procedure undertaken in the UK with 400,000 performed annually. 12
This paper examines whether there is any evidence that local commissioners (Primary Care Trusts - PCTs) in England are using explicit thresholds to determine access to cataract surgery and, if so, to describe what these are. We examine whether thresholds are based on appropriate scientific evidence and exclude only those patients least likely to benefit.
Method
Survey of commissioners
A request was issued to all PCTs in England in May 2011 under the Freedom of Information Act (2000), which gives public bodies 20 working days to respond. The following was asked in relation to cataract surgery: does the PCT have a policy that restricts funding for cataract surgery? and how long has the policy been in place? A copy of the policy was requested.
Two authors independently checked, collated and categorized the responses according to whether a policy was in place or not. Some PCTs had formed consortia. Where a PCT specifically stated it was replying on behalf of others in its consortium, all constituent PCTs were counted as having responded. Where Trusts are part of a consortium but had responded individually, replies were counted individually. Where either no response was received or PCTs stated they had no policy, manual searches were undertaken to see if either the response could be verified or a policy identified.
Literature review
Current best practise in cataract diagnosis, management, treatment and prioritization was determined through a literature search. Studies and guidelines were identified through computerized searches of databases and relevant websites. Manual searches and consulting expert stakeholders were used to locate ‘grey literature’. This yielded evidence on the relevant clinical and cost effectiveness, as well as considerations of equity and prioritization. The evidence was reviewed, categorised and summarized (Appendix 1, available online only at: http://www.jhsrp.rsmjournals.com/cgi/content/full/jhsrp.2012.012023/DC1).
Checklist
A checklist developed against which to assess each PCT's threshold policy. The majority of criteria required categorical answers (yes/no/not stated) but some required free-text. For clarity, the questions were clustered into themes, but with recognition that some criteria may occur in several categories. The draft checklist was reviewed by a senior ophthalmologist specializing in cataract surgery, to ensure the evidence reflected current clinical practise. The finalized list was piloted with four randomly selected PCT policies, the results compared and some minor changes made. The remainder of the policies were then reviewed. The completed checklists for each PCT were compared and any discrepancies discussed until consensus was reached. A descriptive analysis was undertaken and qualitative evidence of unusual or extremes of policy criteria was collated.
Results
