
Abstract
The total number of hip and knee arthroplasties has been increasing steadily in the USA every year. The University of California Irvine recognized a high volume activity that could be improved with the implementation of clinical pathways. Data collection was obtained by monitoring the clinical path on 138 patients. Baseline preoperative data and telephonic postoperative data were collected at 90 days postdischarge utilizing quality-of-life/functionality validated tools. Clinical path utilization was 100%. Ambulation day 1 was at 80% for hips and 85% for knees. Blood transfusions were at 56% for hips and 36% for knees. These percentages are well above the US national reported value for autologous blood transfusions of 30%.
The short form 36 health survey questionnaire (SF-36) and Western Ontario and McMaster Universities Osteoarthritis Index (WOMAC) preoperative and postoperative data were available on 47 patients (35%) at 90 days. The WOMAC osteoarthritis index showed a percent mean difference improvement of 82% (pre = 35.8, post = 65.3). The SF-36 revealed statistical significance in physical functioning, role physical, social functioning, bodily pain, energy/vitality and mental health. In conclusion, clinical pathways are a reliable measure of health care. Analysis of clinical path variance and functional outcomes provide the necessary data for making sound business/health-care decisions.
Introduction
The Joint Commission for Accreditation of Health Care Organizations and the Agency for Health Care Policy Research and Quality in the United States represent two of the contemporary forces that sustain the impetus to examine patient's clinical outcomes, both during hospitalization and postdischarge. Clinical outcomes management provides a mechanism to impact quality through intermediate and long-term outcome analysis. Several methodologies have been proposed and advocated to manage care, 1–6 but the development and implementation of disease-specific clinical pathways has stood the test of time.
In 2000, more than 300,000 primary joint replacements were performed in the USA. This number increased to over 638,000 in 2003 and is expected to rise significantly. 7,8 Analysis of orthopaedic clinical path variances and functional outcomes has provided the necessary data for health-care providers to make sound business/health-care decisions that benefit both patient and provider in the care of these patients during the course of acute and postdischarge environments. 9
The use of the clinical pathways in primary joint replacement surgery was instituted by the University of California Irvine Medical Center (UCIMC) in the year 2000 after identifying orthopaedic surgery issues related to the fragmentation of care, average length of stay (ALOS), cost per discharge and variation in practice. Prior to implementing clinical paths, patients were managed through physician orders, nursing standards of care and practice guidelines that were not formally coordinated. The objective of the study was to determine whether there were changes in the perceived psychological distress and physical function levels of patients who were managed via the clinical path.
This study provides an assessment of the effectiveness of clinical pathways in the acute environment and the impact on function and quality-of-life postsurgical intervention at 90 days postoperatively on joint replacement patients.
Methodology
Creation and implementation of orthopaedic clinical pathways
A review of the entire pre-, intra- and posthospitalization plan of care was conducted by an interdisciplinary team comprised of orthopaedic surgeons, anesthesiology, pharmacy, pathology, radiology, nursing, case management, decision support, information systems and physical therapy in the beginning of 2000. The evidence obtained to develop best practice clinical pathways, and clinical and financial benchmarking included the following sources: University of California expert physician practitioners; extensive literature search in primary joint replacement surgery; University Health Consortium, 10 Lahey Orthopedic Clinic, 11 Agency for Health Care Policy Research and Quality (AHCPRQ) 12 and Office of State Wide Health Planning and Development. 13
In addition to monitoring the ALOS and the absolute cost of these pathways, all clinically important aspects of the path were covered with the following key indicators: ambulation on day 1 postoperatively; pain management; return to operating room (OR); and the percentage of autologous blood transfusion. Clinical pathways were then developed for total joint replacement (Figures 1 and 2). Each patient was also given a path regarding their treatment in language interpretable by the patient.
