
Abstract
The European Quality of Care Pathway (EQCP) study is the first, international, cluster randomized controlled trial launched to study the effect of the implementation of care pathways and to study why and under what circumstances pathways work. The study will be performed in Belgium, Italy, Ireland and Portugal and will include individual studies: a trial including chronic obstructive pulmonary disease patients, a trial including proximal femur fracture patients and a trial focusing on multidisciplinary teamwork within both populations. The study is managed by the European Pathway Association in close collaboration with a multidisciplinary team of the Catholic University Leuven (Belgium), the University of Eastern Piedmont (Italy), the National School of Public Health Lisbon (Portugal) and the Health Services Executive in Dublin (Ireland). This paper will describe the history, project management and overall approach of this international study.
Introduction and objective
This paper will describe the history, project management and overall approach of the European Quality of Care Pathway (EQCP) study. The paper will not focus on the theory and concept of care pathways as such, but will explain the theory, international interest, practical and fund-raising issues based on which the project was launched and is organized, in order to support clinicians, managers and policy-makers in their search to improve research and evidence on pathways.
History
The European Pathway Association (E-P-A) was launched in 2004 and became an official international not-for-profit association in 2008, with its primary goal being to perform research on care pathways. Although interesting publications on pathways are published in international peer-reviewed journals, there is still confusion about the concept and, more importantly, the effect of implementation of a care pathway. 1
The E-P-A performed an international survey on the prevalence and use of pathways in 23 countries in 2005. 2 The conclusion of this survey was that pathways were predominantly viewed as a multidisciplinary tool to improve the quality and efficiency of evidence-based care. Care pathways were also used as a communication tool between professionals to manage and standardize outcome-oriented care, but were not always followed up with valid process and outcome indicators. There was need for knowledge sharing with regard to the development, implementation and evaluation of care pathways. 2
In December 2005, the E-P-A organized a consensus meeting in Ljubljana Slovenia to discuss the definition of pathways. Based on this consensus meeting with international experts, an overview paper on defining pathways, 3 the conclusions of the international survey 2 and multicentre research studies, 4–6 the E-P-A actually defines a care pathway as ‘A complex intervention for the mutual decision making and organization of care processes for a well-defined group of patients during a well-defined period. Defining characteristics of care pathways include: (i) an explicit statement of the goals and key elements of care based on evidence, best practice, and patients’ expectations and their characteristics; (ii) the facilitation of the communication among the team members and with patients and families; (iii) the coordination of the care process by coordinating the roles and sequencing the activities of the multidisciplinary care team, patients and their relatives; (iv) the documentation, monitoring, and evaluation of variances and outcomes; and (v) the identification of the appropriate resources. The aim of a care pathway is to enhance the quality of care across the continuum by improving risk-adjusted patient outcomes, promoting patient safety, increasing patient satisfaction and optimizing the use of resources. 4
From 2005 onwards, several lead members of the E-P-A gave presentations, workshops and teaching courses on pathways to explain the international differences and opportunities and to discuss the concept of pathways as complex interventions. During one of these events, a Health Forum in 2007 organized by Pfizer Belgium, four members of E-P-A (authors JP, WS, MP and KV) presented to Belgian health policy-makers, the opportunities and bottlenecks of pathways for the future of health-care management. The lack of sound evidence on the effect of pathways made Pfizer Belgium decide in 2007 to support E-P-A with an unrestricted educational grant to perform research on pathways. Pfizer Belgium convinced their colleagues from Pfizer Italy, Pfizer Ireland and Pfizer Portugal in 2008 to support this initiative. With these unrestricted educational grants E-P-A was able to launch the first international prospective research study on the effect of pathways in Belgium, Italy, Ireland and Portugal. The unrestricted educational grant provides the E-P-A autonomy and intellectual property regarding the methodological issues, the choice of the patient groups and the possibility of involving different academic institutions and contact persons.