Responses were received from 120 (80%) Trusts. Seventy-one policies (47% of PCTs) explicitly restricting access to cataract surgery were identified. Four were excluded, as the policy was under review, patients were considered individually or no copy could be located. The majority had been agreed in 2010 (25) or 2011 (32). Of the 67 policies available (44% of Trusts), 92% contained criteria that follow neither national guidance nor scientific evidence.
Visual impairment
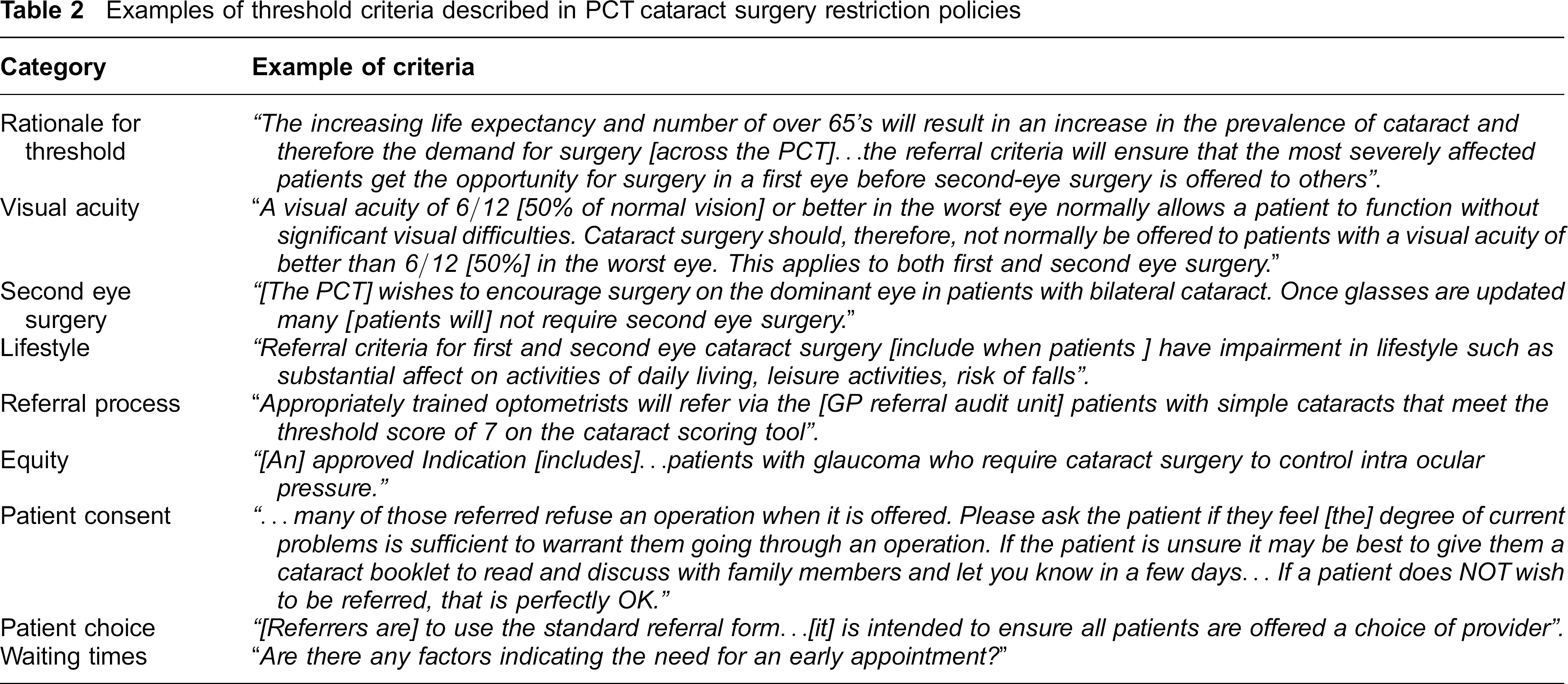
Most Trusts state a minimum level of vision loss that patients must demonstrate before being considered for surgery. Two PCTs use visual acuity as the only indicator (Table 1). Visual threshold levels and criteria ranged widely, with a four-fold difference between the highest and lowest thresholds. Some more complicated thresholds distinguish between combined and single-eye vision (Table 2). Seven trusts specifically distinguish between drivers and non-drivers. Three polices do not give a visual threshold but instead consider visual impairment in combination with lifestyle factors.
Summary of characteristics of assessed cataract restriction policies (N = 67)

n — 65 as two PCTs state they do not take lifestyle factors into account
n — 44 as this is the total number of PCTs that state they allow second eye surgery
Examples of threshold criteria described in PCT cataract surgery restriction policies
Second eye surgery
Two thirds of policies (44) make provision for second eye surgery, with 26 stating it should be sequential. One cluster seems to allow simultaneous bilateral cataract extraction. A quarter (12) apply the same criteria to both eyes. Others make the decision to allow second eye surgery dependent on the outcome of the first: 10 Trusts state that if the vision in the first eye is <60%, then the decision to operate should be taken on clinical grounds. A range of criteria were also identified: for example, two neighbouring PCTs will allow second eye surgery only if the first achieves <60% of normal vision and the second eye has an acuity of <25%.
Lifestyle factors
Almost all (65) policies specify lifestyle factors that determine who is referred for surgery, but the range and number varies widely. Trusts are most likely to take account of cataract affecting the ability to drive, activities of daily living, and ability to work into account, but only three consider the effect on caring responsibilities. The number of factors also varies: one PCT considers only driving impediment, while another assesses the impact on: ability to drive, or to work; activities of daily living; and the risk of falls. Half (32) of policies require a specified visual thresholds and lifestyle infringements to be met; the other half (32) requires either visual or lifestyle impairments to be considered. Eleven policies require the use of specified questionnaires to score the impact of cataract on the patient's lifestyle (Table 3).