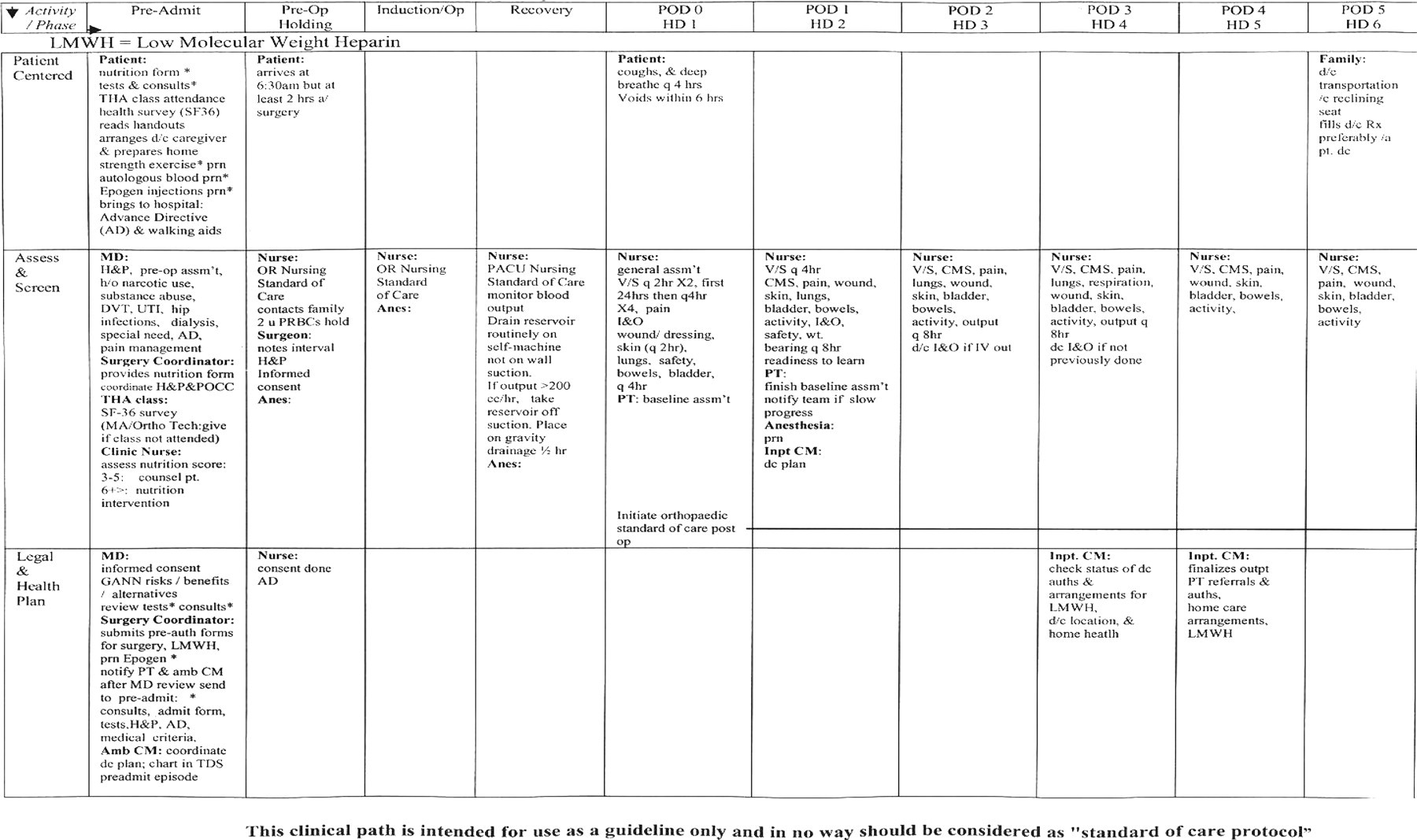
Example of page 1: total hip replacement

Example of page 2: total knee replacement
Developed pathways followed the appropriate approval process that involved the following committees: Pharmacy and Therapeutics, Risk Management, Performance Improvement, Medical Executive Committee and the University Governing Body. The clinical path physician order sets were built into the patient clinical documentation system (E7000 Eclypsis, Atlanta, GA, USA). Data acquisition was achieved through the interface between the hospital's Decision Support System (financial and clinical utilization software system) and the Eclyspis system during 2001. Once the clinical path was accessed, a code was transmitted to the Decision Support Department. Education was conducted with all disciplines associated with the pathway. Caregivers attended mandatory, didactic sessions that were held for all shifts. The primary lead physician for the pathway educated all residents and attending MDs in addition to orthopaedic and surgical grand rounds. The sessions included instructions on how to use the pathway; key clinical indicators; and how data would be collected and analysed. The pathway was then piloted on the orthopaedic unit for a period of 60 days to acquire care provider input. At the conclusion of 60 days, the clinical pathways were implemented.