Project management
The EQCP study was launched at the end of 2007. The E-P-A asked an emeritus professor in health-care management and policy, Leuven University, and adviser to the E-P-A (author JP) to chair the steering committee of the study and take the lead in contacts with Pfizer. The E-P-A council appointed the Center for Health Services and Nursing Research, Faculty of Medicine, Catholic University Leuven, Belgium, and the Department of Clinical and Experimental Medicine, Faculty of Medicine, University of Eastern Piedmont ‘Amedeo Avogadro’, Novara, Italy, to lead the scientific part of the study. Between the two universities an international multidisciplinary research team was built including medical doctors, a clinical nurse specialist, health-care managers, policy-makers, researchers and biostatisticians. This research team has more than 10 years of both practical and academic experience with care pathways. The team includes three PhD students (authors SD, CL and FL).
Within each of the four participating countries (Belgium, Italy, Ireland and Portugal), a national coordinator was appointed and a partnership agreement between an institution and the E-P-A was signed. In Belgium the Catholic University Leuven is supported by the Flemish part of the Belgian Dutch Clinical Pathway Network. 7 In Italy the University of Eastern Piedmont is supported by the AReSS Piemonte (Agenzia Regionale per i Servizi Sanitari). 8 In Ireland the Health Service Executive is taking the lead as national coordinator 9 and in Portugal the National School of Public Health in Lisbon is organizing the study. These national coordinators organize the study and are the main contact persons for the participating hospitals and multidisciplinary teams in their country.
Approach
A care pathway is explicitly defined as a complex intervention. 1,4–6,10–13 Complex interventions are those that include several components, those that have been made up of various interconnecting parts, or those that have been built up from a number of components that may act both independently and interdependently. 14,15 Many health service activities should be considered complex. 15 The evaluation of complex interventions is difficult because of problems in developing, identifying, documenting and reproducing the intervention. 14 The Medical Research Council of the United Kingdom defined five phases in research dealing with complex interventions: 14 (i) the preclinical theoretical phase, which explores the relevant theory to ensure the best intervention and hypothesis is chosen and to predict major confounders and strategic design issues; (ii) the modelling phase, which identifies the intervention components and the underlying mechanisms by which these components will influence outcomes (this will provide evidence about the predictability of how components and mechanisms relate to and interact with each other); (iii) the exploratory trial, which describes the constant and variable components of a replicable intervention and a feasible protocol for comparing the intervention with an appropriate alternative; (iv) the definitive randomized controlled trial (RCT), which compares a fully defined intervention with an appropriate alternative using a protocol that is theoretically defensible, reproducible and adequately controlled in a study with appropriate statistical power; and (v) the long-term implementation phase, which determines whether others can reliably replicate an intervention and results in uncontrolled settings over a longer term. Campbell et al. 14 recommended a parallel approach that combines preclinical and modelling phases with the goal of understanding the problem, intervention and evaluation. Based on the results of a first exploratory trial, researchers must conclude whether organizing and investing time and money in a randomized trial is worthwhile. In 2007, Campbell et al. 15 recommended conducting simultaneously the first three phases to better understand the problem, intervention and evaluation. The international research team of Leuven and Piedmont University have performed phase one, two and three studies over the past 10 years. Piedmont University even has experience with phase four studies. 5,6,12,13
With the EQCP study, the E-P-A launched the first international cluster RCT (cRCT) on the effect of care pathways on the compliance to process indicators and performance to outcome indictors. Next to the effectiveness, the E-P-A is interested in understanding why and under what circumstances pathways lead to their effect. Therefore the EQCP will combine a cRCT with a realistic evaluation approach as suggested by Pawson and Tilley. 16 This approach is closely linked with Donabedian's structure–process–outcome framework as described in ‘The Care Process Organization Triangle: a framework to better understand how pathways work.’ 17 This Care Process Organization Triangle is based on Donabedian, 18 Heskett et al. 19 Teboul, 20 Batalden and Davidoff, 21 Mitchell et al. 22 and Pawson and Tilley 16 (see Figure 1). In this triangle, the relationships between care process structure, multidisciplinary team processes and outcomes are described. Also within this triangle, gaps or chasms between these three cornerstones can occur more frequently than we thought 21,23 and these gaps could be important to understand why pathways sometimes lead to no effects or even negative effects.