Summary of questionnaires (n = 11) specified by policies to be used to score the impact of cataract to determine whether referral to surgery is appropriate
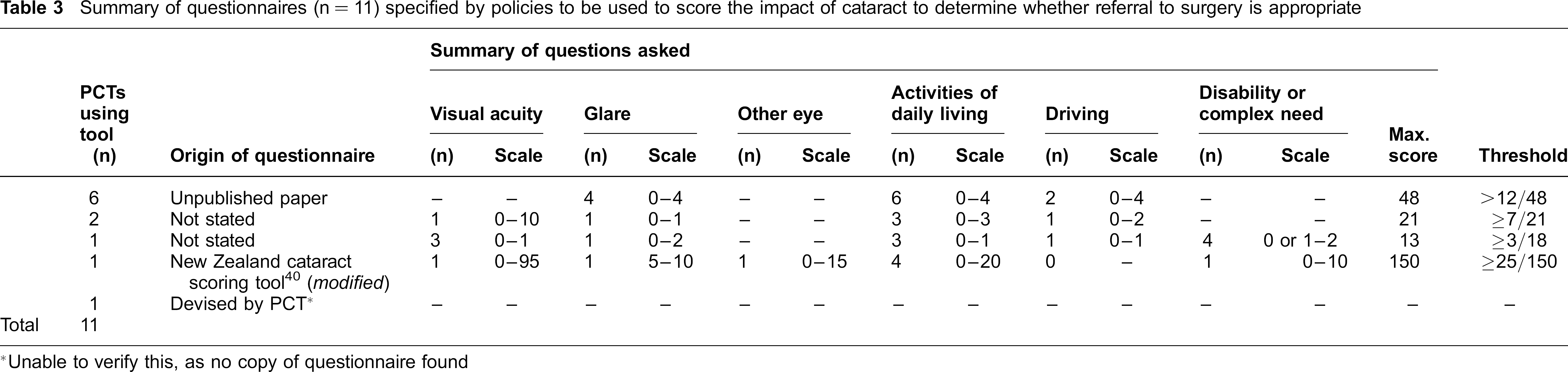
Unable to verify this, as no copy of questionnaire found
Equity
The majority of Trusts (39) state referrals for patients with co-morbidities whose vision may only benefit slightly but where surgery could improve disease management (e.g. diabetes) will be considered. No policy states an upper age-limit for patients, but three make provision for offering general anaesthesia to patients for whom local anaesthesia may not be appropriate. No PCT explicitly allows exceptions to day case surgery, though one asks patients to confirm they are able to self-administer eye drops, or have someone who can do this for them.
Two policies specify any patients undergoing surgery should have stopped smoking at least eight to 12 weeks prior to being added to the surgical list and, if there is no evidence of continuous smoking cessation for at least eight weeks, then the patient may move back to the bottom of the waiting list. Another policy encourages patients to be smoke-free for the eight weeks prior to surgery, though they are not excluded for not succeeding.
Referral process
Most policies do not clearly state who can refer patients for surgery. One in six Trusts triage referrals through a demand management system. One PCT consortium decides on whether a referral is appropriate, whereas in another, GPs can block optometrist referrals. Overall, the referral process varied widely between trusts.
Patient consent
Two thirds of Trusts require the patient to confirm willingness to undergo surgery as part of the referral process. In some cases the patient is required to sign an approval form, in others the referring clinician must verify the patient consents. One Trust specifies consent can only be given after a minimum wait.
Patient choice and waiting times
One Trust liaises with patients to check their choice of hospital but no policy offers patients the choice to transfer to another surgeon if this reduces their waiting time. One Trust specifies a patient should have surgery within three months of referral, and two PCTs ask the referrer to state if there is any reason the patient should be seen urgently.