Postoperative measurement at 90 days: SF-36 and the WOMAC
Patients were interviewed postoperatively at 90 days beyond hospitalization utilizing validated Quality of Life Functional Outcome questionnaires. A trained researcher, scripted, placed all telephone calls to patients.
After obtaining Institutional Review Board approval, patients were evaluated using the Western Ontario and McMaster Universities Osteoarthritis Index (WOMAC) and short form 36 health survey (SF-36) questionnaires. These questionnaires were administered at the same time by the orthopaedic clinic assistant preoperatively. The SF-36 is an available, validated survey tool that is sensitive enough to detect pain, functionality and overall quality of life, and it was selected by the institution to measure external orthopaedic outcomes. 14–16 In addition to the SF-36, WOMAC was selected as an equally reliable tool that is disease-specific for osteoarthritis patients undergoing hip and/or knee surgeries. 17–19
The WOMAC addresses clinically important symptoms in the areas of pain, stiffness and physical function in patients with osteoarthritis of the hip and/or knee. WOMAC consists of 24 questions with the following main categories: pain, stiffness and physical function. Patients were contacted at 90 days postoperatively, via phone by a graduate research student and interviewed using the standard set of questions at each follow-up. Data were directly input into an access database to track patients. Patients also answered questions pertaining to their level of satisfaction with the joint replacement class as it relates to their degree of preparedness for postoperative pain management and exercise (results are not shown). The corresponding categories were minimally, moderately or well-prepared for hospitalization. Over 95% responded that they were well-prepared for the hospital, but not as prepared for the discomfort level following surgery. Preoperative measurements were performed on all patients and postoperative measurements were performed at 90 days for this study report. Both questionnaires can also be utilized at six months and one year (results not reported here).
WOMAC scales are closely associated with the patient's own clinical path given prior to hospitalization. The WOMAC scale was reviewed during the clinical path development process to ensure a similarity between pre- and postoperative expectations. This information reinforces the goals of the patient postdischarge (i.e. climbing stairs, bending, stooping, postoperative exercises and precautions). Based on our findings, we reached the conclusion that this tool provides the necessary link between the clinical path and patient outcomes.
Results
Descriptive data are expressed as percentages and means with standard deviations. Analysis of variance of the clinical pathways, for hospital measurement of care, along with results of the SF-36 and the WOMAC for postoperative scores at 90 days were used as measurement tools to evaluate the programme. Changes in the SF-36 and the WOMAC were calculated by the difference in the mean scores between baseline and 90 days.
Orthopaedic clinical pathways
To evaluate the pathway, 138 patients were followed for their progress while on the pathway. This included 79 total knee replacements (TKA) and 59 total hip replacements (THA). There were 31 (39%) men in the TKA group and 53 (90%) men in the THA group. The mean age of the two groups was 62 for TKA and 63 for THA. These patients underwent surgery from June 2001 to July 2002. Data were collected on these patients from the date their surgery was scheduled until the day of discharge.