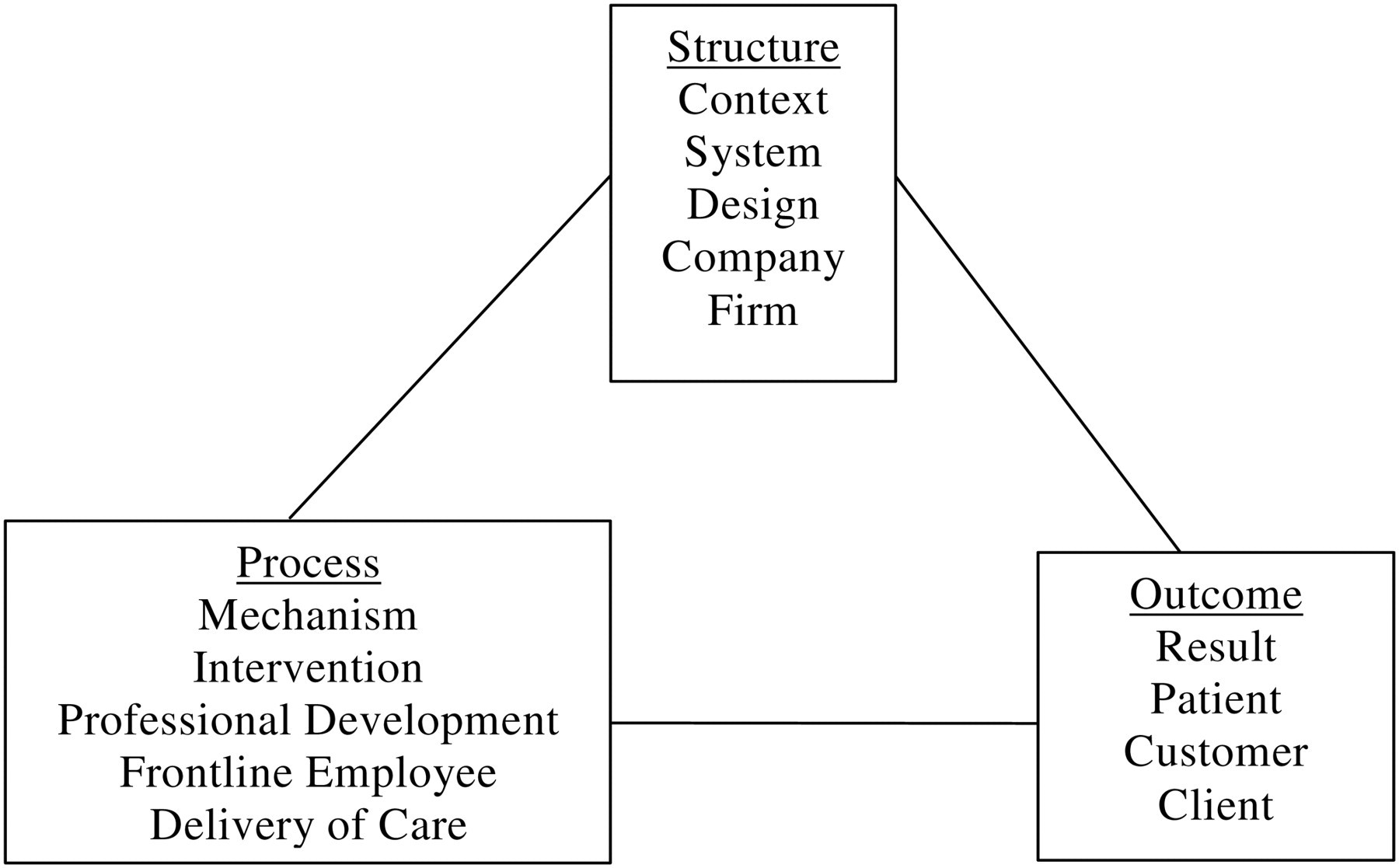
Care process organization triangle 17
Pawson and Tilley (1997) 16 define that an action is causal only if its outcome is triggered by a mechanism acting in a context (context + mechanism = outcome). They argue that programmes are effective only insofar as they introduce the appropriate ideas and opportunities (the mechanism introduced) to groups in the appropriate social and cultural conditions (the context or the environment). 16,24,25 Pawson and Tilley 16 concluded that the basic context–mechanism–outcome concern is still, of course, the outcome. Outcomes must be continuously followed up with evidence-based, risk-adjusted outcome indicators. 26 Well-organized mechanisms acting in well-structured contexts lead to appropriate outcomes, 16 although Berwick 25 and Goldman 27 describe that not all perfectly organized processes lead to improved outcomes. To fully understand these achieved outcomes of an intervention, knowledge of the mechanisms and structures, also known as the context, is essential. 25
To tackle the theoretical, practical and methodological concerns as described above, the EQCP study will consist of three closely related, but each of them unique, randomized trials: a study including patients hospitalized for exacerbation of chronic obstructive pulmonary disease (COPD), a study including patients with proximal femur fracture (PFF) and a study with the focus on multidisciplinary teamwork in both patient groups 28–30 (see Table 1). Based on the framework described in the Care Process Organization Triangle, 17 in each of these cluster trials the context/structure will be assessed using a set of team structure and organizational measures. The set of team structure indicators will be exactly the same in the three trials. Second, a set of process indicators measuring the multidisciplinary mechanism or delivery of care will be followed up. Third, a set of outcome indicators measuring the effect of the process acting within the context will be analysed (see Table 1).
