
Abstract
Summary
The differentiation of roles, tasks and responsibilities in health care has gradually increased because of efforts to decentralize, specialize and professionalize our health-care systems. These development approaches can on the one hand be regarded as successful, although there is also a negativeflipside. Increased differentiation has concurrently fragmented the delivery of health care, which, in turn, can be divided into structural, clinical and cultural fragmentation. Patients are lost as a result of these conditions of fragmentation. This phenomenon can metaphorically be described as a'Patient Bermuda Triangle’. Actions to dissolve the Patient Bermuda Triangles are commonly termed ‘Integrated health care’, a global buzzword that includes integrated care pathway as well as other integrated health-care strategies. Moreover, integrated care is a means to an end: improved patient outcome. To achieve this, it is crucial to have necessary prerequisites in place: both functional and interactional conditions. This procedure seems to be an organic process where the stakeholders go through gradual changes until the optimum level of integration, as well as mutualistic interactions, is established. If these conditions are concealed or impossible to achieve, developmental work should be ended to avoid the evolvement of antagonistic relations between the stakeholders concerned. This state will likely establish a Patient Bermuda Triangle or reinforce an existing one.
Increased differentiation of health-care services
Health-care systems all around the world are continuously developed to match changes in the demands and needs of stakeholders. Common effects of these development actions are, in brief, increased differentiation of roles, tasks and responsibilities in health care. There are three gradually reinforced and rooted conditions behind this outcome: decentralization, where extensive responsibilities and authorities have been placed in the frontline of organizations; specialization, where health-care personnel have developed in-depth knowledge in an ever-decreasing area; and professionalization, where health professionals work independently and with individual responsibility towards the patients. 1
The aim of the paper is to further explore this differentiation of health-care services; its positive effects as well as the flip side with increasing fragmentation of services. There is a growing interest in compensating for fragmented provision of health care by promoting different forms of counterbalancing concepts founded on simultaneous differentiation and coordination of services. The paper also aims at describing key issues and fundamental prerequisites for such integrating models.
Decentralization
There have been calls for rationalization of health care during the last decades due to tighter economic conditions. Different strategies have been employed for this purpose. The 1980s was the start of an extensive decentralization of most health-care organizations, which involve delegation of responsibilities to a lower organizational level, deconcentration of activities to an increased number of units, devolution of power to lower political levels and privatization of former public production. 2 Nearly every Western healthcare system, regardless of if they are of Beveridge or Bismarck type, embodies a hybrid of these four categories of decentralization. 3 Moreover, two of these categories: deconcentration and privatization, sometimes switch back and forth, while the other two seem to be more established. The extent of privatization seems to be linked to party-political circumstances, while the concentration of activities by two fewer units, by mergers or closures, often stem from a conviction that the economy of scale theory is adaptable in health care, which however is not an evidence-based approach. 4
The rationale behind decentralization is usually regarded as attractive because it brings decision-making closer to the health-care staff. A decentralized organization can thereby be more flexible and innovative than centralized institutions in response to local needs and conditions. Furthermore, it can be more effective than a centralized organization, as the frontline workforce has better ability to identify local problems and opportunities. 3 Decentralization can thus be seen as an option to provide health-care services in a more cost-effective way. As a consequence of this strategy, extensive responsibilities, including budgetary tasks, are shifted to frontline managers: physicians, nurses and other health professionals. In this connection, sense of economy and awareness of costs within the frontline of health-care organizations are increased.
Specialization
Parallel to the decentralization process, but with a somewhat earlier start in the postwar period of the 1940s, there has also been an accelerating specialization of health care. For instance, in 1960, Swedish health care contained 29 official clinical specialities. Today almost 60 specialities are included in the official classification. In addition, most clinical specialities are internally divided into subspecialities and also differentiated into levels of specialization, where general skills and knowledge on local level are supplemented by rare specialist competences on a regional level, and sometimes also on a nation level, of the health-care delivery system. Country of origin disregarded, the increased specialization is predominantly due to clinical development, whereby health-care personnel need to acquire more in-depth medical knowledge in an ever-decreasing area. This development is reinforced by more and better-informed patients demanding specialist treatment for their recovery.