Compliance to the pathway in the hospital was considered a marker for the success of pathway implementation. During the study period, a total of 138 patients (79 TKA and 59 THA) were followed for compliance to the clinical pathway during their hospital stay. The length of stay demonstrated 100% compliance to the predetermined ALOS for both hips and knees (ALOS was at 4 days for knees and 5 days for hips). Early ambulation is recommended on all postoperative patients, especially joint replacement. Postoperative ambulation day-1 was at 80% for hips and 85% for knees (Figures 3 and 4). An additional clinical indicator regards the use of morphine as the designated choice of analgesia for postoperative joint replacement as reported by the AHCPRQ. 9 The drug of choice for the pathway was morphine, which included the potential to improve quality of care due to sustained pain relief over a longer period of time and a reduction in cerebral irritation in the elderly population. Variance analysis demonstrated an average 25% use of meperidine (Demerol), rather than morphine for the 138 patients followed. Hospital wide education from the pharmacy resulted in ensuring a reduced utilization of Demerol to less than 2% of patients. Any use of Demerol was in conjunction with an adjunct to anaesthesia. Due to nation-wide scrutiny of the re-transfusion of autologous blood, it was determined that blood transfusions should be a major clinical indicator. The rate of transfusions, both autologous and allogeneic, was high (30% is the national benchmark) and an actual of 56% usage on hip replacement and 36% on knee replacement. These percentages were well above national guidelines for autologous blood transfusions of 30%. Only 9.4% (13 of the 138) of the patients