The European Quality of Care Pathway Study approach
*The same set of team structure indicators will be used in the three trials
The indicators that will be used in the three studies will be developed based on systematic literature reviews, information of previous pathway research, international Delphi studies and expert consensus meetings to obtain a valid and reliable evidence-based set. For the process and outcome indicators in the COPD and PFF trial, the E-P-A has a partnership agreement with the Map of Medicine®, which provides evidence-based information for the care processes.
Discussion
Although the intervention will be thoroughly prepared, described and standardized, the multidisciplinary teams of the involved hospitals in the experimental group will have degrees of flexibility while implementing the care pathway within their own organization. Also, differences between the cultures within and between the involved countries could have an impact on the compliance to the key interventions and the performance to the outcomes.
How the randomization will be performed and how the intervention will be built up will be published in the study protocol and future publications of the study. Organization and quality of the care processes of all experimental hospitals will be evaluated and subsequently a care pathway will be implemented based on a set of evidence-based key interventions and the available benchmark data of the evaluation of the care processes. The hospitals will appoint a pathway facilitator to support the multidisciplinary teams. This person will be trained by E-P-A in the development and evaluation of care pathways. The facilitator will help the multidisciplinary teams in providing patient and organizational data. Pathway facilitators will share knowledge with their national colleagues during the training activities and thereby further improve their know-how. The involved hospitals will become part of an international network on clinical and organizational appropriateness for COPD and PFF processes. The participating hospitals will become a centre of excellence on the organization of care processes.
All participating multidisciplinary teams provide data on the quality and efficiency of the care process for a sample of patients. All teams will receive feedback on their own data and receive benchmark data with other national and international teams. Based on these data, the teams will be able to further improve the organization of their care process. Teams involved in this study will become part of a leading European network on COPD and PFF patients. The participating multidisciplinary teams will become centres of excellence in the development of pathways and will function as examples of good practice on the national and international level.
The research team will aim to publish the study protocols, the intervention, the effects of the three studies and the policy implications of the overall EQCP study in international peer-reviewed journals and aim to share all obtained knowledge with the international pathway community. The E-P-A will provide updates of the study on its website and during its yearly international conferences.
Conclusion
The organization of care processes has received increasingly more attention from both clinicians and managers. Although the effect of care pathways on patient outcomes is thoroughly described in the literature, consensus on their efficacy is still equivocal. There is a growing need to determine why pathways sometimes work and why they sometimes do not have the expected results. With the EQCP study including three cRCTs with respect to the Realistic Evaluation framework, the E-P-A is launching a study in Belgium, Italy, Ireland and Portugal on the effect of pathways and to understand why and under what circumstances pathways work.
Footnotes
Acknowledgements
We hereby thank the involved people and organizations: Prof Dr Paulo Boto and Rita Veloso-Mendez of The National School of Public Health, Lisbon, Portugal, Antoinette Doocey and William Reddy of the Health Services Executive, Dublin, Ireland, Dr Domenico Tangolo of the AReSS Piemonte, Italy and the Map of Medicine in London, UK. A special thank you goes to Pfizer Belgium, Pfizer Italy, Pfizer Ireland and Pfizer Portugal for the unrestricted educational grants.