Professionalization
Professionalization embodies the principles of professionalism, which is founded on autonomy and self-regulation in setting standards of practice, the content of education, and entry into and exit from the profession. As a result of this development, vast responsibilities have been placed on physicians and other professional groups, and they are working with great independence towards their patients. If anything goes wrong, these professionals risk their certificates, or could get reprimands from the authority of supervision. The health-care executives are rarely held responsible in these situations.
According to Abbot, the focus of a profession is its work and not its organization. 5 Furthermore, in a professional organization there is usually also competition for power and influence between the different professional groups. Professional groups therefore principally disallow management by an outsider. An accepted manager thus usually has to have the same profession as those being managed, and the person concerned also needs to give proof of high-quality professional skills. 6
Besides preserving professional autonomy, professionalization tends also to create professional organizations of management, 6 which in these cases will be founded on the structure of specialization, the criterion for the division of decentralization. Thus, in time with increasing differentiation of the health-care services, professionals have become more and more involved in management along with their professional duties. Moreover, in organizations guided by New Public Management principles this development has become more manifest.7,8
The Patient Bermuda Triangle
The outcomes of these three developmental approaches can on the one hand be regarded as success stories. Decentralization is commonly regarded as a successful condition to rationalize activities. Clinical specialization has undoubtedly promoted the health of populations. Furthermore, professional organization of management is today deeply embedded in health care. On the other hand, there is also a flipside of these demandable developments.
Decentralization is reinforcing a local identity and rationality 9 which may lead to suboptimizations at the expense of the overall organizational effectiveness. Thus, the personnel may be concerned with carrying out their tasks in the right way, but not equally concerned with whether they are carrying out the right tasks. Moreover, the specialization of health care has an influence on the formation of health care. Throughout, big departments have been divided into smaller specialized units of common structure. Health-care organizations have thus become more differentiated, but at the same time not more dissimilar to one another. If this standardizing of organizational formation has led to increased efficiency or not has rarely been considered.
According to Lawrence and Lorsch, 10 differentiation implies differences in culture and also in behaviour among groups or units. The organizational culture of health care is strongly influenced by values and ethics of the professional domain. It is thereby difficult to establish and implement common visions and objectives that also include perspectives of the policy domain or the management domain. Interactions between these three domains are predominately incompatible due to each domain operating by contrasting principles. 11
Thus, all three driving forces, individually and together, have contributed to a state of differentiation with manifold negative consequences for the health-care system as a whole. This is often described as fragmentation, which can be defined as a state of differentiation without the integration that is required to achieve a unity of effort. 10 Furthermore, it can be divided into different categories, depending on the interaction between the three driving forces described (Figure 1).
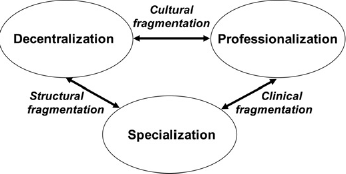
Fragmentation of health care and causal links to development
First, structural fragmentation makes it difficult to manage and organize between organizational units. This form of fragmentation is mainly a result of the adaptation of the decentralization of health-care organizations to the specialization process, where large departments are split up into smaller clinical units. An organizational configuration of this type is characterized by a high degree of autonomy for the different units, but a weak integration between them, which is additionally weakened if functional conditions like ICT, planning and financial systems, are not matched between the units concerned. Moreover, structural fragmentation is aggravated when health care is founded on different authorities. 12
Second, clinical fragmentation is primarily a result of the specialization in health care and its disintegrative pressures, where specialists get more and more encapsulated. 13 In addition, within a specific specialty there are variations in clinical procedures. 14 This can be explained by the professionalization of health care, accompanied by sovereignty of individual professionals and their sometimes reluctance to accept new evidence considering their own clinical experience. 15
Third, professionalization together with decentralization reinforces a cultural fragmentation that preserves ‘tribal values’, 13 which make it difficult to develop and share common values among the health-care personnel. Following the Domain Theory, 11 health-care professionals tend to do what they consider to be best for the patient and not what is beneficial for the organization as a whole. A health-care system can therefore have strong cultures, but it often lacks a common culture comprised of health-care professionals, health-care executives and policy-makers. 16
A fragmented health-care system is characterized by patients often being transferred to other departments or institutions without complete information about the patient's condition, medical history, services provided in other settings or medications prescribed by other clinicians. 17 These conditions may lead to waiting times and delays for the patients, and furthermore, duplications of tests causing additional costs to the health-care system. In this way, fragmentation may cause difficulties in the coordination of activities for patient treatment. Or, according to Berwick, 18 patients are lost due to the fragmentation of health-care delivery systems. This phenomenon can metaphorically be described as a ‘Patient Bermuda Triangle’ and illustrated as in Figure 2.