receiving blood were within suggested guidelines. To address this issue, UCI Medical Center purchased a perioperative, autotransfusion system to maximize blood collection by providing uninterrupted salvage both intra- and postoperatively in a single autoinfusion set (OrthoPAT, Zimmer, Warsaw, IN, USA). Another key indicator tracked was the incidence of venous thromboembolism (VTE). Of the 138 patients during the study period, only one incidence of VTE was noted. Occurrence of VTE remained consistently lower than the US reported rate. 20 The low incidence is due to an aggressive prophylactic, low molecular weight heparin regimen beginning 18 hours postoperatively and continuing postdischarge for seven days. By analysing aggregated data from the clinical path, trends and patterns in care are identified, evaluated, researched and reported to the Orthopedic Department. Interdisciplinary action plans were developed and initiated in response to significant findings.
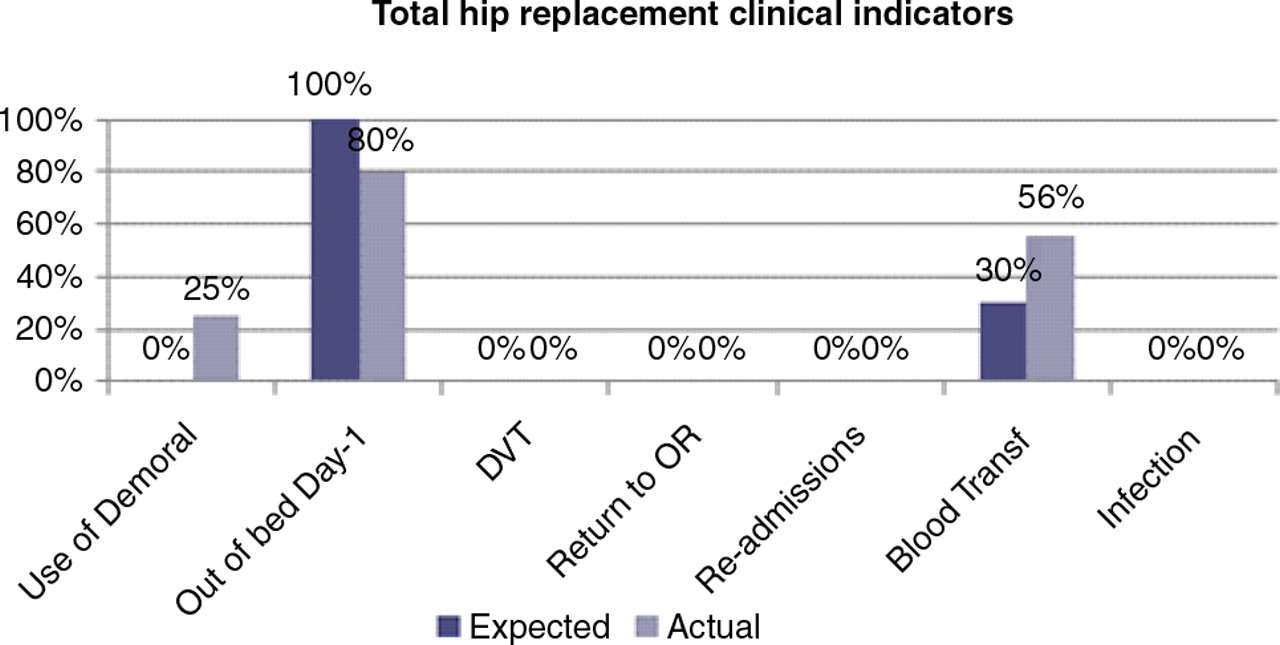
Clinical pathway: percent expected and observed total hip replacement clinical indicators (n = 59). DVT, deep vein thrombosis; OR, operating room
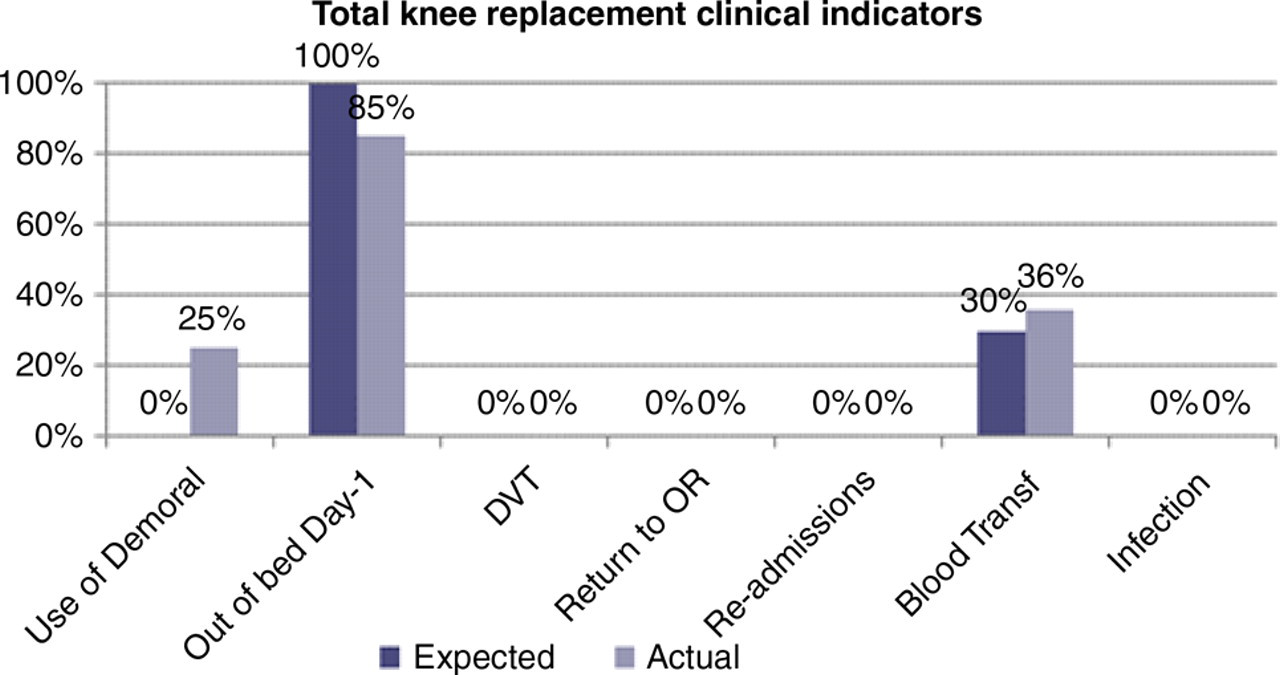
Clinical pathway: percent expected and observed total knee replacement clinical indicators (n = 79). DVT, deep vein thrombosis; OR, operating room
The cost of care on the clinical pathway was examined for the THA and TKA in relation to the benchmark data. THA achieved a reduction in cost per discharge of 6.97% (74 patients) and 5.22% for TKA (54 patients). These cost reductions are a result of clinical path monitoring and comparing the prepath cost to the postpath actual cost. The length of stay for knees met expectation, but hip ALOS exceeded expectation by 10.4%.
