
Abstract
ABSTRACT
In 2005, the south-east Wales Cancer Network obtained support from Macmillan to fund a coordinator for a three-year project to improve the care that dying patients receive in care homes (nursing) across south-east Wales by the implementation of the integrated care pathway (ICP) for care in the last days of life.From the project outset it was clear that to gain commitment to the project from the care home senior staff they needed evidence that the ICP would improve the care they delivered to patients at the end of life. This was obtained through undertaking a retrospective baseline audit examining the documentation of care provided for dying patients in care homes, implementing any changes required and then re-auditing to review improvements.From the evidence and recommendations, changes were implemented including ongoing education for all levels of care home staff. The audit was repeated one year later to measure whether these changes had proved to be beneficial.This article provides an overview of the completed audit cycle results whilst outlining the changes that were implemented and highlighting some recommendations for the future. Throughout the article when it refers to a ‘patient’ this also refers to 'residents', ‘service users’ and ‘clients’.
BACKGROUND
It is widely accepted that palliative care should be part of the care extended to patients who have a chronic progressive disease and for whom a cure is not possible 1 regardless of the care setting. 2 There have been projects in the UK and north Wales addressing the palliative care education needs of care home staff, but none previously in south-east Wales.
The South East Wales Cancer Network, with the support of Macmillan Cancer Support, instigated a project to coordinate the progression of the implementation of the All-Wales integrated care pathway (ICP) for the last days of life into care homes (nursing) across the network area (November 2005 to November 2008). The role of the project coordinator is to create a system that develops, supports and sustains the implementation of the All-Wales ICP into care homes.
The National Council for Palliative Care (2006) 3 states that five deaths in every six are of people aged ≥65 years, and one in every five of all deaths take place in a care home. This establishes the need for ensuring that care home staff are educated and equipped to care for patients at the end of their life.
The Welsh Health Circular (WHC) (2006) 030 4 formally endorses the All-Wales ICP following the ministers commitment to ensure that health care encompasses the needs and wishes of those at the end of life.
The National Institute for Health and Clinical Excellence (NICE) recommends ‘Staff providing general palliative care should be trained in identifying needs of patients and carers and in general principles and practices of palliative care.’ 2
All of these organizations support the project with its aims for ICP implementation.
All-Wales ICP care home project aims:
To coordinate, develop and improve care of the dying in care homes throughout the network area by implementation of All-Wales ICP for the last days of their life To assist in facilitating the implementation of the ICP into participating homes through negotiation with local palliative care providers To create a system that develops, supports and sustains implementation of the All-Wales ICP To develop an education facilitated learning pack on the concept and documentation associated with the All-Wales ICP in conjunction with local specialist palliative care providers To carry out a baseline audit to examine the documentation of care provided in care homes for dying patients, prior to implementation of the All-Wales ICP To evaluate the current level of palliative care knowledge and skills held by care home staff participating in the project To assist in facilitating the implementation of the ICP into participating homes through negotiation with local palliative care-providers To evaluate effectiveness of education by completing the audit cycle one year on from the baseline audit.
This article will focus on the audit that was completed in September 2007, at the end of year two of the project. A baseline review was initially completed as a method of examining current practice. This baseline pre-implementation audit was carried out, prior to education on the All-Wales ICP to examine the documentation of care provided in care homes for dying patients in their last days of life. The audit of documented care during the last days of life is a measure of the quality of documentation. It must be stated that with clinical governance in practice if care is not documented, then in essence, care cannot be measured and the intervention ‘did not take place’.
METHODS
Three ‘champion homes’ were nominated from each local health board (LHB) (January 2006). This was achieved by sending written requests to each nurse director from the 10 LHBs in the South East Wales Cancer Network area. They were asked to collaborate with their local trusts and palliative care clinical nurse specialists in order to decide which care homes would participate.
The care pathway coordinator undertook visits to these care homes between February 2006 and August 2006. The last five sets of deceased patient records were requested in each care home. This proved to be challenging at times due to accessibility of notes, or incompleteness of information, e.g. medication charts.
Baseline pre-audit conclusion
The audit demonstrated poor recording of care. The conclusions from the pre-audit concurred that:
There was poor evidence of communication between the care home staff, patients, relatives, general practitioners, hospital staff and other involved professionals There was evidence of poor symptom control of dying patients in care homes Care homes would greatly benefit from a programme of ‘facilitated learning’ on the foundations in palliative care incorporating the use of the All-Wales ICP for the last days of life.