Discussion
Main findings
At least half of PCTs are restricting access to cataract surgery through clinical thresholds, with many denying treatment to patients with capacity to benefit. In addition, there is variation in the criteria applied to patients in different localities. Despite falling within the generally-accepted QALY range,5,10,13 71 PCTs restrict access to surgery, and a third make no allowance for second eye surgery. The question is whether the restrictions only exclude people where the cost per QALY is in excess of NHS acceptable levels.
If cost per QALY is accepted as the prime criterion for treatment, referrals for surgery should usually be based on considerations of visual functioning, not acuity and the associated quality-of-life. 14 Two Trusts use visual acuity as the only referral criterion and all but three rely on it as a key criterion. A randomized trial of patients with pre-operative vision of half or less than normal, demonstrated that surgery is cost-effective if benefits over the remaining lifespan are considered. 15 Only offering surgery to patients with extremely poor vision may exclude patients with a large capacity to benefit, as patients with 50% vision feel very disabled by the loss. 16
Although there is some evidence that prioritization tools can predict benefit, it is unclear how many PCTs that specify a scoring method use validated tools.17,18 The range of lifestyle criteria considered by Trusts varies considerably. Despite the high economic value of informal care-givers, just three policies acknowledge caring responsibilities, but the majority consider whether ability to work is affected. 19 However, since those over 65 years of age are predominantly afflicted, the majority of patients will be beyond the current retirement age. 11 Two PCTs consider a history of falls, and two fifths take the risk of falls into consideration, even though falls can be substantially reduced by offering surgery. 20 Operating within four rather than 52 weeks represents an incremental cost per prevented fall of £4,390.15,21 There is a strong case for incorporating such benefits into any prioritization process.
Fifty-one PCTs consider a person's need or wish to drive. To hold a licence in the UK, drivers must be able to read a number plate at 20 metres distance, an approximate binocular visual acuity of 60% of normal vision. 22 However, visual acuity can be poor predictor of ability to meet the legal driving standard. 23 This suggests PCTs that include driving as a criterion, should base their assessment on a patient's actual ability to pass the number plate test.
Guidelines recommend patients should not wait more than two months for surgery, but only one PCT recommends a maximum waiting time. 24 Poorer outcomes are associated with delaying intervention: patients with <50% vision should wait no longer than three to 12 months; those waiting over six months experience reduced vision and quality-of-life, and increased rate of falls and car accidents.15,25 By contrast, expedited (within one compared to 12 months) surgery is associated with increased activity, confidence and quality-of-life and generates a conservative cost of £13,172 per QALY, assuming quality-of-life does not decline for someone with an un-operated cataract. 15
In addition to cost-effectiveness, the NHS also seeks to take equity into account when deciding which patients could benefit from treatment. No policies include age-related criteria, despite studies indicating that surgery may not be cost-effective in older age groups. The incremental cost-effectiveness of first eye surgery is estimated at US$38,288 per QALY for older patients (mean age 78 years) previously estimated to only have a small probability (<30%) of benefitting from surgery, meaning its cost-effectiveness is borderline from an NHS perspective. 26 The capacity to benefit from surgery seems higher at younger ages, with patients aged 60 to 69 years over three times more likely to achieve a ≥50% vision than those >80 years. 27 Nevertheless, significant improvements are found in care home residents, who tend to represent an older and frailer cohort. 28 Patients with co-morbidities whose disease management, not vision, may be improved by surgery are generally not restricted from receiving treatment, which is in line with specialist guidance. 14
Three PCTs consider smokers differently. Although abstaining from smoking in the four to six weeks prior to general surgery reduces the risk of wound infection, there is no conclusive evidence of poorer outcomes following cataract surgery among smokers. 29 Restricting access to services based on smoking status raises ethical concerns.