Postoperative measurement at 90 days: SF-36 and the WOMAC
To assess post-operative external orthopaedic and functional outcomes, SF-36 and WOMAC questionnaires were mailed at 90 days. Of the 138 patients followed on the clinical pathway, pre-operatively 47 (34%) completed the follow-up questionnaires at 90 days. Multiple phone calls were placed to contact the patients who did not respond to the mailed out surveys. The contact attempts were not successful which was determined to be due to the patients: change in telephone number; inadequacies in their phone voicemail system or lack of automated answering device; and change of address.
The SF-36 is divided into eight subcategories. These categories are as follows: physical functioning, role limitation due to physical problems, bodily pain, general health perceptions, vitality, social functioning, role limitations due to emotional problems and general mental health. Low numeric scores reflect an unsatisfactory perception of health, function and pain. High numeric scores reflect an improved perception with respect to health, function and absence of pain. For the functional quality-of-life outcome studies at UCIMC, raw scores were normalized to enable benchmarking with other studies. In conjunction with the SF-36, the WOMAC was used to evaluate pre- and postfunctional outcomes.
Subjective interpretation of pain and function, individual practice of analgesia, and discharge goal disparity between hips and knees were taken into account by the study coordinator in the patient interview.
SF-36 pre- and postsurgical scores: 90-day evaluation postsurgery
SF-36 = short form 36 health survey questionnaire
*Statistically significant P value
†Mean and standard deviation are shown
‡ P value for mean differences
For WOMAC, THA and TKA scores were combined due to low volume in either category. Data were collected and included baseline and 90-day postoperatively. WOMAC raw scores were transformed to normalized scores. WOMAC osteoarthritis index showed a percent mean difference improvement of 82% (pre = 35.8, post = 65.3) (Figure 5).
The Western Ontario and McMaster Universities Osteoarthritis Index (WOMAC) pre and 90 days postoperatively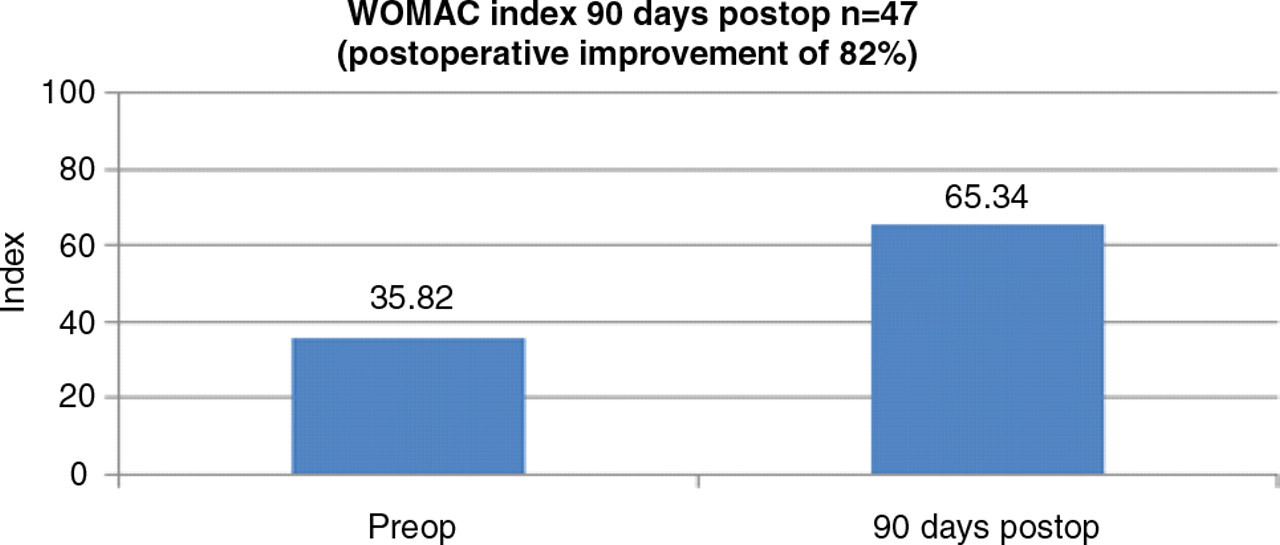
Discussion
The study results show that the utilization of the clinical pathway to manage care has demonstrated an effective method to monitor the process and content of care in orthopaedic surgery. Our pathways have shown that multiple disciplines can unite towards the achievement of goals directed at improved quality and financial stability for an institution. In accordance with some other studies, we concluded that pathways are a reliable tool that monitor the inpatient experience; provide realtime monitoring of multiple variances in the care delivery process and support accountability for outcomes of care. Pathways have been found to be superior to retrospective review and traditional quality assurance techniques. 21–24
We concluded that the clinical value of the SF-36 appeared marginal as it relates to medical decisions regarding the treatment plan, but remained as an indicator for early postoperative improvement. The SF-36 was chosen because it is not based on a ‘can do’ ‘can't do’ range of questions; however, it does examine domains of function, such as physical, social and mental. Global measures can remain stable and obscure real change if there is a gain in one domain (physical functioning) while there is a decline in another (social). It remains questionable if this instrument does have the sensitivity to detect subtle change. 25