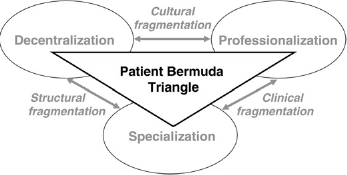
The ‘Patient Bermuda Triangle’: caused by a fragmented health-care system
Integrated care
Patients within the Bermuda Triangle are thus lost due to an incoherent provision of services by the health-care providers involved, which especially can happen to patients with manifold needs. This group contains the frail elderly, patients with chronic conditions and disabilities, as well as patients who require multiple clinical treatments of distinctive diseases or injuries. The approach to dissolve the Patient Bermuda Triangle is commonly termed as integrated care. This global buzzword has driven and shaped health-care systems to be more coherent and patient-centred. 19 At the same time, as is apparent from explorations of this widespread policy, integrated care lacks a common definition, and, furthermore, it includes several concepts. What they do seem to have in common is the striving for a counterbalance to fragmented health-care services. Moreover, these concepts are all regarded as means to an end: mostly improved quality of care. 1
The somewhat unclear perception about integrated care implies accordingly a variation of strategies, but also of appellations. Managed clinical network, transmural care, chain of care, shared care, case management and integrated delivery system are only few examples showing this variety of applications and designations. Integrated care pathway is yet another concept to be included in the extensive community of integrated care. This concept has a strong foothold in many countries all around the word, 20 and, furthermore, originally developed as a case management plan in 1985, which later evolved into the method CareMap. 21
The concepts of integrated health care could include integration within an organization: intraorganizational integration, for instance within a hospital department, and between organizations: interorganizational integration, for instance between hospital departments and primary care. This later form of integration is, for obvious reasons, more difficult to develop. Moreover, these forms of integration may include vertical integration, that is, between units on different hierarchical levels, as well as horizontal integration, that is, between organizational units on the same hierarchical level. 22 In addition, different forms of health-care integration are in practice mostly funded on interprofessional integration: joint working between health-care professionals. 19
Continuums of integrated care
According to Lawrence and Lorsch, 10 the level of integration should be correlated to the degree of differentiation of the health-care services; a high degree of differentiation implies a high degree of integration, and vice versa, in order to fulfil demands of other providers or the patients. In accordance with this argument, different forms of continuums have been proposed in order to describe the context of integration.
Hudson et al. 23 suggest a range from autonomous organizations and functions on one end, through cooperation and coordination, to fully integrated organizations and functions on the other end. Konrad 24 argues that integration is constituted by different levels of intensity: informal contacts, cooperation and coordination, collaboration, consolidation and full integration. Based on a study of integration in the USA and UK, Leutz 25 developed a similar typology of connection degrees between providers of services: linkage, coordination in networks and full integration. The latter mean that resources of the organizational units concerned are pooled together to form a new organization.
Ahgren and Axelsson 22 adapted these theories into a continuum of integration to be used in a clinical context, starting with full segregation followed by linkage, coordination, cooperation and ending up with full integration. Full segregation constitutes the absence of any form of contacts between providers of health care. In a health-care context, the stages between full segregation and linkage could be described as interspecialty contacts founded on referrals of patients. While clinical guidelines for specific patient groups, describing what shall be done by whom and when, are an example of linkage, coordination is about facilitating the transition of patients, comprised by clinical guidelines, between different health-care units. Integrated clinical pathways and other types of clinical networks are included in this form of integration, but there are usually no network managers appointed. The existence of such managers, as in the case of managed clinical networks, would entail a higher degree of integration, that is, cooperation.