Developments and changes implemented
Changes were implemented with the collaboration of the care home matrons, LHBs and the palliative care clinical nurse specialists including:
Analysis of formal education needs of care home nurses among the champion homes was carried out. Education subgroup was formed. Standardized ICP education pack was developed. Formal teaching sessions were carried out. ‘Train the trainer’ syringe driver training was set up and implemented Matron forums were established Informal training and support sessions, including post-death debriefing sessions were delivered.
RE-AUDIT (SEPTEMBER 2007)
To complete the audit cycle and evaluate effectiveness of the implemented changes and developments, a re-audit was undertaken between 1 August and 12 September 2007 using the same method as the baseline audit.
Table 1 outlines the number of nursing homes visited and the number of deceased patient records audited from each of the LHBs in the South East Wales Cancer Network area in both the pre- and post-education audits.
Number of nursing homes visited and deceased patient records audited from each local health board areas in both the pre- and post-education audits
The audit tool used was based on the ‘Welsh Collaborative Care Pathway Project’ tool 2000. Results were then collated and analysed using an excel database.
RESULTS
All the care homes visited willingly participated in the audit. In all, 130 sets of notes from 29 care homes were reviewed over the six-month period in the pre-audit and 133 sets of notes from the same 29 care homes were reviewed in the post-audit. Six ‘champion homes’ did not have five sets of notes available for the pre- and post-audit (between one and four sets of notes available to audit). All care homes but one uses ‘paper’ notes/records, and one used electronic.
In the pre-audit, four of 29 care homes stated that they used the All-Wales ICP (questionnaire data). The first care home had used one ICP but the documentation was incomplete and none of the staff had had any formal education. The second care home had used one ICP. The medical assessment had been completed but the nursing assessment had not. The third care home had not used the ICP in any of the reviewed notes. They had suggested its initiation once but the general practitioner (GP) felt it was too early (patient had died three weeks later). The fourth care home had used the ICP for one patient for 12 h prior to death. The ICP had been commenced in three of 93 patient records (of those patients who died in the care home). Therefore, ICP usage was found to be 3% in the pre-audit.
In the post-audit, 10 of 29 care homes had used the ICP. Twenty-eight ICPs had been used and completed. The average length of time patients were on the ICP prior to death was four days, ranging from a few hours to 14 days. Two ICPs were commenced and stopped when patients did not die and recommenced in one case a few hours before death. In the second case the day before the patient died.
The omissions from the 28 used ICPs were as follows:
The ‘after death’ page was not at all used in four ICPs and others were not fully completed A few staff continued writing in kardex and duplicating in ICPs Not all ICP ‘as required’ medications were prescribed; nothing was documented on the variance as to why only certain medications from ICP guidelines were prescribed.
The findings included:
One patient had no analgesia prescribed (3.5%), was agitated and had sedative prescribed. Eight patients on the ICP did not have antiemetics prescribed (28.5%); none of these had documented sickness as a symptom. Three patients on the ICP did not have sedatives prescribed (11%); none of these had documented agitation as a symptom. Seven patients on the ICP did not have an anticholinergic prescribed (25%); three of these patients had noisy secretions documented as a symptom. Variance sheets were not appropriately completed, i.e. used inappropriately as a communication sheet. ICP document pages were not filed together, therefore were difficult to follow/find pages in some cases.
ICP usage had gone up in the post-audit from 3 to 31% (Table 2).
Integrated care pathway (ICP) usage pre- and post-audit
*Local health board areas that did not have an ICP document in use at the time of the audit
Demographics
In the pre-audit of the 130 patients, 86 (66%) were female and 44 (34%) were male. In the post-audit, 86 (65%) patients were female and 47 (35%) were male (Figure 1).

Distribution of sex of all deceased patients pre- and post-audit
Age distribution
The majority of those who died were over 80 years of age in the pre-audit with the average age being 86 years. In the post-audit, the average age was also 86 years, reduced by the higher number in the under-70 age group (Figure 2).