Our study supported the WOMAC as a valid indicator of short- and long-term postoperative quality of life as it pertained to functionality. 18 One limitation of the study was associated with the values for pre- and postvitality scores that were confounded due to low volume and aggregating hip and knee scores together. The activity goals for functionality were more difficult to achieve for knee replacement surgery than those of hip replacement and were taken into consideration by the interviewer. Other limitations of the study were interviewer subjective interpretation of pain and function, and individual practice of managing one's own pain. Another limitation of our study is the percentage of non-responders. Despite our multiple contact attempts of patients who completed the baseline questionnaires, only 34% completed the 90 days follow-up. In a study by Norquist et al., non-responders had lower scores for social function and mental health summary on the SF-36. 26 Although follow-up outcome condition of the non-respondents in our study could not be determined, patients who are lost to follow-up are found to be different than those who continued to participate in a study. 26 , 27 This could reduce the generalization of the results and the data should be interpreted cautiously. However, this limitation is unlikely to influence the specific arguments of this paper.
Although we are pleased with the results of our study, reductions in average cost and length of stay, we should be cautious in attempts to further reduce length of stay. This could be harmful and even dangerous to the well-being of some patients, especially elderly patients.
The readers will note that the study was performed in 2002. Functional outcome measurement and clinical path utilization remain valid health-care measurement tools today as in 2002 for the following reasons: practice has remained unchanged; and the SF-36 and WOMAC remain the best available tools for both the public and health-care providers to access pre- and postoperative outcomes on joint replacement. Clinical paths continue to stand the test of time and are now required to be a designated Center of Excellence and/or a Joint Commission Certified Program. This study can be replicated in a variety of health-care delivery systems and has been adapted by other University Medical Centers.
Beside the development of an evidenced-based clinical path, the following are some of our study strengths: a reduction in length of stay; reduction in cost; improvement in postoperative pain control; early and appropriate interventions; and the continual provision of data to enhance medical practice and promote best practice.
We evaluated not only the cost of the development and implementation of our pathways, but also the components within the clinical pathway that would readily identify key clinical indicators carrying the highest chance of a negative clinical outcome, for instance, ensuring the application of sequential compression devices postoperatively in conjunction with evidence-based guidelines for anticoagulation therapy.
The clinical path strategy of managing care during hospitalization with a 90-day follow-up postoperatively has proven to be a consistent and structured programme. The programme's strength lies in its emphasis on the continuum of care concept where all aspects of patient care are directed towards the achievement of an optimal, clinical outcome. UCI Medical Center's commitment to outcome-based practice has been a segue into identifying other high volume, treatment-sensitive diseases. This practice provided the opportunity for caregivers to collaborate and stop the fragmentation in health-care delivery.
Footnotes
Acknowledgement
Saran Wilkins-Tucker, MPH, PhD, is acknowledged.