Two thirds of PCTs currently require patient confirmation that they would proceed if offered surgery. In 2007/8, hospitals lost £100 per patient in revenue for missed appointments. 30 Obtaining informed consent from patients reduces the risk of unwanted operations being carried out, and maybe also the likelihood of patients missing appointments. Ten trusts operate referral management centres to pre-approve surgery requests. Although the Department of Health promotes this, it is not clear these centres are effective, and concerns have been expressed they result in patient flows being controlled by managers rather than clinicians.31,32
Strengths and limitations
First, we cannot be sure that those PCTs for which no policy was identified definitely do not have one. It is therefore possible that our results are an underestimate, and more PCTs are restricting access to cataract surgery than our study suggests.
Second, the heterogeneity of policies made them difficult to compare. By presenting a quantitative descriptive analysis, we seek to offer clear comparisons between policies, but we also show some examples of unusual practice used to inform the surgery threshold.
Third, it is not clear whether the main purpose of a threshold is simply to reduce the number of operations, and thereby expenditure, or to prioritize treatment for those patients that have most capacity to benefit. Although this latter consideration should principally be driving access to surgery, we cannot be sure that some PCTs are simply trying to manage costs.
Fourth, although the majority of PCTs have developed their policies recently it is not possible to say whether these policies are new, or are revisions to earlier policies. The peak in policies developed in 2010 and 2011 suggests that the need to secure rapid spending reductions may have precipitated the development of such policies.
Fifth, we were reliant on the quality of the information received from PCTs. Since this was variable, it is hard to draw direct and detailed comparisons. In addition, PCTs’ functions are currently transferring to GP-led commissioning groups. It is therefore likely that policies will change, as the new commissioning arrangements are implemented. This state of flux makes it hard to assess definitively the level and restrictiveness of the policies in practice. In addition, the extent to which these policies are adhered to in each locality is not clear.
Finally, although our research did not examine implicit rationing, it is important to note it may be occurring, thereby also preventing patients accessing services, even where no policy exists. For example, long waiting times may encourage patients to seek privately-funded treatment. A specific unresolved issue is whether referral management centres reinforce or undermine explicit rationing policies.
Implications
Although the NHS is encouraging the use of clinical thresholds, commissioners must clearly demonstrate either that a procedure is of low clinical value, or which patient groups could benefit from treatment. 33 Given the high prevalence of cataract, the availability of a safe, cost-effective treatment, and the existence of robust guidance and heterogeneity in both the form and content of PCT cataract referral policies is of concern.
It is well-documented that the visual function, not the visual acuity, predominantly affects the level of quality-of-life that a patient experiences. The range of criteria applied by PCTs are often not specific enough to be of practical use in managing referrals. There is, therefore, a need for guidelines to provide a standardized set of criteria by which visual function should be assessed.
It is difficult to reconcile our findings with the NHS principle of ‘equal access for equal need’. The results highlight tensions between the ambition to deliver a national standard of care and the task of adhering to local priorities and budgets. Our findings raise questions about whether similarly variable thresholds are being developed for interventions where the evidence of benefits may be less straightforward or more subjective.
Given the continuing financial pressure the NHS is under, and the devolution of commissioning to smaller bodies, it is important to consider the risks of increased variability in treatment access depending on where a patient lives. Given readily available evidence is not being used, and the suggestion that cataract surgery should be reduced or even stopped, there is a need for the development of national guidance that outlines which groups could benefit from surgery, and also where local discretion would be appropriate.
Conclusion
There is evidence that PCTs are limiting access to cataract surgery. Some restrictions may be necessary if the NHS is to maximise the health gains it secures with its finite budget. However, there are wide variations between localities in the applied thresholds, giving rise to the potential for major inequalities in access. Furthermore, we demonstrate the applied limitations reflect neither national guidance nor the scientific evidence base, and patients with capacity to benefit are being excluded.
Footnotes
Acknowledgements
We thank Graham Duguid for his specialist input and Christopher Millett for comments.