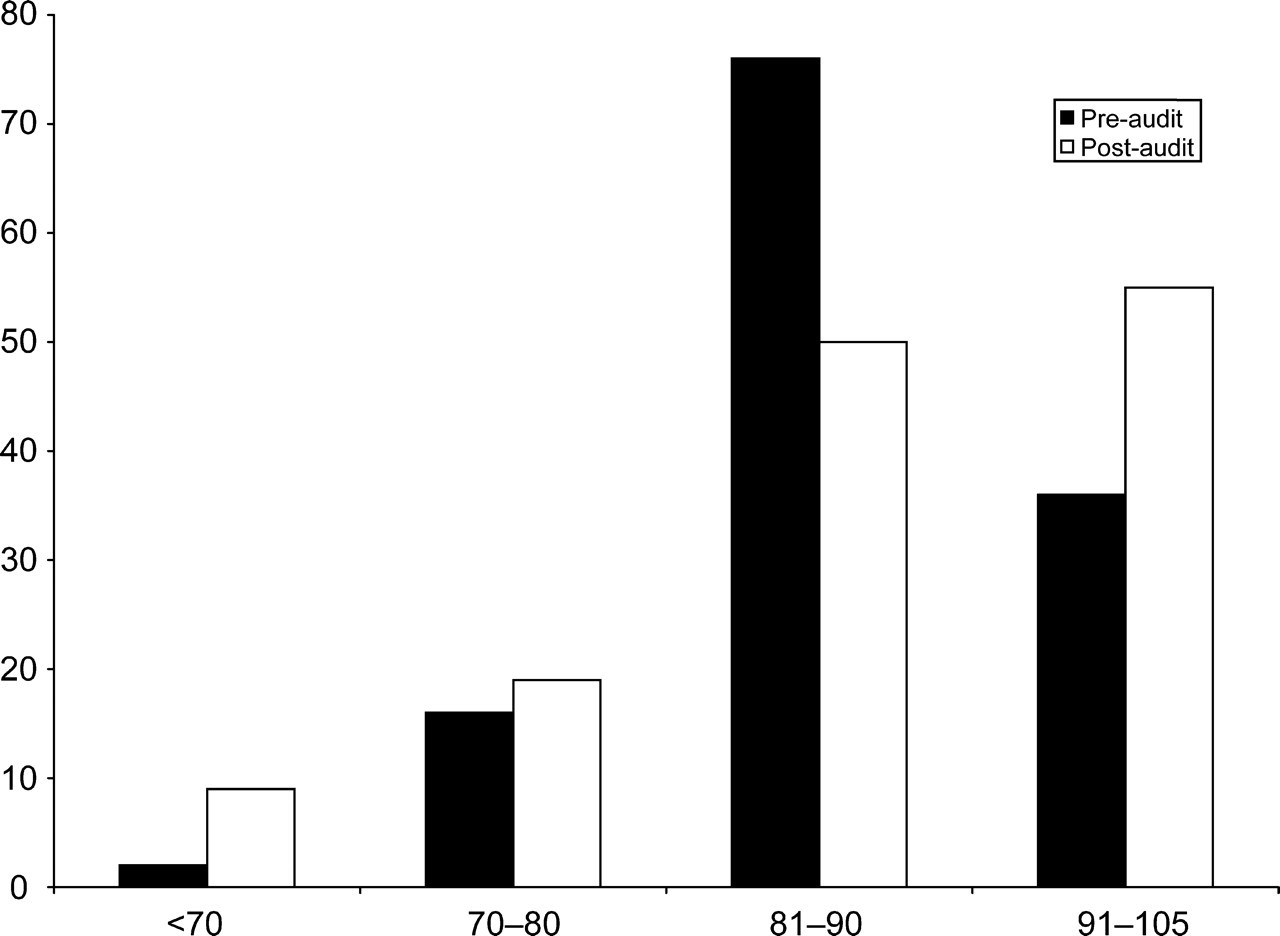
Distribution of ages of all deceased patients pre- and post-audit
Place of death
In the pre-audit, 37 patients (28%) died in hospital after being transferred from the care home, 93 (72%) died in the care home itself.
Length of stay in the hospital from date of transfer to date of death ranged from 1.5 h to weeks It was documented that three of 37 (8%) died on the All-Wales ICP in the hospital In the majority of cases, it was very unclear why the patients were admitted to hospital or what happened in the hospital Average age of residents who died in the hospital was 86 years (excluding one 56-year-old male).
In the post-audit, 43 (32%) patients died in the hospital after being transferred from the care home. Figure 3 demonstrates this in each LHB.