Whatever continuum used, a high level of integration must not be interpreted as better than lower levels. The optimum level of integration varies between different services and units and depends solely on their need of integration. In some cases it is necessary to merge, while in other cases integration can be limited to loosely contacts between providers of services.
Integration synergy
The optimum level of interorganizational integration is a functional prerequisite to attain integration synergy: an overall improved outcome than if each unit was working towards the same objective separately. 26 It is important that health-care providers discover and recognize collaborative advantages of this kind; otherwise functional integration will be unimportant and should be avoided. 27 The development of functional integration could even be destructive when collaborative advantages are concealed or lacking. According to the theory of Health Care System Ecology, integrative arrangements founded on such conditions can turn into antagonism. That is, a condition in which the interaction between two health-care providers has an overall outcome which is less than the sum of their individual effects. Mutualism is the opposite relation, which could be described as an interaction between two providers where both derive decisive benefits. Furthermore, mutualism and antagonism could be viewed as opposite endpoints along a continuum of symbiotic effects. Commensalism can be placed on this continuum in between antagonism and mutualism. In practice, this is a relationship between two health-care providers where one benefits of the interaction while the other is unaffected. 28
Conventional interorganizational theory mainly focuses on functional arrangements, that is, how to organize between the organizations involved. Different kinds of environmental consequences are not always the centre of attention; for example what kind of symbiotic effects evolve by developing and implementing a health-care delivery network. Are determinants of development in place, like professional dedication and confidence, and legitimacy of the development work? 29 These conditions seem to be of vast importance to whether or not integrated health-care arrangements will be implemented and sustained. 28
Integration synergy thus seems to be dependent on both the functional formation and the symbiotic condition of integration. Establishing the optimum level of integration between two health-care providers is necessary if the synergetic effect shall be maximized. However, the lack of mutually recognized benefits of such an arrangement could, at the worst, evolve into an antagonistic interaction, which, in turn, implies a disadvantaged shift of focus; from core activities to the protection of boundaries. Hence, a health-care delivery network most likely marked by contra productivity and quality flaws. 28
Integration outcomes
An optimum degree of functional integration together with mutualistic process conditions will, according to the classical theory of Donabedian, 30 be in favour of best possible outcome; the ultimate aim of integrated health care. 19 However, outcome can be viewed from several perspectives, and it is therefore important to distinguish the final outcome, that is, the one in relation to a patient perspective. Other types of outcomes, like for instance those related to managerial or professional perspectives, are also important, but mostly for the understanding of dependency between different stakeholders. 31 For example, impact of managerial actions on professional condition, and of clinical performance on demand and choice among patients. Research has so far predominantly focused on these two perspectives, and there is accordingly a need to improve the knowledge about the final outcomes of integrated health care, that is, the satisfaction of the needs of the patients, for example, their recovery or rehabilitation. According to Haggerty and her colleagues, 32 it is only the patients who can really assess the extent of outcome satisfaction correlated to an integrated provision of health-care services, that is, if a Patient Bermuda Triangle exists, or if it is dissolved and replaced by a coherent health-care system.
Concluding remarks
According to the theories revisited, it is vital to have the necessary prerequisites in place: both functional and interactional conditions. The latter include determinants of developments like professional engagement. There are apparently no manuals for this work. It is instead more an organic process where the stakeholders go through gradual changes until the optimum level of integration as well as mutualistic interactions are established. Only at this complete stage is it possible to extract lasting full synergy of interorganizational integration.
On the other hand, if these conditions are concealed or impossible to achieve, the development work should be terminated to avoid the evolvement of antagonistic relations between the stakeholders concerned; a state which most likely establishes a Patient Bermuda Triangle or reinforces an existing one.
Creating an integrated care pathway, or another integrated health-care solution, thus seems to be more of an ‘art’ by engaging professionals and creating other favourable development conditions, than a predictable process founded on development work with a predetermined design. This kind of structural support can of course be helpful when the conditions are favourable, but it has low significance when the work is marked by doubts between stakeholders. In particular, there is a need to understand and take into account the mechanisms of professional behaviour to be able to replace fragmentation by integration, and thereby dissolve Patient Bermuda Triangles.