Length of stay in the hospital from date of transfer to date of death ranged from hours to over six weeks Of the 43, five (12%) died in <12 h, 12 (28%) died in 12 h to one week. Time was not clearly documented in other cases In the majority of cases, it was very unclear why the patient was admitted to hospital or what happened in the hospital Average age of patients who died in the hospital was 86 years.

Distribution of place of death pre- and post-audit. RCT, Rhondda Cynon Taff
Diagnosis
In the pre-audit, 17 of the 130 patients (13%) had a diagnosis of cancer. In the post-audit, 28 of the 133 patients (21%) had a diagnosis of cancer. Other diagnoses ranged from dementia, stroke, Parkinson's disease, heart failure to ‘old age.’
Evidence of communication
Pre-audit showed that documentation of communication with any patient or family member regarding wishes about hospital admission was negligible. There was very little documented evidence from the hospital on interventions carried out and no documentation of communication from the hospital on actual date of death.
Post-audit showed that documentation of communication appeared better in cases and overall seemed to be more ‘systematic’. There was still little documented record from the hospital on interventions carried out and little documentation of communication from the hospital on actual date of death.
GP's were informed in 125 of 133 (94%) post-audits (88.5% in pre-audit) that the patients were deteriorating. There was documented evidence that families were informed in 70 of 133 (53%) post-audit (44% in pre-audit) cases that the patients were deteriorating.
There was documented evidence that the GP was contacted regarding death in all cases where the patient died in the care home as the GP was the death verifier and certifier.
Of the 37 patients who died in the hospital in the pre-audit, there was no evidence that the GP had been informed of their death: it is assumed that the hospitals do this. The same applied for the 43 patients in the post-audit who died in the hospital.
Of the eight (6%) post-audit (10 [8%] in pre-audit) patients who had any type of clinical nurse specialist involvement, none had been contacted regarding death according to documentation.
Resuscitation status
In the pre-audit, 44 of 130 (34%) patients had documentation to support ‘allowing natural death to occur’. In the post-audit, 62 of 133 (46%) patients had documentation to support ‘allowing natural death to occur’.
Spiritual support
In the pre-audit, 67 of 130 had their religious denomination recorded (51%) and there was no documentation to support any level of spiritual support. In the post-audit, 71 of 133 had religious denomination recorded (54%), but those where the ICP was used had documented evidence of spiritual care and support.
Primary symptoms documented
In the pre-audit, 22 patients had it documented that they had pain as a symptom. Ten of those patients had analgesia prescribed. In the post-audit, 12 patients had pain recorded as a symptom and all had analgesia prescribed (Figure 4).
Patients prescribed analgesia for pain pre- and post-audit
In the pre-audit, nine patients had agitation recorded as a symptom and four (44%) of those had a sedative prescribed. In the post-audit, 16 patients had agitation recorded as a symptom and nine (56%) of those had a sedative prescribed (Figure 5).

Patients prescribed sedative for agitation pre- and post-audit
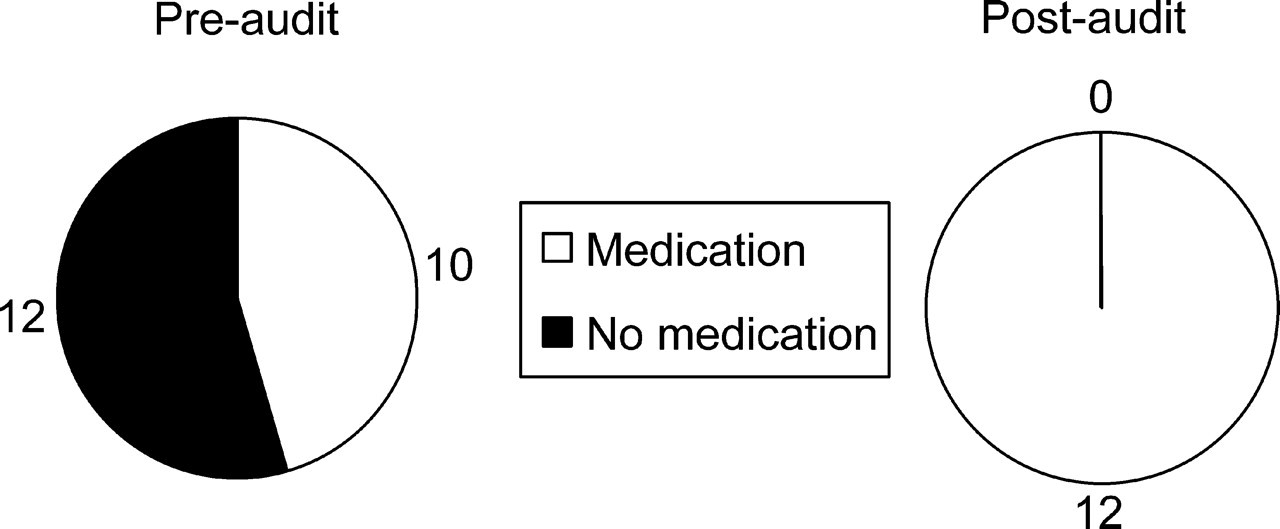
In the pre-audit, seven patients had a recorded symptom of sickness but none of those seven had an antiemetic prescribed. In the post-audit, seven patients had a recorded symptom of sickness and two of those had an antiemetic prescribed (Figure 6).

Patients prescribed antiemetic for nausea and vomiting pre- and post-audit
In the pre-audit, six patients had a recorded symptom of respiratory tract secretions; none of the six had an anticholinergic prescribed. In the post-audit, 13 had the symptom recorded and six had an anticholinergic prescribed (Figure 7).
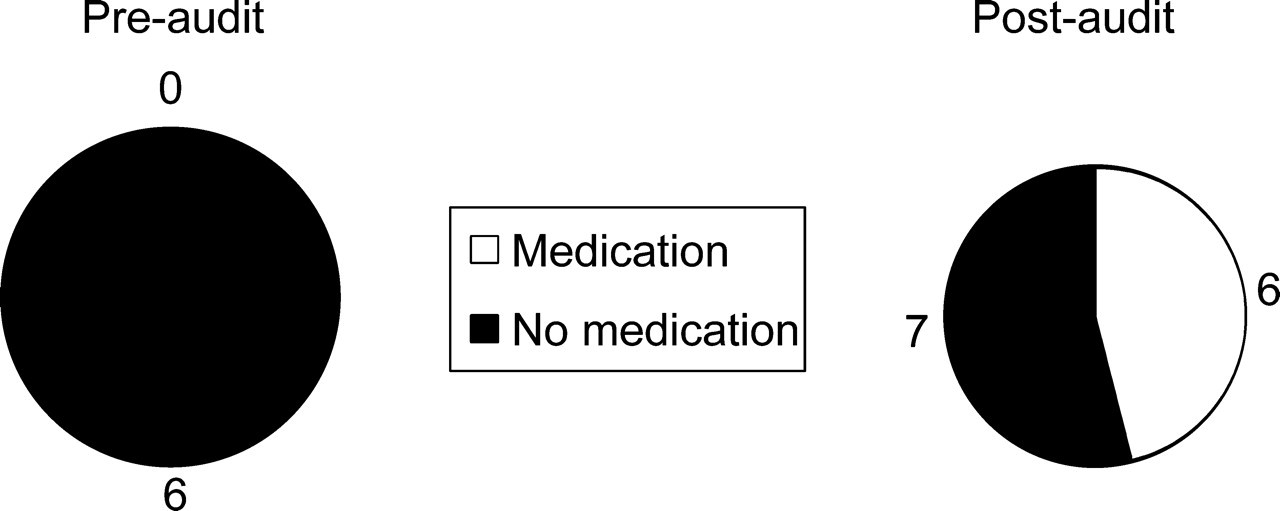
Patients prescribed anticholinergic for respiratory tract secretions pre- and post-audit
Experiential findings
Care homes can be appropriate settings for the provision of good quality palliative care, provided there is an understanding of the principals of palliative care among nursing home staff and access to specialist palliative care services when required. 5 The project has undoubtedly raised care home nurses understanding of the principals of palliative care through education on the ICP.
The project coordinator had spent two years working closely with the care home sector across south-east Wales and has found key comparables with regard to barriers to the successful implementation of the ICP. Where a care home had a consistent or established nurse/matron/manager, the coordinator found building working relationships to be more productive.
In five of 29 (17%) ‘champion homes’, the matrons have moved on from their post since the project began. Three of those matrons are now matrons in other care homes across the network area, one has retired and one has resigned. This supports findings from the ‘education needs analysis’, whereby it was found that even if care home staff change jobs they often remain within the care home sector. One of the ‘champion homes’ has had four matrons since the project began; another has been without a matron for many months.
In the homes without a constant lead, the coordinator found uptake of education poor and where education has taken place there has been no evidence of ICP usage. In these instances, the only follow-up on ICP understanding and usage has been one-sided, i.e. from the project coordinator.
The matron is for the most part, the coordinators' ‘link nurse’ within the care home for taking the lead in organizing the staff for training and encouraging the use of the ICP.
For successful implementation of the ICP, the coordinator has found that care home nursing staff must feel confident about their skills at recognizing when a patient is in the dying phase. Exploring issues around recognizing the dying phase has been found to be very useful for the staff. Many have said that they feel more empowered and ‘less apprehensive’ about discussing issues regarding the end of life of their patients.
The coordinator found a large part of discussion in the education sessions focused on the difficulties care home nurses face with the dementia/general frailty illness trajectory, and it was clear that the care home nurses were the best placed to recognize when a patient is dying.
The lack of protected time for education has been highlighted by some as a barrier to implementation, but the coordinator found that by having a learning contract with the care homes involved and by delivering the sessions in the individual care homes, only a few sessions were cancelled.
Some of the community-specialist palliative care teams have an established link with some of the care homes and ongoing education/training could be built up to encourage/sustain ICP usage.
These experiential findings are comparable with a survey carried out by Froggatt et al., 6 in which they found through a survey of 730 community-specialist palliative care nurses that although 92% of them had worked with care homes, the work was primarily reactive and undertaken infrequently.
In the pre-audit there was documented evidence of community palliative care specialist nurse input in 10 patients (8%). In the post-audit there was documented evidence of input in eight patient's records (6%). Care home staff would welcome and benefit from closer ongoing long-term collaboration with their community palliative care clinical nurse specialists.
Conclusions and recommendations for the future
The re-audit demonstrated an improvement in the recording of end of life care. The All-Wales ICP use has increased from 3 to 31% in one year.
Where the ICP was used in the post-audit, there was a reduction in the hospital deaths as demonstrated in Figure 8 in Cardiff, Vale of Glamorgan and Blaenau Gwent (also noted in Rhondda Cynon Taff where there was no ICP document available to use, but the principles of the ICP were adhered to).

Percentage difference between pre- and post-audit hospital deaths in relation to integrated care pathway (ICP) usage. Increased ICP usage demonstrates decrease in percentage of hospital deaths in Cardiff, Vale and Blaenau Gwent. (Although there was no ICP document in use in Rhondda Cynon Taff [RCT] it was clear in some records that the principles of the ICP were adhered to.)
There remains poor documented evidence of communication between care home staff, patients, relatives, GPs, hospital staff and other involved professionals. The pre- and post-audit demonstrated poor recording of care.
The care homes main link for expertise/specialist advice is through the GP, but it is widely recognized that the support and advice received can be inconsistent. The palliative care educational needs of GPs should therefore also be addressed if appropriate end of life care is to be provided for all care home patients across the network area.
Care home patients should have the same access to specialist palliative care teams as other patients. This can be achieved through formal liaison, ongoing education and an increased presence/contact of teams in the care home sector.
The project coordinator will ensure that by the end of the project every care home involved has a named community palliative care clinical nurse specialist with clear guidelines for referral. This will be achieved through collaboration with the teams.
There also remains the ongoing issue for the care homes of accessing the ICP document. One of the 10 LHBs has an electronic version of the ICP that provides easier access for the care homes. The project coordinator will clarify ongoing access of the ICP for the care homes in the forthcoming months, ensuring that a system to sustain usage is set up.
Care homes would greatly benefit from ongoing education on the foundations in palliative care incorporating use of the All-Wales ICP for the last days of life.
The biggest challenge will be sustaining ongoing use of the ICP; the project has a lifecycle of 10 months remaining in which time systems to sustain usage will be addressed.
This will include formalizing work with Care and Social Services Inspectorate Wales (CSSIW) to influence the care of the dying standard incorporating use of the ICP further enforcing the WHC 030 to endorse implementation.
The project will circulate project recommendations at the end of the project cycle in October 2008.